What is a cerebral tumour embolisation?
The aim of a brain tumour embolisation is to improve surgical outcomes of tumour removal by reducing blood loss.
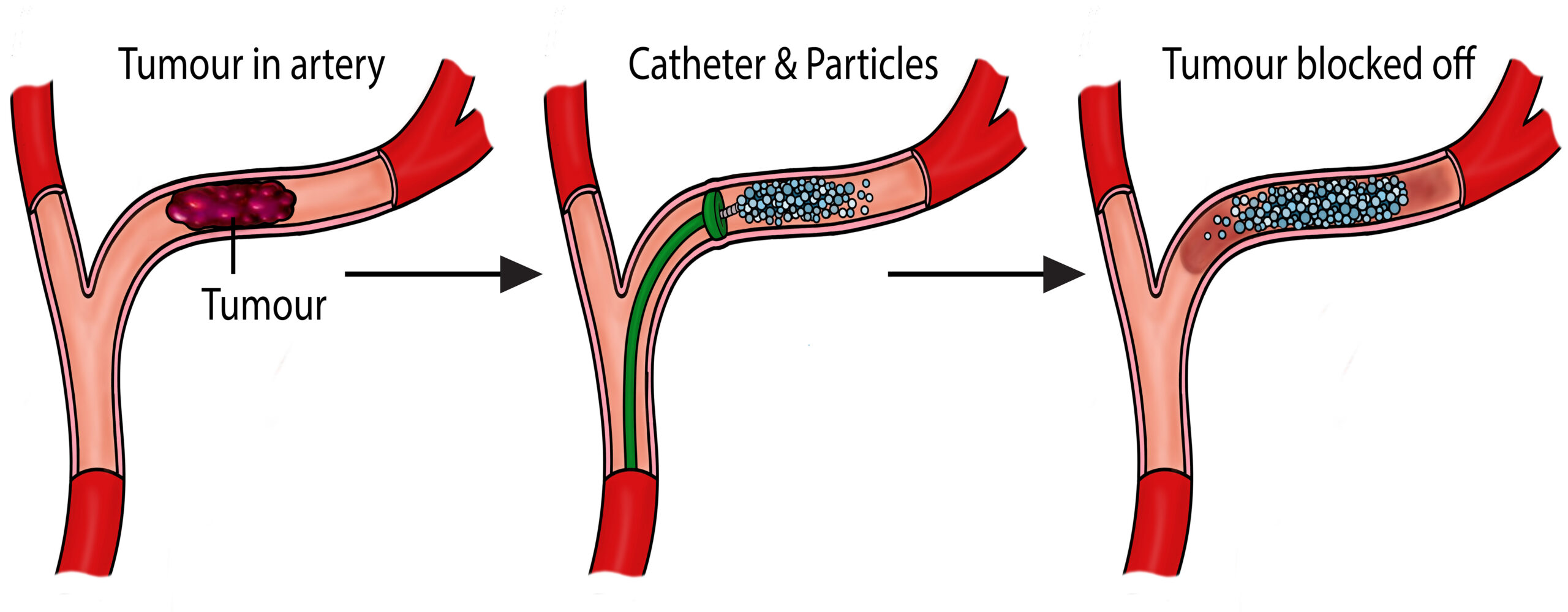
Embolisation is a term used in vascular operations whereby blood vessels are purposefully blocked to stop blood flow in arteries or veins. A brain tumour embolisation is primarily performed before tumour removal surgery, to block major blood vessels supplying the tumour.
How do I prepare?
This procedure is done under general anaesthetic, so you will need to fast for at least six hours. Before entering the theatre environment, you will be given a hospital gown and asked to remove any artefacts such as jewellery, glasses, dentures etc. as any metal may obscure your x-rays. A cannula will need to be in place to provide you any medication throughout the procedure, this will also be used to administer anaesthetic medicine.
You will then be taken to theatre, where a team of radiologists, anaesthetists, nurses and radiographers will be setting up for your procedure. You will be shown where to lay on the x-ray table and be made as comfortable as possible.
How is a Cerebral Tumour embolisation performed?
Consent
Before the procedure, the Neuro-radiologist will meet you in our recovery area to discuss the procedure in more detail, the risks and answer any of your questions to your satisfaction before you provide your permission and sign your consent form.
Anaesthetic
Brain tumour embolisation operations are done under a general anaesthetic. This means you will be put to sleep under the care of an anaesthetist. You will meet your anaesthetist before the operation where you may discuss any anaesthetic related queries.
Operation
When you are asleep, you will be positioned on your back with an X-ray machine above you. The radiologist will make a small hole in the femoral artery at your groin; this is the only opening needed for the operation.
Small tubes called catheters will be guided by X-ray through the arteries in your brain supplying the tumour. Special X-rays using contrast (X-ray dye) will be taken to demonstrate where exactly these blood vessels are supplying. When the target arteries are found, the radiologist will use an embolic agent to block the arteries from reaching the tumour.
