You have been given this leaflet because you are a carrier of Sickle Cell Disease (SCD) and are pregnant.
The information in this leaflet will explain how we care for people with SCD during pregnancy.
What is sickle cell disease (SCD)?
It is a blood disorder caused by a difference in the red blood cell pigment, haemoglobin, which carries oxygen around the body.
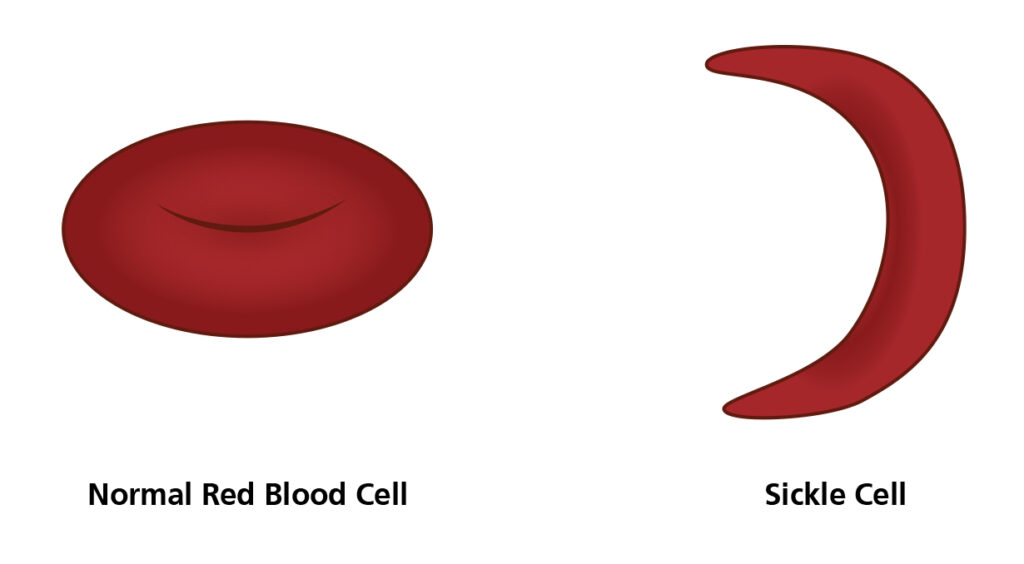
Normal red blood cells are round and flexible whereas in sickle cell disease, cells become rigid and crescent, or ‘sickle’ shaped.
These different cells cannot pass through blood vessels as easily, causing clogging of blood vessels. This is associated with episodes of pain, known as ‘crisis’.
The different cells are broken down by the body but not replaced quickly enough, leading to a shortage of red blood cells and haemoglobin, known as ‘anaemia’.
What causes sickle cell disease?
SCD is a genetic condition. It is caused by an difference in the gene that codes for haemoglobin. Everyone has two copies of the haemoglobin gene, one gene is inherited from your mother and one is inherited from your father. If a person has two of the different genes it will lead to the development of sickle cell disease.
Some people may have only one different gene and one typical gene, these people are known as ‘carriers’ or as having the sickle cell trait. Carriers will not develop sickle cell disease and are well in themselves, but there is a chance that they could pass the different gene on to their children.
Will sickle cell disease be passed on to my child?
It is important that the father of the baby is tested to check whether they have the sickle cell gene. If both parents have the sickle cell gene, there is a risk that the baby can get SCD. If you have SCD but your partner does not have the different gene, then your baby will have the trait and be a carrier.
How does pregnancy affect sickle cell disease?
Pregnancy puts extra stress on the body and as a result SCD can get worse with an increase in the how often you have acute painful crises. Also, you can become more anaemic during pregnancy. This is due to an increase in plasma volume compared to the increase in red blood cells, causing the blood to become diluted and the amount of haemoglobin to decline.
How does sickle cell disease affect pregnancy?
