This leaflet is aimed at patients who have undertaken an anterior cruciate ligament reconstruction and will inform them on both the surgical and rehabilitation process at Leeds Teaching Hospitals NHS Trust.
The ACL, injury and reconstruction
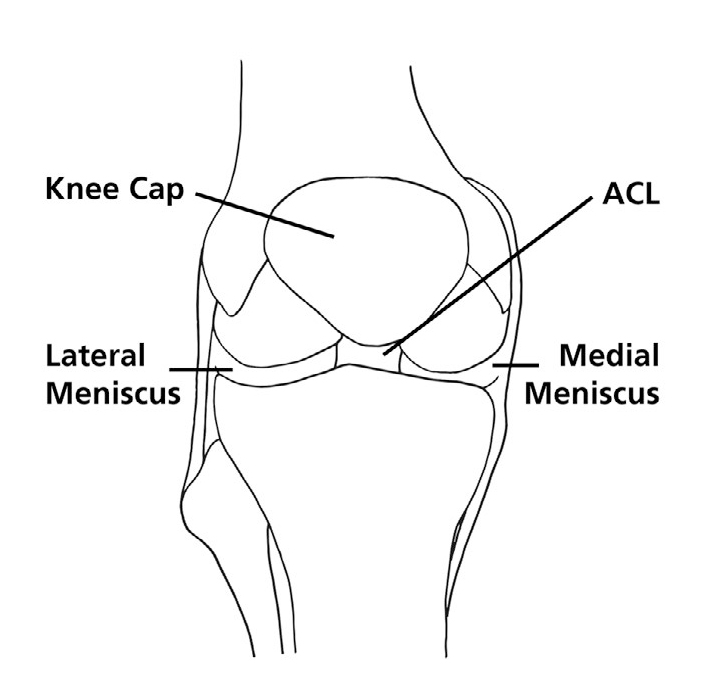
The anterior cruciate ligament (ACL) is a ligament in the knee that provides it with stability. Injury can result in the knee giving way and sometimes meniscus or cartilage damage. The aim of surgery is to restore the functional stability of the knee whilst retaining range of movement.
If an ACL is completely torn, in most cases the ends of the torn ligament will not heal back together, even if the torn ends were repaired or stitched together. A reconstruction involves removing the torn ends and replacing it with a graft which is tissue that is harvested through a small (less than 5cm) incision usually from the hamstring tendons (which come from the muscles in the back of the thigh and attach to the front of the shinbone).
There are other graft alternatives which your surgeon will discuss with you if necessary.
With the help of an arthroscope (camera) placed through ‘keyhole’ incisions on the front of the knee, tunnels are made in the shin bone (tibia) and thigh bone (femur). The graft is passed through and secured in these tunnels with special buttons and/or screws to form your new ACL. If meniscal or cartilage surgery is required this can usually be performed at the same time.

Advice prior to surgery
Your operation will be performed by a specialist knee surgeon, usually as a day case procedure at Chapel Allerton hospital.
Whilst waiting for your operation your physiotherapist will organise an assessment at
St James’s Hospital to discuss your treatment options, set specific goals, advise on pain/swelling management and prescribe important exercises. Research has shown that the stronger and more functional the knee prior to surgery the better the outcomes after surgery.
On the day of your operation
You will have the opportunity to ask questions. You will be reviewed by a physiotherapist and your anaesthetist will explain the anaesthesia process. Your surgeon will discuss the indications, benefits and risks of surgery. The knee undergoing surgery will be marked and you will be asked to sign a consent form. The operation can take up to 1½ hours.
Risks of surgery
These include infection, stiffness, swelling, scarring, scar tenderness, pain, graft re-rupture, nerve injury and sensory loss (particularly around the graft harvest site scar), loss of muscle strength (especially quadriceps or hamstring if this tendon is harvested) and bruising at the back of the knee or thigh. The risk of deep venous thrombosis is very low and prevention is not routinely indicated.
After your operation
The wound will be covered by a simple dressing and a bandage will be wrapped around the knee. An x-ray will be performed for your surgeon to review. You will be discharged after physiotherapy review and when your pain is under control.
It is normal to have some pain, swelling and bruising to your thigh, knee and leg following surgery. Good pain relief is important to ensure adequate range of movement and prevent stiffness. You will be able to move your knee and weight bear as your pain allows but crutches are generally required for up to three weeks.