This can take several hours depending on the complexity of the tumour anatomy. The small hole in your groin will be closed using a device to plug the hole that has been made. This will be monitored throughout your stay.
Staff involved
Interventional Radiology (IR) procedures are performed by a multidisciplinary team. The team includes the following key Staff:
- Interventional Radiologist (Consultant/Fellow): A doctor specially trained in minimally invasive, image-guided techniques who performs the procedure.
- Radiology Nurses: Highly trained nurses who care for the patient before, during, and after the procedure. They assist with sedation, monitor vital signs (heart rate, breathing, oxygen levels), and may “scrub in” to assist the radiologist directly.
- Radiographers: Experts in imaging equipment who operate the machines to provide real-time guidance for the doctor.
- Senior Clinical Support Workers (SCSWs): Assist with the setup of the room, patient positioning, and maintenance of sterile conditions
What are the risks?
This is overall a safe procedure, although with any procedures, this carries the following risks:
- Stroke – introducing foreign equipment into the brain such as catheters brings the risk of stroke as they can develop blood clots. There is also a risk of haemorrhagic stroke from the bleeding of the tumour or a blood vessel in the brain
- Groin haematoma – there is a small risk that the plug of the groin will not work effectively. This can result in a leak from the artery into the surrounding tissue. Manual compression is most effective at resolving this. In more serious cases a pseudoaneurysm, a bulging weakness in the artery, may form. This can be blocked off with an injection using ultrasound or in extreme cases, surgical intervention.
- Anaphylactic reactions to contrast are rare. Out of all contrast reactions, only 0.6% of them result in anaphylaxis. These extreme reactions usually happen within 20 minutes of the contrast being administered. Moderate reactions include: Severe vomiting, bronchospasm, facial oedema, vasovagal attacks. Mild reactions include: nausea, vomiting, rash, headache. Please let a healthcare professional know if you have had a previous reaction to X ray dye before your procedure.
- X-rays will be used to make images of your body and guide your doctor during the procedure. X-rays are a type of radiation. We are all exposed to low levels of natural radiation as part of our everyday lives and medical x-rays give an extra dose of radiation. Radiation can increase your chances of developing cancer many years or decades after the exposure. The chances of this happening to you as a result of this procedure are considered to be very low.
- In some very rare situations, you might experience some hair loss or some reddening of the skin in the area that was imaged. If this happens, you should contact your clinical team who will be able to give some advice on the simple steps you can take to look after your skin.
- It is important to remember that your doctor thinks that the benefits of this procedure outweigh any risks from the radiation. We will make sure that the amount of radiation used in your procedure is as low as possible.
What else to expect from this operation?
Admission
You will arrive at the admissions ward at LGI in the morning, where the nursing team will complete your admission. The anaesthetist will usually see you there. Once a ward bed becomes available, you will be transferred to the radiology theatres. The radiologist will then go through the consent process with you. After this, you will be taken into the theatre for your general anaesthetic and the procedure.
Recovery
You will wake up from your operation in a separate recovery area, where specialist recovery nurses will look after you. During this time, your groin puncture site will be monitored closely, and you will need to remain on bed rest. Once your initial recovery period is complete, you will be transferred to a ward, where you will stay until your tumour removal surgery.
Aftercare
After your procedure, you might be able to sit up slightly (around 45 degrees) if a small plug has been used to close the artery in your groin. If a plug isn’t used, you’ll need to stay lying flat for a while, depending on the size of the tube that was inserted. Nurses will regularly check your groin site and monitor your neurological observations. You’ll then go on to have your surgery, which usually results in less blood loss thanks to the embolisation done beforehand.
Care at home
There may be specific care at home instructions you need to follow after the tumour removal surgery. You may ask your neuro surgeon for more specific advice.
- Exercise: It is advisable that you rest for the first 24 – 48 hours after your procedure and avoid going up and down stairs too frequently and do not carry put any heavy lifting, you should not do any strenuous exercise during this time.
- Work: You might need to take a significant amount of time off work for appointments, treatment and recovery.
- Driving/travel: You might need to stop driving for at least one month. You may ask your neuro surgeon when it is safe to do so.
- Medicines: The radiologist will advise you when to restart any medication that was stopped for the procedure.
- Follow-up: You will usually be seen in a follow up appointment with your neurologist or the specialist neurovascular nurse and you might also require further follow up scans.
Contact information
We hope some of your questions have been answered by this leaflet. If there are any questions you would like to ask before you come for your operation, please get in touch.
Interventional Radiology LGI
Ward 24 LGI
Ward 25 LGI
Neuro Nurse Specialists
Your GP or NHS direct
How to get to our department
We are located in the Jubilee Wing of LGI, Ground Floor.