This leaflet aims to give you some information about hip replacement surgery.
The hip joint is a “ball and socket” joint. The hip allows movement to occur between the thigh bone (femur) and the hip bone (pelvis). The pelvis contains the socket called the acetabulum.
The Hip Joint

About the hip replacement
The aim of the replacement surgery is to:
- Relieve your pain
- Improve your quality of life
The hip prostheses are designed to copy the human anatomy as closely as possible. There are many different designs of hip prosthesis available and your surgeon will choose the one considered most suitable for you.
Components of a hip replacement
Each hip prosthesis is made of several parts.
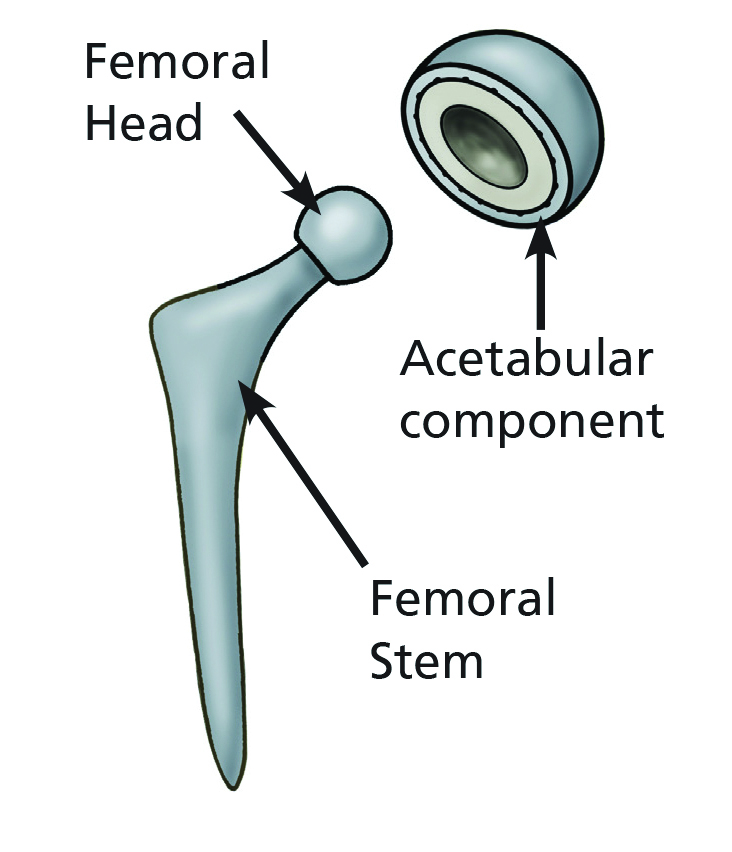
- The acetabular component replaces the acetabulum. The part that articulates with the femoral head can be made of ceramic or plastic.
- The femoral component replaces the femoral head. It consists of the femoral stem, made of metal l and the femoral head which is either ceramic or metal.
- Each component can be fixed to the bone using cement or without. Both have excellent long-term results. You can ask your surgeon which is most suitable for you.
- We no longer use metal-on-metal hip replacements as there have been concerns about early failure.
Primary total hip replacement
Risks of Surgery
Total hip replacement is one of the most successful operations for relieving pain and disability.
Approximately 95% of patients have no problems following surgery but up to 5% of patients develop a problem.
These include:
- Chest infection.
- Wound problems such as infection or a blood clot.
- Deep joint infection. This is rare (less than 1% risk) but almost always requires further surgery to clean the hip joint or exchange the implants. You will also need antibiotics for around 6 weeks.
- A dislocation of the joint after the operation. This is where the femoral head comes out of the acetabular component. Usually this is treated by putting it back in under an anaesthetic without opening up the wound. However, if it happens more than once you may need to have further surgery.
- Leg length inequality. Every care is taken to ensure the leg lengths are equal at the end of the operation. However, sometimes this is not possible and the patient may be left with a minor degree of leg length difference.
- Loosening. Your hip replacement may wear out in time and if this causes problems the implants may need to be exchanged.