If meniscal surgery is also performed, you may need to use a range of movement knee brace. You may be instructed to use elbow crutches and your physiotherapist or surgeon will tell you how much weight to put through the operated leg.
An outpatient appointment will be made for you to return to see the doctor and a sick note will be provided, if required to cover the period from your operation until your return to clinic.
Rehabilitation
ACL reconstruction requires a lot of dedication from the patient towards rehabilitation. You will need to commit to doing your exercises as prescribed by your physiotherapist and attend physiotherapy appointments when organised. This process can take up to 1 year to complete successfully and may be delayed further if complications arise or rehabilitation is not followed.
Early stage post surgery
In this stage you will see a physiotherapist on a one to one basis at St James’s University Hospital. Your physiotherapist will advise on pain, swelling and range of movement exercises.
You are advised to walk with crutches for the first few weeks as you regain a normal walking pattern. There will be set criteria you will need to meet to be able to progress to the mid stage of the rehabilitation process.
Mid stage post surgery
Once the early stage criteria have been met you will have opportunity to attend the mid stage ACL class working with both a physiotherapist and a strength and conditioning coach at St James’s University Hospital.
Here you will aim to build strength, mobility, stability and will be introduced to more dynamic tasks, such as running. Some exercises will be restricted to ensure protection of the ACL graft therefore it is important to follow the instructions and goals set by your physiotherapist.
Advanced return to sport stage post surgery
Once mid stage criteria have been met you will have opportunity to attend the advanced stage ACL class, which will take place at St James’s University Hospital and be led by a physiotherapist and a strength and conditioning practitioner.
Here, more vigorous strengthening exercises will be undertaken, with a gradual introduction to power activities (hopping, jumping, sprinting, cutting and pivoting drills). Further evidence based criteria will need to be met to be able to successfully return to sport/activity.
ACL Videos – YouTube
Anterior Cruciate Ligament Injury; an overview. Transcript.
my name is sanjeev
i’m a knee surgeon at leeds teaching
hospital and i deal with knee injuries
in children and young adults today we’re
talking about acl which is anterior
cruciate ligament it is one of the main
ligament inside the knee
and it keeps the knee together
especially in twisting movement
it’s a common injury unfortunately and
usually people get this injury while
doing sports which involve mostly
pivoting or twisting
it can occasionally happen when you
contact contact injury with someone or
it can often happen when you twist
without any contact with somebody else
people who have this injury often it’s a
significant force which goes through the
joint and there feels like a pop in the
knee and the knee swells up soon after
that
and often people limb for a few days two
weeks after that it is important that
this injury gets identified and picked
up so that the appropriate and timely
management can be taken if you injured
your knee and you find your knee is
swollen significantly and you’re
struggling to work you should seek
medical attention either a gp or your a
a service can direct you to the
appropriate pathway and most hospitals
have acute knee service where these
injuries can be assessed and
appropriately managed
your clinician would assess your knee
for not just for this ligament injury
but also for the injuries to the
structures around the knee where the
different ligaments because
understanding injuries to those
influences management of this
cruciate ligament injury as well it’s a
good clinical assessment we’ll be able
to identify whether you’re done in
injury to this ligament your doctor or a
clinician may ask for further imaging
which may be either x-rays or mri scan
they want to know whether you’ve done
damage to other structures besides aca
because they can influence the
management of this injury your clinician
will discuss different treatment options
with you it could either be surgery or a
trial of physiotherapy your treatment
will depend on what your demands from
your knee is and also damage to the
other structures around the knee some
people can manage without hcl especially
if your sport does involve mostly
running in straight line say you may be
given an option of trying physiotherapy
and see if you can manage with your knee
but if there are other injuries to the
knee sometimes your surgeon may advise
you surgery directly surgery is best
done once you recover your full movement
with a knee joint and that’s
what we call prehabilitation and you may
be referred to a physiotherapist service
to get your knee moving and to recover
strength because surgery itself can
reduce strength and if you have a good
strength before your surgery you get a
better outcome afterwards of course
there are certain indications when
surgery may be needed urgently and your
surgeon would be able to advise you on
that your surgeon will discuss different
ways they want to do surgery mostly
