Introduction to fetal monitoring
At all times you will be given information that allows you to make an informed choice about all aspects of your care.
Your community midwife will have a conversation with you about monitoring your baby in labour as part of your antenatal care and document your discussions and decisions in your personalised care plan. This conversation will take into account your pregnancy, your well-being and your birth preferences.
Most babies come through labour without any problems, but there are a few babies who run into difficulties. The best way of finding out which babies are having trouble is to listen to every baby’s heartbeat regularly throughout labour.
There are no current guidelines to suggest when your midwife should listen to your baby’s heartbeat during pregnancy, however it is possible to hear it from approximately 16 weeks.
From 24 weeks, your midwife will ask you about your baby’s movements every time you see them and, if there are any concerns, they will ask to assess you and your baby.
This may result in a visit to the Maternity unit at the hospital.
How do we listen?
If you are healthy and have had a problem free pregnancy, your midwife will ask to listen to your baby’s heartbeat using a Pinard stethoscope or a hand-held doppler.


During labour your midwife will ask what method of monitoring has already been advised and decided upon as part of your personal antenatal care plan.
Intermittent Auscultation
When you are in labour, the midwife will ask to listen to your baby’s heartbeat at least every 15 minutes, immediately following a contraction, and more frequently as labour advances. This method of monitoring is called intermittent auscultation. The advantage of this method is that it enables you to move around freely and can be used in water.
It is important that the midwife starts listening to your baby’s heart beat just as your contraction is going away, and they will need to count the heartbeat for a full minute.
It is helpful if you know about this as your midwife may ask you to change position to make this easier.
The midwife will need to count your baby’s heart beat for a full 60 seconds every time they listen in.
If your midwife notices a change in the baby’s heart rate that suggests your baby might not be coping well, they will tell you and they may recommend continuous monitoring.
The midwife will ask to manually feel your pulse on your wrist every hour during the first stage of labour and if you are still having intermittent auscultation during the second stage, they will ask to feel your pulse every five minutes. This helps your midwife be sure that it is definitely your baby’s heartbeat that is being picked up and not yours.
Continuous electronic fetal monitoring (CTG)
This type of monitoring produces a continuous ‘trace’ of the baby’s heart rate throughout your labour and is referred to as a cardiotocograph or CTG
The CTG monitor has two sensors that are strapped around your abdomen, one to monitor the frequency of your contractions and the other to monitor your baby’s heart rate.
Continuous monitoring can limit your ability to move around, however it is still possible to mobilise, or to change your position to standing or sitting on a birthing ball.
A wireless monitor may be available. This allows you to move more freely.
Risk assessment is an ongoing process and the recommended method of fetal monitoring may change throughout labour. If there are no identified risk factors for fetal compromise, there is a risk of increased interventions with continuous CTG monitoring compared with intermittent auscultation, which may outweigh the benefits. Advice given by the midwife or obstetrician on the method of fetal heart rate monitoring will take into account the whole clinical picture.
When performing CTG monitoring your midwife may find it difficult to get a clear trace on the graph (particularly when you are pushing or mobilising). If this happens, they may ask permission to monitor your baby with a fetal scalp electrode (FSE). If this method of monitoring is recommended during your labour your midwife or doctor at the time will discuss this with you and support you to make an informed choice.

What is a fetal scalp electrode (FSE)
An FSE is a small wire that is placed just beneath the baby’s scalp by piercing the skin. This may give a more accurate and continuous reading compared to abdominal monitoring during labour (please see image below).