- Fracture. Sometimes this can occur during the surgery but if you were to fall and fracture the acetabulum or femur with the hip replacement in place, this may require further surgery to fix the fracture and maybe exchange the implants.
- Nerve damage.
- A blood clot in the leg (deep vein thrombosis).
- A blood clot in the lungs (pulmonary embolus).
- Urinary retention. You may need a temporary catheter to help you pass urine.
These problems are usually treated in a straightforward way and may only cause a short delay in your recovery. They usually do not affect the long‑term result of the operation. Hip replacement is major surgery and like all major surgery carries a risk. Approximately 1% of patients have a major problem which may not be correctable.
This may lead to a situation for you that is worse than before the primary surgery. This may be permanent. It is therefore important that you carefully weigh up the risks and benefits before going ahead. It is extremely rare for a patient to die following hip replacement (about 1 in 2000) and these patients usually have major long-term health problems.
An artificial hip will not allow heavy work, lifting, running or repetitive impacts. Heavy gardening and impact sports will be limited. You may kneel following hip replacement but you will not be able to rest back fully on your heels.
You may need further surgery to redo your hip replacement some years after your original operation if it wears out or if there is another problem with it such as infection, dislocation or fracture.
Advice before your hip replacement surgery
Points to remember
- The operation usually takes 1 ‑ 2 hours.
- The most important thing you can do is to get motivated to ‘get up, get going and get home’ after your surgery.
- Your recovery begins now. Don’t forget to start your exercises as soon as you are listed for surgery. It will help with your recovery after surgery.
- The occupational therapist will be in contact with you for advice and education about the surgery and rehabilitation.
- You will be out of bed and taking some steps immediately after surgery with the help of a Zimmer frame or elbow crutches.
- You will continue to practice your exercises throughout your stay. These will be monitored by your physiotherapist.
- If stairs are applicable to your home setting you will be assessed on these before you go home to make sure you are safe.
- You will be in hospital until you are safe to go home. This is variable between patients and some will even go home on the evening of surgery.
Hip exercises before surgery
To get the most out of your hip replacement, it is important that you start your exercises before your operation.
It is your responsibility to carry out the exercises independently and regularly. A diagram of each exercise is provided in the booklet given to you by your physiotherapist.
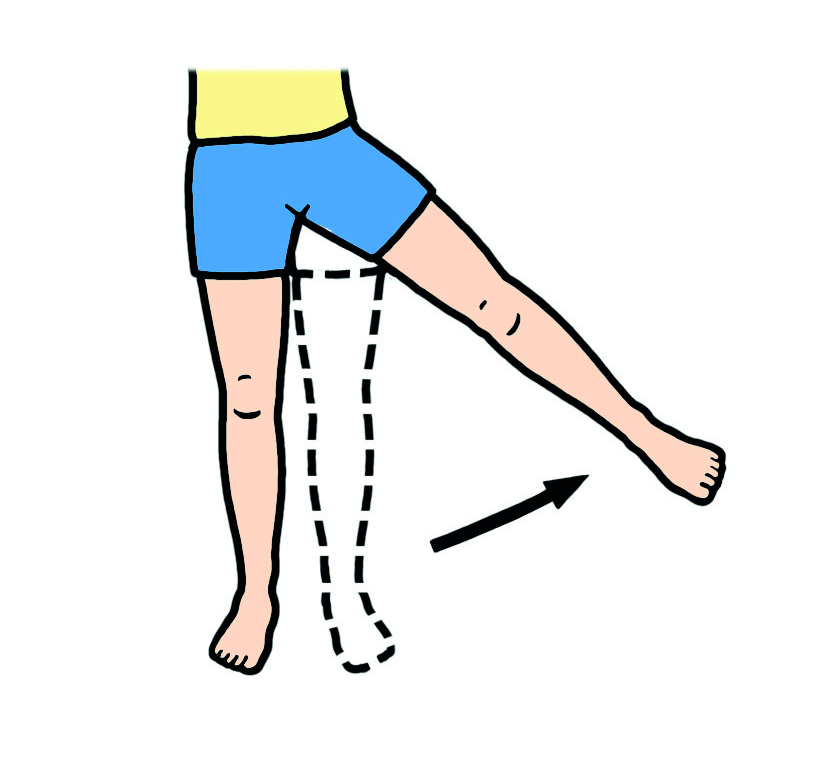
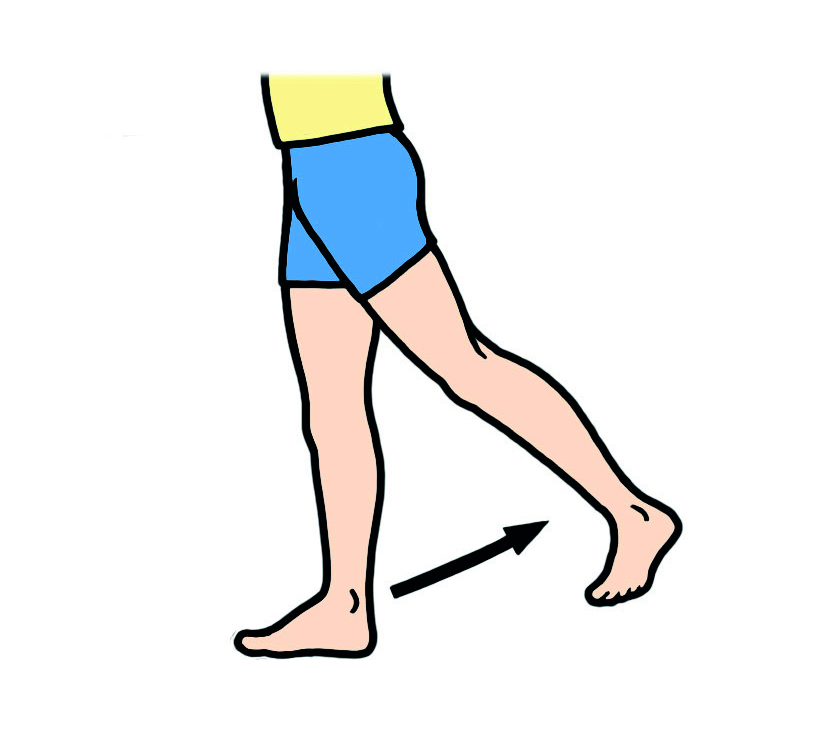
Try and do these exercises three times per day
For each exercise make sure you are holding onto a secure object e.g. worktop/ table.
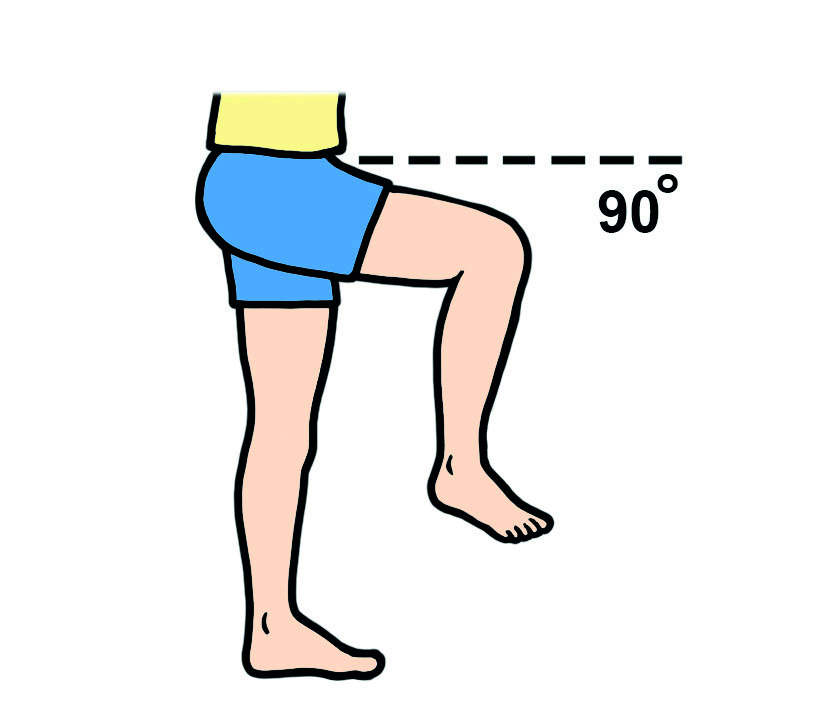
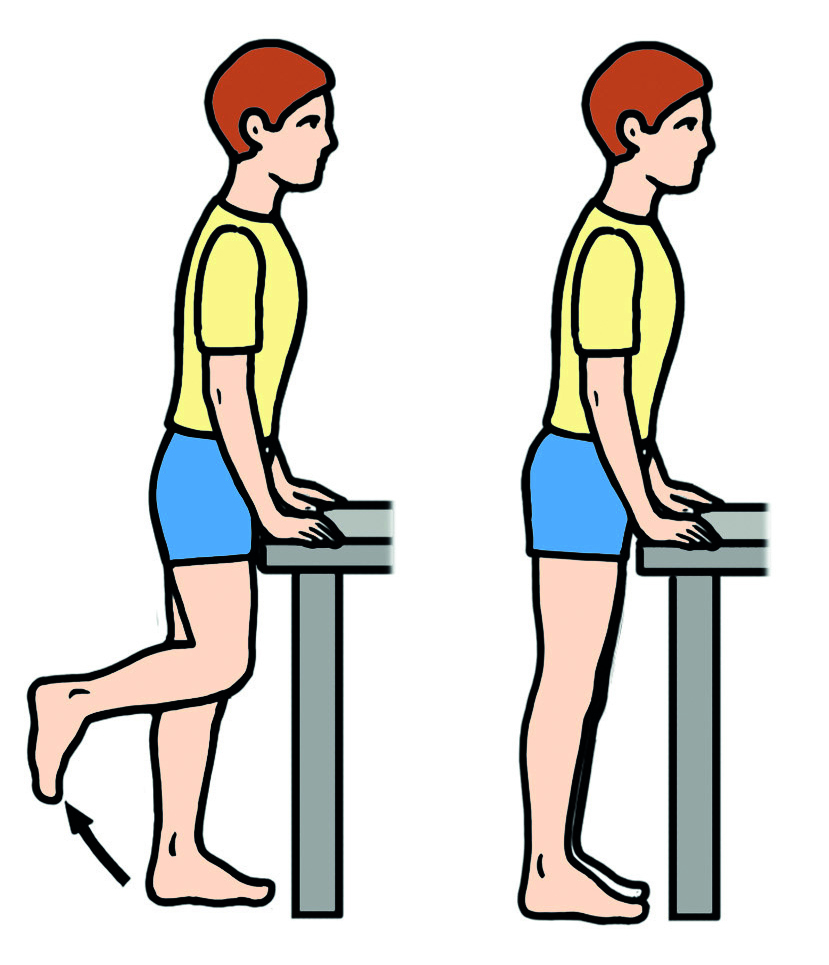
Gently bend your operated knee bringing your foot towards your bottom. Hold for a few seconds and slowly lower.
Advice after hip replacement surgery
Hip precautions
You may be required to follow specific hip precautions following your operation. You will be advised about this prior to surgery by the therapy team.
Returning to work
You may return to ‘light’ duties as soon as you feel able to do so and continue on ‘light’ duties for the first three months after your hip operation.
Driving
You may begin driving again six weeks after surgery providing you can do an emergency stop.
Sport
It is advisable that you avoid any sport which involves excessive movement of your hip (e.g. Yoga) or jogging or jarring of your hip joint (e.g. running, squash). Avoid swimming for three months. Please also refer to the booklet provided to you by your occupational therapist that includes a full list of sports and when they may be resumed.
Sex
Sexual relations may resume cautiously from six weeks to three months. The person with the hip replacement should lie on their back whilst their partner is on top. There are no limits after six months, however care should be taken to avoid excessive bending of the hip.
Useful contact numbers
Pre-assessment
Hip School
Theatre Scheduler
Ward C3 post-op
It is normal to have a degree of swelling and bruising to your leg following surgery.
If you have any concerns after discharge home, with anything, particularly your wound, pain or swelling please feel free to contact Ward C3 for advice, and assessment if indicated.
Your x-rays may be used for teaching/research purposes. If you do not want this to happen, please let your surgeon know.