This leaflet explains how to prepare for your knee replacement surgery.
The knee joint
The knee joint is one of the most complex joints in the body. Apart from bending and
straightening it also rotates and glides. It is made up of three bones, the thigh bone (femur), the shin bone (tibia) and the knee cap (patella). The joint is covered by articular cartilage which ensures that movements of the knee are pain free and smooth.

The knee joint is enclosed in a joint capsule which is lined with fluid.
The knee movements are started and controlled by the strong muscles of the thigh and lower leg.
When a knee develops arthritis it is the articular cartilage which becomes worn and roughened. This is painful.
About the Knee Replacement
The aim of the replacement surgery is to:
- Relieve your pain
- Improve your quality of life
Knee replacement surgery involves resurfacing the ends of the femur, the tibia and if necessary the underside of the patella with man made components, called prostheses.
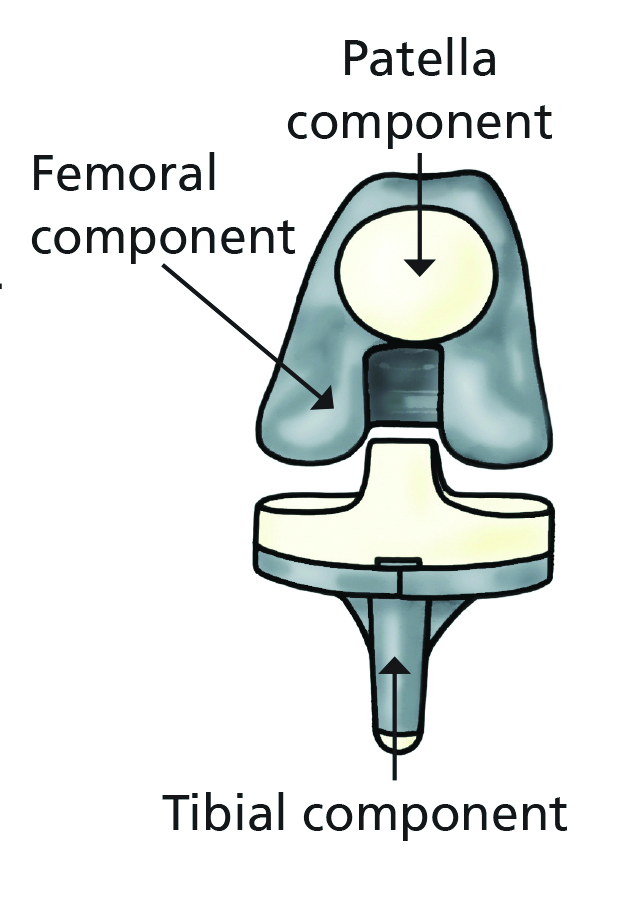
Components of a Knee Replacement
Each knee prosthesis is made of several parts
- The femoral component resurfaces the femur. It is made of metal.
- The patella is not always resurfaced. The patella component is either made completely of plastic or plastic with a metal back.
- The tibial component can be a one or two piece design. The single piece is made of plastic. The two piece is metal and plastic.
Primary total knee Replacement
Risk of Surgery
Total knee replacement is one of the most successful operations for relieving pain and disability. About 90%, that is 90 out of 100 patients, have no problems following surgery. 10%, that is 10 out of every 100, develop a problem. 5% have a complication.
These include:
- Chest infection
- Wound infection
- Urinary infection
- A blood clot in the leg (deep vein thrombosis)
- A blood clot in the lungs (pulmonary embolus)
- Nerve damage
- An area of numbness adjacent to the scar.
These problems are usually treated in a straightforward way and may only cause a short delay in recovery. They usually do not affect the long term result of the operation.
- 5% of patients have no complication but their knee remains painful or stiff and they are not happy with the outcome of surgery.
Amputation is fortunately very rare. Loss of a limb is usually a result of a deep infection, or may occur more commonly in people suffering from circulatory problems and insulin dependent diabetes. It is extremely rare for a patient to die following knee replacement (about 1 in 2000) and these patients are usually not very fit before the operation.
Most patients can bend the knee to a right angle after a knee replacement. Some patients feel that their new knee joint is stiff and the leg swollen. This is quite normal and usually settles on its own by three months after the operation.
An artificial knee will NOT allow heavy work, lifting or repetitive impacts. It will not allow running, and heavy gardening will be limited. If individual sports are important to you discuss these with your consultant before surgery.
You may not be able to squat down or kneel following your surgery. You may need further major surgery to revise your total knee replacement some years after your original operation.