it will work putting a new acl using
different graft and it is a choice of
graft which can be used which could be
often is either hamstring or your
kneecap tendon and your surgeon will
discuss this can benefit of each with
you hi i’m nyle and i’m one of the lower
lymph physiotherapists i’m going to talk
to you today about what you might expect
once you’ve had an acl injury suspected
so once you have injured your knee
and the assessments have been made you
may be waiting for some imaging you will
then be referred to physiotherapy to
help with improving the movement in your
knee it’s very important to manage the
swelling you may need to do this by
elevating your knee using ice if it’s
allowed and then some very early gentle
exercises as your knee improves and the
movement increases you’ll then be able
to do some early strengthening exercises
which will continue to improve your
function and your outcome in certain
cases there may be some restrictions on
what you may be allowed to do if there
is associated suspected injuries for
example with meniscus tears you may be
advised to avoid deep squatting and
bending while carrying a weight the
period in between when you are in what
we would call your rehabilitation phase
after injury and before surgery
is very important to help you get the
best outcomes for any possible surgery
that you need to undertake however as
mentioned by the colleagues there is
definitely a successful conservative
path that people can take and they don’t
require surgery and will get excellent
outcomes as long as they do the correct
exercise and manage things well to
improve your outcomes
with your knee injury be that
conservative or surgical management it’s
key to work on equalizing the strength
in your legs and trying to improve the
injured side compared to the uninjured
site and this will be one of the tasks
that the physiotherapy team and strength
conditioning team will help you to
achieve
one of the key exercises to work on
after you’ve had an acl injury and also
when you’ve had your acl surgery from
day one post up is to try and achieve
extension in your knee or straightening
of your knee so the way to do this is to
comfortably put a towel under the back
of the knee not too high and then you’re
aiming to apply tension into the
quadriceps muscle
as we’ll demonstrate
excellent you may or may not get a heel
lift off of the bed depending on your
normal levels of movement
patient hair has excellent quadriceps
activation however sometimes it may be
difficult to achieve with swelling and
with the nerve block so a cue to use
sometimes is if you place your hand
underneath and you sit on your hand
try not to squash your hand try and
tighten the muscle and gentle pressure
into the towel again you achieve that
quadriceps activation
what you’re aiming to do if you relax
again is for your kneecap or your
patella to pull gently upwards into this
fashion when you’re tightening the
muscle
this would be carried out as soon as
it’s comfortable and you would be doing
this three to four times per day and you
can do this in time or you can do this
for repetitions and this will be
explained to you on the ward
the next really important exercise to
work on is bending your knee or flexing
your knee and you can use a towel to
help do this either on a sliding surface
or even with a plastic bag under your
foot if needed and then pull towards
trying to work towards the amount of
range movement that you’re allowed to if
you have an associated meniscal injury
you may be restricted to 90 degrees at
this point but your brace will dictate
this however for an isolated acl injury
you try and achieve as much comfortable
bend as possible
and on the way out you can combine the
movement by trying to straighten the
knee also by tightening the quadriceps
and finally you can pull the toes
towards you to stretch your calf muscle
at the bottom of the leg here this is
combined type exercise you can also
break it up into its various parts by
just focusing on the bend if you need to
in situations where it’s difficult to
achieve full straightening or full
extension you may need to place your leg
onto a table a chair or a block which
will allow you to put some space between
your knee and the bed and gravity will
help you to assist in straightening the
knee it may be uncomfortable to leave it
longer than 10 to 15 minutes and you may
need to change position as comfort
allows however you can then combine this
position by trying to tighten your
quadriceps as we’ve demonstrated
and this would be an excellent exercise
for patients that are struggling to get
into extension or straight knee position
as an extra addition to the passive hang
position you can also apply a gentle
calf stretch in this position to feel it
stretch at the back of your calf or
lower leg in this area holding for up to
15 to 20 seconds releasing the tension
and repeating as comfort allows
the amount of times you do any of these
exercises will be guided for you by the
physiotherapists on the ward or your
physiotherapist when you attend the
outpatients department
another important exercise when you’ve
had an acl reconstruction in the early
stages is to gently activate your
hamstring the way to achieve this would
be with the knee bent in this position
gently pressing your heel into the bed
until you feel the tension build up in