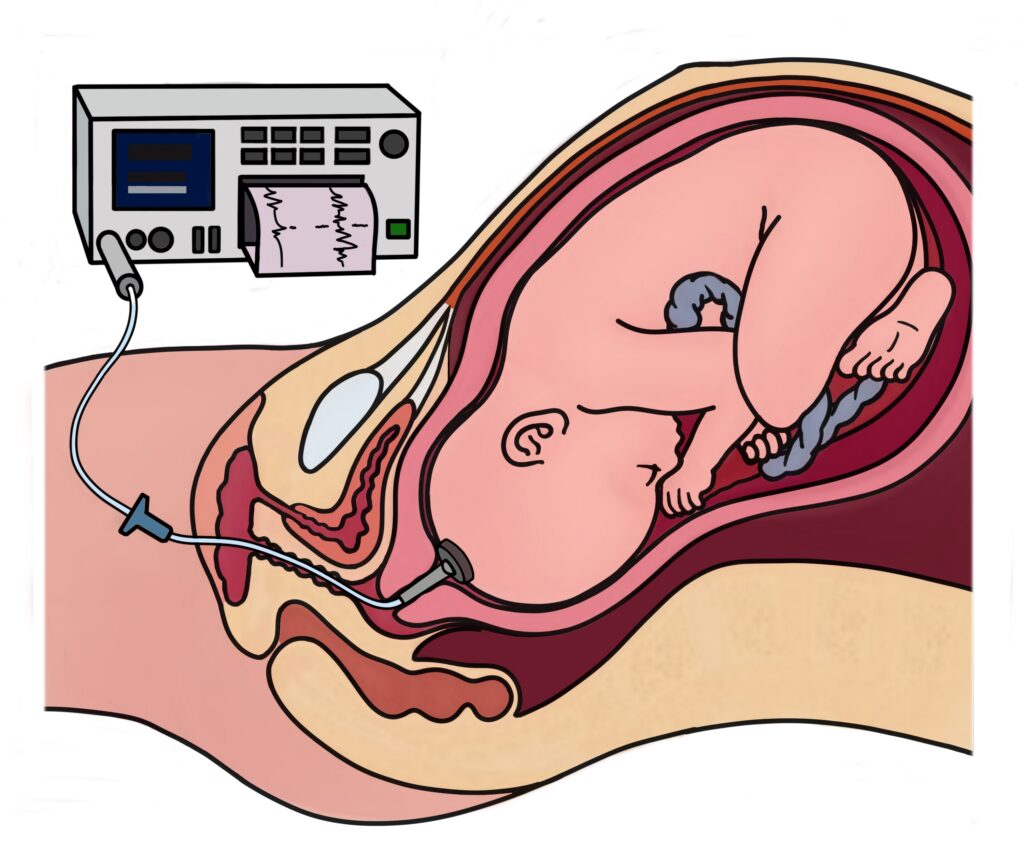
Your midwife or doctor will insert the electrode through your cervix during a vaginal examination. They will carefully attach the electrode to your baby’s head. The electrode is then connected to the CTG machine, which tracks your baby’s heartbeat.
The procedure is generally safe and very commonly used. However, it does carry some small risks, such as:
- Slight bruising to the baby’s scalp.
- Irritation to the baby’s scalp.
- Rare risk of infection to the baby’s scalp.
Things to remember
- A normal CTG trace indicates that the baby is coping well with labour.
- Changes to your baby’s heart rate pattern during labour are common and are not always worrying.
- Sometimes these changes can show which babies are having trouble coping with the stress of labour.
- If your midwife has concerns with the CTG they will ask your permission to invite a senior midwife and/or doctor to be involved in your care and they will make an assessment to find out if there is an identifiable cause that can be corrected.
- Such causes include an infection developing which can be treated with antibiotics or if there are other signs that your baby may be distressed such as the baby opens their bowels inside (passes meconium).
- This will be all be considered along with how your labour is progressing to make a personalised plan of care for you and your baby taking into account your preferences.
Peer review (Fresh Eyes)
Every hour during your labour, another midwife or doctor will ask to come into your birthing room to review your care and the CTG; this is called a peer review (fresh eyes) and is normal practise to ensure consistent, accurate interpretation. If you are having intermittent auscultation the timing of the reviews may vary.
The following will be considered at each review:
- What your contractions are like.
- Any antenatal and intrapartum risk factors that you may have.
- How you are feeling.
- How well your labour is progressing.
- Interpretation of your baby’s heart beat tracing.
This hourly risk assessment is a continual process and so it is good to bear in mind that your recommended method of monitoring may change during your labour.
The results of this hourly assessment will be discussed with you and recommendations on your care in labour will be based both on these findings and your preferences.
Helping you feel safe and comfortable
While you are in labour your midwife will help you to be as mobile as possible, to find positions that are comfortable and to change position when you want to.
A midwife will stay with you while you are in active labour.
This is called 1:1 care and is a national recommendation. If the midwife needs to leave the room, they will tell you why and how long they will be. You will be given a call buzzer so you can call for help.
