If you have any further questions, please telephone the department or discuss them with a member of staff on the day of your procedure.
What is a Gastroscopy?
Camera test down the throat
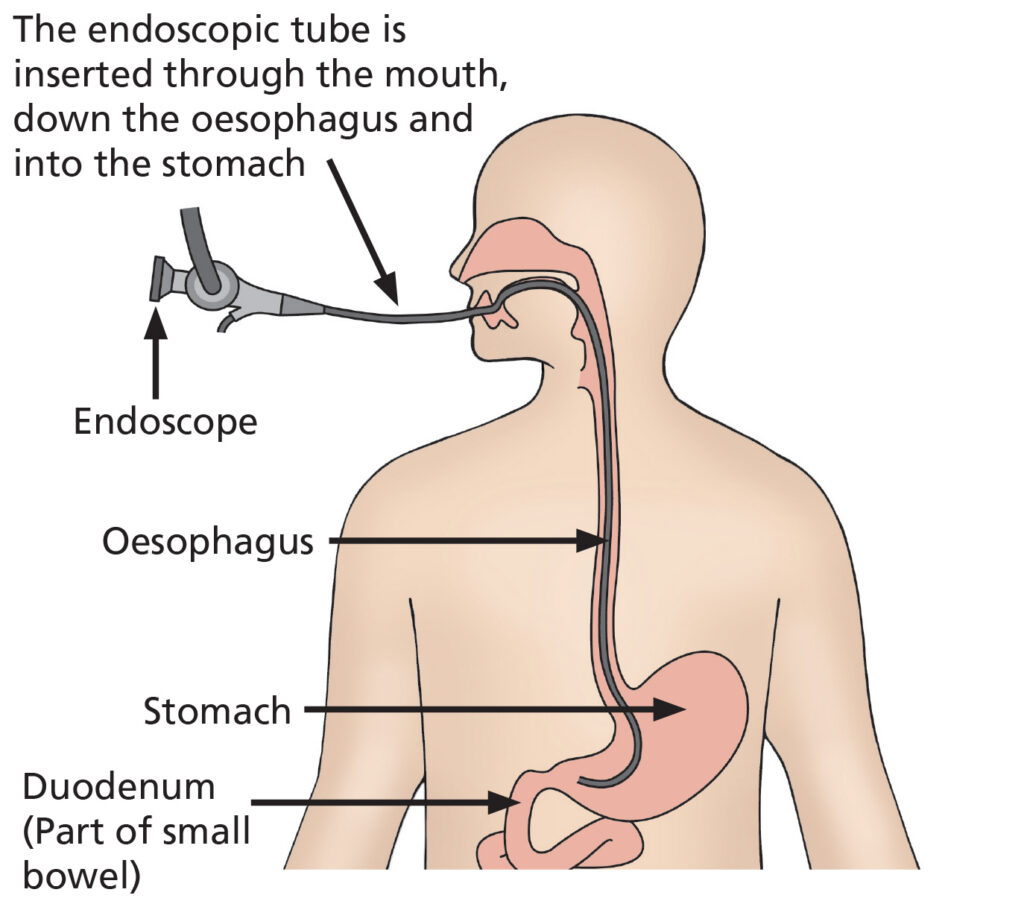
A gastroscopy is a test to examine the upper part of your digestive system – your oesophagus (gullet), stomach and duodenum (small intestine).
A flexible tube with a camera on the end is used for this procedure. Pictures from this camera are seen on a television screen by the endoscopist. The test takes between 5 and 20 minutes (depending if treatment is required). You can expect to be in the Endoscopy Unit about 1½ – 4 hours depending on whether you have sedation for your procedures.