this area here
you would do this until you feel fatigue
may take up to 10 to 15 repetitions and
you’ll be guided at the amount that you
do this each contraction should take up
to 10 seconds to achieve
another important exercise to work on
for static quadriceps activation you can
resist with your unoperated leg in this
case this side and the tension is
applied by pushing this leg forward but
meeting the tension in the middle and
holding that contraction in your
quadriceps this is good for activating a
quadriceps and is safe to do in the
post-op phase according to the
literature time would be to hold the
activation for up to 10 seconds as
comfort allows and again for inducing
that fatigue you may then develop
towards 10 to 15 repetitions as you’re
able to improve this exercise the range
of movement will be then increased by
your physiotherapist once you attend
your patient’s appointment
another excellent exercise to help work
on extension is a simple inner range
quadriceps exercise in standing by
placing a ball or a rolled up pillow or
rolled up towel at the back of the knee
tightening the quadriceps muscle at the
front of the leg and gently squeezing
back into the ball to achieve that
straightening of the knee holding the
tension in the muscle for up to 10
seconds
it can be repeated up to 10 to 15 times
a key teaching point here would be not
to rotate the hip backwards and to also
try and push the middle of the foot into
the floor to achieve that muscle
activation
the next important exercise to consider
is an exercise for your calf region to
help stabilize the lower part of the leg
after surgery or after injury a simple
calf raise where you go up onto your
tiptoes on both sides trying to maintain
that the knee is straight on both sides
and slowly lowering body
weight the key teaching points here are
not to allow your hips to swing forwards
and to try and keep equal weight on both
legs as you work through the exercise
next exercise to cover would be a knee
lock on lock exercise or a mini squat
where the aim is to allow your knee to
soften so take the tension out of the
straightened position and now you need
to bend to approximately 30 degrees on
both sides and then to slowly bring it
back to a straight position locking it
into place by tightening the muscles
what you want to avoid here as you bend
your knees down is too quickly snapping
the knee back which you’ll get an
example of now
so you want to try and control that
speed and tension by increasing the
tension in the muscle of the front of
the knee and also pressing your foot
into the floor will help to control this
the progression for this exercise and
you may achieve this before your first
physiotherapy appointment would be to
try this exercise on your operated leg
again allowed attention to ease off on
the straight knee you don’t have to bend
too far forwards and then bring your
knee back to a straight position under
control keeping that tension
another good example
and slowly bring it back to the starting
position this is again an exercise which
can be done until the knee starts to
feel fatigued aiming for up to 10 to 15
repetitions it also will help on
standing balance as is important for
achieving good proprioception or good
balance and position awareness from the
knee after the injury all these
exercises will be shown to you on the
ward and also will be reinforced when
your first physiotherapy appointment and
then they will either be progressed or
you will maintain at that level until
you improve your function
Strength and Conditioning for ACL injuries. Transcript
hi i’m harry i’m the strength
conditioning coach at Leeds Teaching
hospitals
patients can be referred to me anytime
after the 12-week mark so coming to snc
you’d go from doing more generic and
general strengthening etc
to more specific and individualized
programs and exercise based work which
will be tailored to what your end goal
is
so
that’s where the timeline may vary
patient to patient and the
exercise type might also vary in how we
periodize that training
for the individual what we’d look to do
initially is to strength test you so we
look to get as symmetrical in strength
as possible with your operated and
non-operated limb that way you’ll be in
the best place possible going forward so
what we’d need to do is strength test
and achieve above 80
symmetry that way we can then progress
to doing some low-level plyometrics so
that’s involves hopping
maybe a little bit of change of
directional hop in as well just getting
your knee used to taking a little bit
more impact so we go to sort of break in
first and then proportion side of it
afterwards then what we do after that is
do a plyometric test
where it’s a series of hops
in which we want to achieve again above
80 of symmetry between the operating and
non-operating limbs so after the
plyometric tests we then look to
go towards return to play strategies or
return to goal if you’re not actually
returning to sport but instead returning
to
activities that you’d be used to doing
before your injury what we’d do is give
you some high-level plyometrics to do
build the intensity slightly in the hops
etc give you a guided program in which
to go away and do yourself in terms of
timeline from going from
operation
to discharge or return to play this
could be anywhere between nine and 12