If another midwife comes to care for you while your midwife takes a break, you will be told that this is happening and the new midwife will be introduced to you and informed about your care and preferences.
If you prefer not to have a midwife in your room all the time, then please tell them and agree between you how the midwife can continue to safely monitor you and your baby.
What are we checking for?
The normal range for the rate of the baby’s heartbeat is between 110 and 160 beats a minute, although this can be higher or lower without meaning that the baby is in difficulty. The variation in the baby’s heart rate may be caused by the womb contracting, which affects the blood flow to the placenta (afterbirth). This is normal and most babies cope without any difficulty.
If your baby is not coping well, this may be reflected in the pattern of their heartbeat.
How will we monitor your baby?
In an uncomplicated pregnancy and labour intermittent auscultation will be offered.
Continuous electronic fetal monitoring will be offered if:
- The midwife has concerns with your baby’s heart rate.
- You have a raised temperature.
- Your baby has had their bowels opened (meconium stained liquor).
- You have any bleeding during labour.
- You have an epidural for pain relief.
- Your labour progresses slowly, and you require a hormone drip.
- Or if there are other factors that may affect your labour and baby’s wellbeing.
If you have experienced problems during your pregnancy, or if you have certain medical conditions which may affect your baby, we will offer you continuous electronic monitoring from the start of your labour.
Reasons for this may include:
- Your baby is small or premature.
- Your pregnancy has lasted more than 42 weeks.
- You have high blood pressure.
- You have diabetes.
- Your baby is not coming head first.
- You are expecting more than one baby.
- You have had a caesarean section in the past.
- Your waters have broken over 24 hours ago.
- You are being induced.
- You have had bleeding during your pregnancy.
- Your baby has not been moving normally during the past 24 hours.
What happens if we suspect a problem?
If your midwife identifies changes in your baby’s heart rate which may indicate a worry, they may ask you if they can try measures to correct it. For example, they may ask you to change position to alleviate pressure on the baby’s cord.
If the changes persist, your midwife will ask the labour ward coordinator or a doctor to review the baby’s heart rate. This means that the doctor and/or co-ordinator may need to come into your room. You may be asked if you agree to having a vaginal examination to assess your baby’s wellbeing, in addition to the progress of your labour.
Following this, a discussion will take place with you and your birthing partner to make a decision about whether it is appropriate to continue with the labour, or whether an assisted birth, or caesarean section is recommended. You will be given all the information you need, in terms you can understand, so that you can make an informed choice.
If you need any further information about the methods we use to monitor your baby, or the reasons why, please talk to your midwife or doctor.
The use of hand-held Doppler and mobile phone apps
If you have your own Doppler to listen to your baby’s heartbeat or are planning on purchasing one, this is not recommended by health professionals. Although the use of a Doppler is safe, what can be problematic is how the sounds you hear are interpreted by you.
Often you can pick up the blood flowing through the placenta or your own heartbeat and think that you are hearing your baby’s heartbeat.
Only health professionals trained in their use should be using a Doppler to listen to your baby’s heartbeat.
Be even more careful with the use of mobile phone apps that also claim to monitor your baby’s heartbeat. These apps do not have adequate regulation and it is difficult to know what kind of testing they have been through to check they really work.
If you feel that your baby is not moving as much or the pattern of movements has changed, please speak immediately to the Maternity unit at your hospital, who will invite you to come in so that you and your baby can be monitored.
Important
Please don’t delay or think that you are being a burden. We are here to make sure you and your baby are safe – 24 hours a day, every day of the year.
Useful resources
Contact us
Leeds Teaching Hospitals NHS Trust
Maternity Assessment Centre – Leeds General Infirmary
Maternity Assessment Centre – St James’s University Hospital
This patient information leaflet has been co-produced by the fetal wellbeing lead midwives, obstetricians and service user representatives from the six trusts that make up West Yorkshire & Harrogate Local Maternity and Neonatal System:
- Airedale NHS Foundation Trust
- Bradford Teaching Hospitals NHS Foundation Trust
- Calderdale and Huddersfield NHS Foundation Trust
- Harrogate and District NHS Foundation Trust
- Leeds Teaching Hospitals NHS Trust
- Mid Yorkshire Teaching NHS Trust