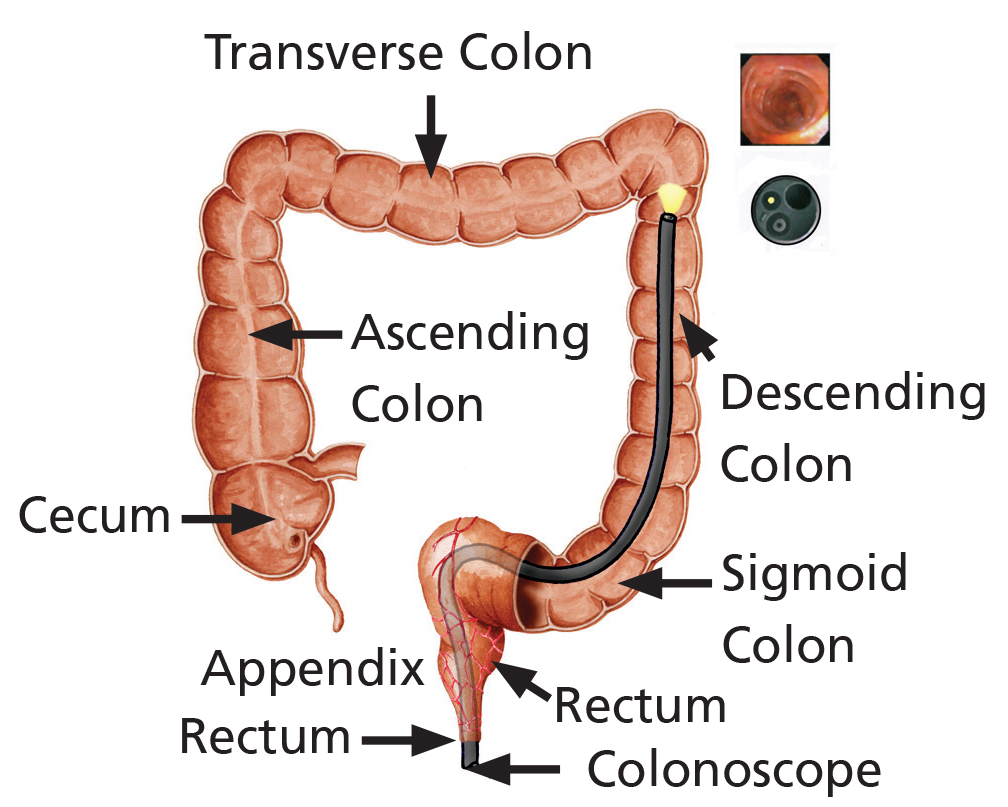
What is a Sigmoidoscopy?
A sigmoidoscopy is an extremely useful test that examines the lower part of your large bowel (colon). A flexible tube with a camera on the end is used for this procedure and is passed through the back passage and around the lower part of your large bowel. Pictures from this camera are seen on a television screen by the endoscopist. The test takes 5 – 15 minutes depending on how difficult it is pass the camera around the bends in your bowel.
Camera test for your large bowel
Why am I having a Gastroscopy and Sigmoidoscopy?
Your doctor has referred you for a gastroscopy and sigmoidoscopy to investigate the symptoms you have been having from your digestive system and bowel such as indigestion, heartburn, stomach pain, diarrhoea and change in bowel habit or bleeding.
During your gastroscopy and sigmoidoscopy, the endoscopist (doctor or nurse practitioner) may take a small piece of tissue (biopsy) to aid diagnosis. It may also be necessary to remove polyps from the bowel wall. Both removing polyps and taking biopsies is painless and is achieved by passing special equipment down the inside of the camera – you will not feel this. All tissue samples have to be sent away to the laboratory so the results will not be available straight away. You will be able to discuss the results of your biopsies with the doctor who referred you.
What are the benefits to having a Gastroscopy and Sigmoidoscopy?
A gastroscopy and sigmoidoscopy provides detailed information of the appearances of the lining of the digestive system and bowel. The information gained during your test may reveal a cause for your symptoms and will assist your doctor in your further treatment. If you prefer not to have a gastroscopy or sigmoidoscopy, we would advise you to discuss the implications with your doctor.
What are the alternatives to having a Gastroscopy?
There are other methods of examining the stomach such as a barium meal or CT scan. These methods; however, do not allow biopsies and photographs to be taken and provide less information about the lining of your digestive tract.
What are the alternatives to having a Sigmoidoscopy?