months post acl reconstruction ideally
patients would want to be getting back
to sports as early as possible we
understand that but there’s also
research to suggest that if you return
to sport within sort of the nine
month
timeline then you’re at seven times more
risk of re-injury which is really what
we want to avoid so
given the extra time and the extra focus
on this sort of return to play
controlled environment which we provide
it will guide you better and
reduce the risk of re-injury going back
to sport
How to use a Range of Movement Brace for Meniscal Repair. Transcript
If your surgeon requires you to have a
brace
on your knee after your surgery we will
fit this for you in recovery when you
come out of theatre you’ll have a big
bulky dressing on your knee
this generally comes down 48 hours after
your operation and you may find you need
to adjust
the tightness
of your brace
always ensure
the dials are in line with your knee
joint
you should not need to touch anything on
these dials they will be set for you
your brace needs to be worn
all of the time
even when sleeping
to protect the healing of the structures
that you’ve had surgery on
we recommend that you have a strip rush
rather than removing it to go into the
shower
undoing the brace to have a strip wash
you simply need to press
on the clasp to release
when your bandages come off or
your swelling changes you will need to
adjust how tight or loose your straps
are
to do this you will pull up on the
velcro
and pull it tighter you’ll pull across
or to loosen
relax it off and pull back through
your brace needs to be tight enough so
that it does not slip down when you walk
but loose enough to not leave
indentation marks in your skin
as a general rule you say you need to be
able to snugly fit a finger underneath
you need to ensure you wear the brace
directly in contact with the skin
and not over the top of clothes if you
wear it over the top of the clothes it
will slide down
so we recommend wearing shorts
or baggy trousers
most of the time your movement will be
allowed between naught to 90.
so this gray dial should be
in line with naught
and on the flexion it should line up to
90.
if you have not maybe knocked your brace
and you need to reposition it you need
to press the dial in
slide along
in line to the number you need to get at
it is locked in position when it pops
back up you need to make sure
that the red button is pointed towards
the unlock picture
this will allow your brace to move if
you find
your brace is not allowing you to move
it might be that it’s slid down to the
locked position
slide your finger up
to unlock
How to do stairs with crutches. Transcript
hi my name’s kimberly i’m one of the
physiotherapists that work on the
electrical orthopedic unit at chapel
alton hospital we’ll see you on the
morning of your operation to measure you
up for crutches and teach you how to use
these in a variety of different
weight-bear statuses depending on the
repair that you have within your knee we
will also go through your basic
exercises that well you will need to do
in the first few weeks following your
surgery give you education
on the use of ice to help with your
swelling management it is normal after
your surgery to have swelling within
your knee
we recommend that once your nerve block
has worn off and you can feel touch to
your knee use ice up to five times a day
to help reduce the swelling when you’re
using ice this could be a bag of frozen
peas wrapped in a damp cloth only put it
on your knee for a maximum of 20 minutes
and always check that there’s no adverse
reaction to your skin
it is important after your operation
that you use the crutches as we advise
and you do not come off these until
you’re advised in your outpatient
appointment the exercises are important
to keep your knee moving especially
getting your knee straight after surgery
and switching on your quadricep muscles
to provide stability around your knee
joint it’s normal to experience
post-separative pain it’s important you
take your pain medication as prescribed
and we recommend timing doing your
exercises with pain relief
approximately 30 minutes after taking
your pain relief
after your theatre you’ll be brought
round to recovery where the nurses will
monitor your heart rate and your blood
pressure as you come around from your
own aesthetic once you have come around
you’re feeling well and have had
something to eat and drink we will come
and see you again from physiotherapy at
this point
we will have read through your operation
note and we’ll inform you of your weight
bear status and whether or not you need
to wear a brace
if you need this brace we will apply
this for you we will assess your leg to
see if you have your sensation back
whether your muscles are switching on if
you do not have your sensation back
but are keen to go home that same day
you need to make sure you are
non-weight-bearing which we will have
practiced before you go into theatre
we’ll make sure you’ve retained the
information that we’ve given you in the
morning and we’ll check through your
exercises we’ll help get you up out of
bed and having a walk you will be able
to go home
that day depending on the effects of
your anesthetic and whether your pain is
well controlled it might be that the
surgeons require you to wear a brace
after your surgery we’ll go through how