Most women with SCD have a safe pregnancy with few serious complications owing to appropriate, coordinated care from the haematologist, obstetrician, nurses and midwife. It is important to plan ahead and discuss your plans for having a baby with your haematologist. This is so that your health status can be optimised before pregnancy, in order to increase your chances of having a healthy and successful pregnancy.
Sometimes sickle cell disease can cause serious complications in pregnancy, which can be divided into fetal, maternal and pregnancy-related complications.
Fetal complications
SCD affects the ability of red blood cells to carry oxygen that is particularly important in pregnancy.
- Intrauterine growth restriction – reduced growth of the fetus due to a reduced oxygen supply.
Maternal complications
- Pre-eclampsia (high blood pressure, and increased protein in the urine).
- Increased risk of uterine (womb) infection.
- Increased risk of blood clots in the leg and lung.
Pregnancy-related complications
- Miscarriage.
- Premature birth.
- Increased risk of requiring a caesarean section.
- Increased risk of bleeding during labour.
Pre-pregnancy care for SCD patients
Partner screening
- Genetic testing to find out the haemoglobin status of your partner.
- Counselling to discuss the chance of having an affected child.
- Specialist counselling if the father of the baby has SCD or is a carrier.
Up-to-date screening for chronic disease complications
Whether you are planning a pregnancy or not, you should see your SCD team at least once a year. Their checks may include:
- Echocardiogram (a detailed scan for your heart): looking for pulmonary hypertension (high blood pressure in the blood vessels that supply the lungs).
- Blood pressure: looking for raised blood pressure.
- Urinalysis: looking for protein in the urine.
- Blood tests: specially looking for iron overload or red blood cell auto antibodies.
- Retinal screening (a special eye test): looking for signs of proliferative retinopathy (problems at the back of the eye).
Medication review
You should discuss stopping certain medications with your haematologist, in particular:
- Hydroxycarbamide – Stop 3 months before conceiving.
- ACE inhibitors and angiotensin receptor blockers – medicines often used to control high blood pressure e.g. Ramipril.
- NSAIDs e.g. ibuprofen, diclofenac, naproxen.
Vitamin supplementation
High-dose Folic acid (5mg) every day – this will reduce the risk of worsening anaemia, as it helps the body to make red blood cells, and ensures a healthy pregnancy by reducing the risk of spina bifida in the baby.
Infection prevention
- Daily antibiotic prophylaxis (usually penicillin): as people with SCD are at high risk of infection
- Ensure vaccination are up to date including:
– Hepatitis B vaccine
– Flu vaccine
– H. Influenza type B vaccine
– Pneumococcus vaccine
– Neisseria meningitis ACWY and B
What should you do once you find out you are pregnant?
It is important to inform the Sickle Cell Disease Team as soon as you find out you are pregnant.
Regular midwife reviews and monthly attendance at a combined haematology and obstetrics clinic will be scheduled to monitor you and your baby’s health, and to plan further management of your pregnancy.
Antenatal care – what to expect
Medications
- Aspirin 150mg from 12 weeks – helps to reduce the risk of pre- eclampsia.
- Iron supplementation if iron deficient – usually not indicated in SCD patients as anaemia is caused by excessive breakdown of red blood cells rather than iron deficiency.
- Low molecular weight heparin (blood thinning injections) from 28 weeks of pregnancy unless indicated earlier – in order to reduce the risk of blood clots which is increased in SCD.
Monitoring
- Blood pressure – each consultation.
- Urine dipstick testing for protein – each consultation.
- Urine culture sample – tested for urine infections, which can sometimes be present without symptoms – monthly.
- Routine blood tests – monitor kidney and liver function and level of anaemia.
- Ultrasound scans:
– 7-9 weeks: Viability scan – to ensure a healthy pregnancy.
– 11-14 weeks: Routine first trimester dating scan.
– 20 weeks: Routine anatomy scan – screening for fetal anomalies.
– 24 weeks onwards: Monthly growth scans to ensure your baby is growing well.