Another method of examining the colon is a CT scan. Although this test offers valuable information, it also provides less information about the lining of your bowel and does not allow biopsies to be taken or procedures such as the removal of polyps.
What are the risks of having a Sigmoidoscopy
The risks associated with your test are detailed on your consent form and below. Please read this. If you have any questions, speak to the nurse or endoscopist on the day, or alternatively, ring the Endoscopy Unit. Complications are rare but it is important that you are aware of them before the test begins. As with any medical procedure, the risk must be compared to the benefit of having the procedure carried out.
- Having a sigmoidoscopy carries a small risk of making a hole in the bowel wall (a perforation), this occurs in 1 in 1,000 examinations. Perforations usually need to be repaired with an operation and might require a temporary stoma (a surgical constructed opening that permits the passage of waste).
- If the endoscopist removes a polyp, then the risk of perforation, although still rare, increases slightly to 1 in 500 occasions.
- Bleeding from the back passage can occur after the test, especially if biopsies are taken. Bleeding is more common after a polyp has been removed. Bleeding usually stops without any treatment; however, occasionally treatment may be needed to stop this.
- Sedation is not often used during this procedure; however, if used sedation can cause affect your breathing. To reduce this risk, we monitor your pulse and oxygen level. The endoscopist may recommend that you don’t have sedation if you at a high-risk of breathing difficulties during the test. This often applies to patients with heart disease and breathing problems such as Asthma and Chronic Obstructive Pulmonary Disease (COPD).
What are the risks of having a Gastroscopy?
The risks associated with your test are detailed on your consent form and below. Please read this. If you have any questions, speak to the nurse or endoscopist on the day, or alternatively, ring the Endoscopy Unit. Complications are rare but it is important that you are aware of them before the test begins. As with any medical procedure, the risk must be compared to the benefit of having the procedure carried out.
- Having a gastroscopy carries a small risk of bleeding or making a hole in the digestive system (perforation). The risk of this happening is less than 1 in 5,000. Although this is a serious complication for which surgery may be necessary, it is rare.
- Using sedation can affect your breathing. To reduce this risk, we monitor your pulse and oxygen level during the test. If the endoscopist feels that you are at risk of breathing difficulties during procedure, they may recommend that you do not have sedation or may give you minimal sedation. This often applies to patients with heart disease and breathing problems such as Asthma and Chronic Obstructive Pulmonary Disease (COPD).
- Some patients can experience abdominal discomfort or bloating during the procedure. If this persists at home or you have signs of bleeding such as black tarry stools, you should contact your nearest Emergency department for further advise and also inform us.
- Other rare complications include damage to loose teeth, crowns or to dental bridgework.
What preparation will I need for my Gastroscopy and Sigmoidoscopy?
Gastroscopy must be performed on an empty stomach, your appointment letter will tell you when you will need to stop eating and drinking.
Before the start of your examination, you will need an enema to clean and empty the bowel. This ensures that the endoscopist can see the bowel lining clearly. An enema may have been sent to you in the post so that you can administer it at home (the instructions and enema will be with your letter). Alternatively, an enema will be administered by the nursing staff in the department. If you are unable to administer the enema yourself, don’t worry. Bring it with you to the Endoscopy Unit on the day of your appointment and one of the endoscopy nurses will do this for you.
Choosing how to have the test. What are my options?
Your gastroscopy will be the first test to be completed and takes 5 – 20 minutes. Many patients are concerned with the thought of swallowing the tube but we would reassure you that the test is not painful, you will be able to breathe normally and you will not choke. During the test, we have to inflate your stomach with air, some patients find this unpleasant.
Throat spray:
This involves numbing the back of your throat with local anaesthetic spray. You will be awake and aware throughout the test, the nurse taking care of you will talk to you throughout the test and tell you what to expect. If you choose this option, you will be able to have your sigmoidoscopy with some Entonox. If you are uncomfortable (see below), go home soon after your test as there are no after-effects apart from some numbness of the throat for up to 1 hour.