Advice before knee surgery
Points to remember
- on’t forget to start your exercises now. It will help make your recovery easier. You will be expected to know the exercises well for your recovery.
- Please see our ‘Shape Up 4 Surgery’, section with advice and videos for you to watch before surgery. Scan the QR code or visit the website:
Shape Up 4 Surgery
- After your surgery, the physiotherapists will aim to get you out of bed and take a few steps with the help of a zimmer frame, this can be on the same day as your surgery.
- You will recommence your exercises the day after surgery and will be expected to be completing these on a regular basis. Some of your exercises can start on the same day that you have surgery but you will be advised by the physiotherapists if this is the case. Your exercises will be monitored by a physiotherapist.
- Once you are able, you will be progressed from a zimmer frame to elbow crutches. If it is applicable to your home, you will be taught how to climb stairs with your crutches to make sure you are able to manage them before being discharged home.
- If stairs are applicable to your home setting you will be assessed on these before you go home to make sure that you’re safe.
- You will be in hospital until you are safe to go home. This is variable between patients and some will even go home on the evening of surgery.
- The operation usually takes 1 – 2 hours depending on the severity of the disease in your knee.
- Before you go home you should be able to get in and out of bed, shower, dress and go up and down the stairs.
Knee exercises
Try and do these exercises three or four times per day.
1) Sit with the leg straight out on the bed. Pull your foot up and tighten the front of your thigh. Press the back of the knee down into the bed, hold for five seconds then relax. Repeat 10 times until the muscle feels tired.
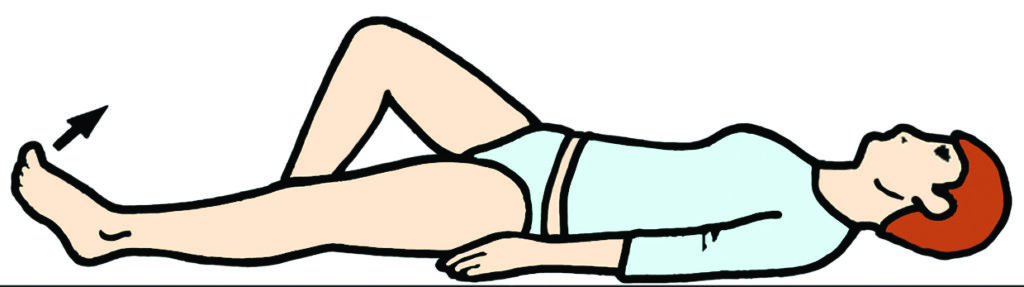
2) Sit and brace your knee as in the first exercise. Keeping your leg straight raise the leg a few centimetres into the air. Keep your toes pointing upwards. Lower slowly. Repeat until the muscle feels tired.
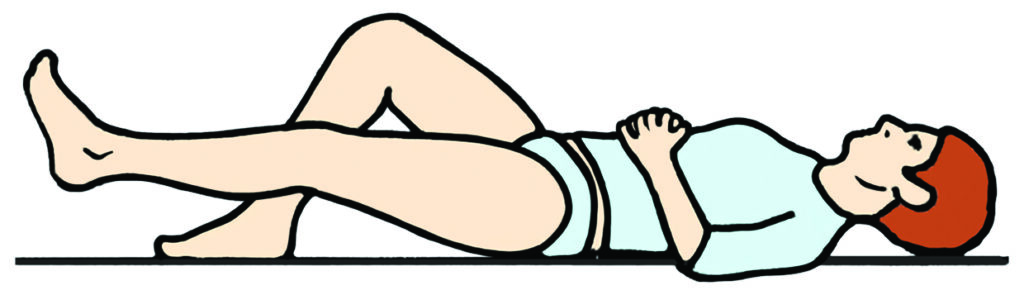
3) Rest your leg on a sliding board/shiny tray. Bend your knee upwards as far as you are able. Hold for five seconds then slowly lower. Each time, gradually aim to bend a little further. Repeat 10 times. You may also bend your knee when sitting in a chair or on the edge of a bed. Repeat 10 times.

4) Place a rolled towel or blanket under the knee during this exercise. You must remove it immediately when you have finished. Lift the heel off the bed, straighten the knee and hold for five seconds. Lower slowly. Repeat until the muscle feels tired.

Useful contact numbers
If you have any concerns regarding surgery, please ring for advice:
Pre-Assessment
Theatre Scheduler
Ward C3 post-op
Ward C3
It is normal to have a degree of swelling and bruising to your leg following surgery.
If you have any concerns after discharge home, with anything, particularly your wound, pain or swelling please feel free to contact ward C3 for advice, and assessment if indicated.
Please note
Your x-rays may be used for teaching/research purposes. If you do not want this to happen, please let your surgeon know.