Advice
Here are some tips to manage your SCD during pregnancy and avoid triggering crises:
Diet and fluids
- Drink plenty of fluids throughout the day, aim for 3-4 liters per day, to keep well hydrated and avoid dehydration that trigger a crisis.
- Early pregnancy is associated with nausea and vomiting
– vomiting can lead to dehydration therefore it is important to seek medical attention early if you are worried about persistent vomiting, or you are becoming dehydrated. - Eat a healthy, balanced diet.
Keep warm
- Extremes of temperature, especially being too cold, are known to trigger a crises. Therefore, it is important to keep warm by wearing warm clothing in winter, and ensuring your home, and working environments are well heated.
Monitor for complications
- Infection – seek medical attention early if you notice:
– Fever
– Burning pain on passing urine or urine that is more
smelly than usual (urine infection)
– Cough, bringing up yellow-green sputum, shortness of
breath or chest pain (chest infection) - Blood clots – seek medical advice if you are worried about swelling of one leg compared to the other, and pain in the leg.
Take adequate rest
- You should consider making adjustments to your working and home life to reduce your usual work load, and ensure you get plenty of time to rest – overexerting yourself during pregnancy may cause a crisis.
- You may begin to feel more tired than usual during pregnancy; this could be a sign that your anaemia is worsening. In severe cases of anaemia, a blood transfusion may be required to top up your red blood cells, or alternatively you may require iron supplements.
What should you do if you have an acute crisis?
- If you experience pain, you should begin by taking simple painkillers, such as paracetamol or weak opioids such as
- co-codamol (but NSAIDs such as Ibuprofen should be avoided), and oral fluids.
- If the pain cannot be controlled at home or if you have a fever, experience pain that is not your usual sickle pain, shortness of breath or chest pain, you must seek urgent medical advice and come to the hospital promptly.
- In hospital, you will be given strong painkillers, oxygen to breathe, and fluids through a drip in your arm if you are dehydrated. You will also be checked for other causes of your symptoms and you may be given antibiotics. You should also be given blood-thinning injections during your stay in hospital to reduce the risk of blood clots. You will be monitored closely – often in a high-dependency area of the hospital. Your baby’s wellbeing will be checked.
How will my labour and baby’s birth be managed?
You will be seen by the haematologist, obstetrician and midwife at 34-36 weeks to discuss your options for the timing and method of birth of your baby, pain relief during labour and care of your baby after birth. After taking your preferences into account, an individualised labour plan will be drawn up and agreed on by the team and yourself.
If your baby is growing normally it is usually recommended that you are admitted to hospital for induction of labour between 38 and 40 weeks. The baby will be continuously monitored throughout labour ensuring that any signs of fetal distress are detected and acted upon straightaway, to reduce the risk of complications.
What will happen after birth?
How soon you can go home will be determined by how well you are and how your baby was delivered. Normally, after a vaginal delivery, providing you are well and there are no complications, you may be discharged within one to two days. However, if you have had a caesarean section or experienced any complications you may need to stay in hospital longer.
You will need to receive blood-thinning injections after you have given birth to reduce the risk of blood clots. The length of treatment with these injections is for six weeks no matter the nature of your delivery.
Your baby will be routinely tested for sickle cell disease after birth and the results will be discussed with you.
What about contraception?
Progesterone-only pills, Progesterone injections (Depo- Provera), implants (Nexplanon), the coil containing hormones, and barrier methods (condoms and caps) are safe and effective.
The combined estrogen/progesterone oral contraceptive (‘the pill’) and copper coil can be used, but only if the above methods are unsuitable for you. You can talk to your GP or family planning specialist.
Useful contacts
Obstetric Secretaries
Monday to Friday 09:00 – 16:00.
Maternity Assessment Centre (SJUH)
Open 24 hours a day, 7 days a week.
Maternity Assessment Centre (LGI)
Open 24 hours a day, 7 days a week.
Haemoglobinopathy Team Clinical Nurse Specialist
Monday to Friday 09:00 – 16:00.
Haematology Wards
Monday to Friday 09:00 – 16:00.