Sedation:
Sedation is not a general anaesthetic and will not put you to sleep; however, it may make you feel relaxed and possibly, a little drowsy. Sedation is a combination of Midazolam a sedative and Fentanyl a pain killer. Giving sedation is not always recommended for patients with breathing problems such as COPD and heart problems. Your endoscopist may recommend that you do not have sedation or give you minimal sedation if they feel you are at risk from complications.
Following sedation, you will have to rest in the recovery area so we can monitor your recovery from the sedative, this can take 1 – 3 hours.
Important
You MUST bring someone with you and also go home in a car / taxi, not on public transport as you may be unsteady on you feet due to the sedation.
Also, you must have someone at home to care for you for 24 hours and must rest indoors. This means no work, no driving, no alcohol and you shouldn’t operate machinery.
Sedation will not be given if the above are not arranged before the test is undertaken. If you choose to have sedation, this will still be effective during your sigmoidoscopy test.
There are known adverse effects from the intravenous drugs administered during the procedure, ranging from mild and common to rare and serious. These include: headaches, nausea, fainting, depression of respiratory and nervous system, which may result in aspiration pneumonia, anaphylaxis and coma. Although these serious complications are rare, they are common in patients with deeper sedation and / or general anaesthesia.
Entonox:
Entonox can be used during your sigmoidoscopy if you have had throat spray for your gastroscopy. For many people, a sigmoidoscopy is only slightly uncomfortable, you may feel cramp like discomfort as the camera passes around the bends in the bowel. This soon eases when the bend has been passed.
Entonox is the gas and air mixture commonly used in childbirth – it can help with the discomfort during your sigmoidoscopy. The gas is administered by a special mouthpiece which you hold yourself during the procedure. The Entonox gas works within 30 seconds and you may feel slightly lightheaded and sleepy.
You control the amount of gas that you have yourself by simply removing the mouthpiece but the nurse looking after you will monitor you closely throughout the procedure and make sure that you are using the gas successfully.
Entonox has some rare side-effects, these are mild nausea, dizziness and a dry mouth. As the effects of the Entonox wear off quickly so do the side-effects.
One of the benefits of Entonox is that when the procedure is over, the gas is rapidly eliminated from the body so you can usually leave the department soon after your procedure, if you feel well enough. You can drive 30 minutes after the test or use public transport as long as you feel back to your normal self. You will not need anyone to look after you.
Entonox is not suitable for everyone (particularly if you have COPD or a collapsed lung).
Please discuss the options available to you with the nurse and / or the endoscopist before your test. The endoscopist / nurse may advise you of the option that may be more appropriate for you considering your medical history.
Do I keep taking my tablets?
You must keep taking any essential tablets unless your doctor tells you specifically not to. Please take your tablets early morning with a sip of water if you have a morning appointment. If you have an afternoon appointment, please make sure that you take your medication 4 hours before your appointment or leave it until after your test.
Please telephone the Endoscopy Unit if you are diabetic, have sleep apnoea or are taking tablets that prevent blood clots. Examples of blood thinning tablets are Warfarin, Aspirin, Clopidogrel (Plavix), Dipyridamole (Persantin), Prasugrel (Efient), Ticagrelor (Brilligue), Acenocoumarol (Sinthrome), Rivaroxaban, Edoxaban or Apixaban.
If you are taking iron tablets (ferrous sulphate), please stop them 7 days before your test.
What should I bring on the day?
You may wish to bring your dressing gown and slippers. You will be asked to change into a hospital gown that is open at the back before your test.
Please bring a list of medication that you take and also any medication that you may require whilst in the department such as GTN spray, inhalers and insulin. Please do not bring valuables to the department or wear lots of jewellery. Please can you also ensure that you remove nail varnish as this interferes with the signal we receive from our monitors about your oxygen levels.
What will happen on the day of the test?
When you arrive at reception in the Endoscopy Unit, your personal details will be checked. The assessment nurse will collect you and take your medical history, discuss and explain the test and take your blood pressure and pulse. You will be able to ask any questions and discuss any worries or questions that you have about the test. You will be asked for your consent forms (supplied with this leaflet). This will be attached to your notes and taken to the procedure room.
Please make sure that you have read this through before you come for your test as when you sign this form you are agreeing that this is a test you want. Remember, you can change your mind about having this procedure at any time. The endoscopist will discuss the consent form with you.
Please note:
Every effort will be made to see you at your appointment time; however, due to hospital inpatient emergencies, delays may occur. The endoscopy staff will keep you informed of any delays.
What happens in the procedure room?
You will be greeted by two nurses who will remain with you during the test. If you have chosen to have sedation, a cannula will be placed in your vein so that sedation can be administered and you will be given oxygen through a small plastic tube in your nose. If you are having throat spray, your throat will be numbed. You will be shown how to use Entonox if you have chosen this option as well.
You will then be asked to remove any dentures or glasses and lay on a trolley on your left-hand side. All patients pulse and oxygen levels are monitored by a probe placed on your finger during the test. Before the test starts, a plastic mouthpiece is placed between your teeth to keep your mouth slightly open.
When the endoscopist passes the endoscope through your mouth, you may gag slightly – this is quite normal and will not interfere with your breathing. During the procedure, air is put into your stomach so that the endoscopist can have a clear view. This may make you burp a little, some people find this uncomfortable. Most of the air is removed at the end of the test. When the procedure is finished, the endoscope is removed quickly and easily.
After your gastroscopy is completed, the endoscopist will then begin your sigmoidoscopy. The endoscopist will initially examine your back passage with a finger to make sure it is safe to pass the camera and then introduce the endoscope into your back passage and guide it around your bowel. You may experience bloating from the air and a period of discomfort as the camera goes around a bend in the bowel. Usually, this will ease once the bend has been passed. Air can also be relieved by passing wind (this is normal and you must not be embarrassed as the endoscopist will expect you to do this). If you are finding the procedure more uncomfortable than you would like, please let the nurse who is looking after you know. You may also be asked to change position during the test e.g. roll onto your back to make the procedure easier and more comfortable.
Please note:
All hospitals in the trust are teaching hospitals and it may be that a trainee endoscopist performs your procedure under the direct supervision of a consultant, registrar or nurse practitioner.
What happens if a polyp is found?
One of the aims of sigmoidoscopy is to detect polyps. Polyps are growths that can occur on the bowel wall that can range in size. Some are perfectly innocent but others can slowly develop into bowel cancer if they are not removed. Removing polyps is a simple and painless procedure, this is termed a polypectomy.
What happens after the test?
You will be transferred to the recovery room after the test. The length of your stay is dependant on if you have had sedation or throat spray and Entonox.
If you had local anaesthetic spray only for your test, you can leave the department after the recovery nurse has checked your blood pressure. You will have to wait 1 hour before you have anything to eat or drink as the throat spray can make swallowing difficult. If you have had Entonox, you should be able to leave after 30 minutes.
If you have had sedation, the recovery nurse will monitor you during your recovery from sedation, this can take 2 – 3 hours.
Remember: if you have sedation, you will need an escort with you, transport home and someone to look after you for
24 hours after the test, you must not:
- drive a vehicle;
- drink alcohol;
- operate machinery; (This applies for sedation only)
- go to work; and
- sign legal documents.
The recovery nurse will prepare you for discharge home and give you after-care instructions. You may experience a sore throat and feel bloated due to the air left in your stomach. Both sensations are normal and should clear up quickly by themselves.
When will I get my results?
A full report will be sent to your referring doctor and your GP. The endoscopist or nursing staff will usually have the opportunity to speak to you after your test regarding the results. An appointment to see the doctor who referred you for the test will be sent to you in the post or given to you in the department. Any enquires regarding your outpatient appointment should be directed to your consultants secretary.
If you feel that you are waiting a long time for an appointment to discuss your results, your GP will also have a report so you can see them too.
This leaflet has been designed as a general guide to your test. If after reading this you have any questions that you feel have not been answered, please contact the Endoscopy department on the numbers below.
Contact us
Administration Team
For any enquiry about your appointment including cancellation. Also, contact this number if you require an interpreter or transport.
Nursing Team
Please contact this number if you would like advice on your medication, or any other medical question or worry.