to adjust this once you have come out of
theatre and we fit the brace for you if
it is required the brace will need to be
worn at all times and the length of this
will depend on the structures that you
have repaired we recommend that you do
not touch the dials on the brace
but you will need to alter it once your
dressings have come down
and as swelling changes
[Music]
if you’re able to take weight through
your leg if you have a handrail on your
stairs at home you’ll pass the crutch on
the side of the handrail to the opposite
hand
it wants to go in a t-shape and be on
the outside of your other crutch so if
it falls it doesn’t trip you up
to go up the stairs
you’ll go up with your unoperated leg
then your
operated leg
and then your crotch
[Music]
to come back down the stairs again you
will pass the crotch on the side of your
rail to the opposite arm
make sure you’ve got a good grip
go down with your crutch and keep your
hand in line with your crotch on the
rail step down with your operated leg
and then you’re unoperated
to go up the stairs if you do not have a
handrail you will step up with your
unoperated leg
push down through your crutches step up
with your operated
bring both crutches up to join
[Music]
to come back down the stairs you’re
going to step up to the edge of the step
place both crutches down making sure
they’re towards the back of the step
step down with your operated leg and
bring your unoperated leg to join
[Music]
if you’re a non-weight bearing and you
have a rail you pass your opposite
crotch across opposite hand
hold on to your banister
bend your operated knee so your toes are
off the floor you’re going to pull up on
the rail and push down on the crotch to
hop yourself up the step
bring your crotch up to join you on that
same step
[Music]
come back down again you’ll pass the
crutch across to your opposite hand
move the crotch down onto the step in
front of you
straighten your leg out in front so your
toes don’t catch
and then you’re lowering yourself down
on your unoperated leg onto the step
below
[Music]
if you are non-weight bearing to go up
the stairs you’ll put your operated leg
bent
get yourself nice and close to the edge
of the step
you’re going to push down through both
crutches
to hop yourself up onto the step
try make sure you do not catch your toes
on the operated leg
to come down the stairs i recommend you
stick your operated leg out in front of
you to help maintain your balance
bring your crutches down in front
and lower yourself down on your
unoperated leg
[Music]
[Applause]
[Music]
before your operation when we see you
from physiotherapy we will measure you
for elbow crutches
to do this we will ask you to stand
up relax your arms at your side
[Music]
you want to make sure the handle of your
crutch is in line with the bony point on
your wrist
we’ll then teach you how to stand up and
sit down with the crutches
if you are full or partial weight
bearing
the crutches will create a h shape in
front of you
one hand goes onto the handle one hand
on the chair arm
and push up to stand
your free arm will go through the hand
of the crotch hold on to both handles to
allow your other hand in
bring the crutches out to the side
handles pointing forwards and your
elbows in towards your body to sit down
it is the reverse bring the crutches in
front of you
one hand feels onto the crutches and
hate shape one hand onto the chair and
sit down
if you are non-weight-bearing
post-surgery due to your nerve block
when you stand up and sit down you need
to make sure your operated leg is kept
up off the floor
have a stand up
the legs off the floor one hand in
then the other
and crutches out to the side
maintaining your balance
to sit down it is the reverse keeping
your operated leg off the floor
and a controlled sit down to your chair
[Applause]
[Music]
[Applause]
after your acl surgery you’ll be walking
on crutches to help offload your knee
it’s important that you try and get your
knee straight when you’re walking and
walking without a limp when you walk
you’re going to put your crutches and
place them in front of you
step with your operated leg into the
line of the crutches and then bring your
unoperated leg through
if your surgeon has requested that you
are non-weight bearing or your foot is
still numb after your surgery
you will need to learn to use the
crutches in a different technique for
this bend your knee keep your toes off
the floor
place the crotches in front of you and
then hop into the line of the crutches
with your other leg
you’ll need to brace your arms and keep
your elbows into your body
Return to driving, work and activity
Rehabilitation rates vary from person to person and depending on whether meniscal surgery was performed. As a general guide, depending on your range of motion and ability to perform an emergency stop, you should refrain from driving for around four weeks. You need to inform your car insurer about your surgery.
Return to office work should be possible after approximately 2-3 weeks. If you have a job that involves heavy physical work you should leave 8-12 weeks before going back to work.
Swimming (but not breast stroke) can usually be started by 3-4 weeks and riding a stationary bicycle by 6 weeks.
It is recommended that adults (over 18 years of age) should not return to sports until at least 9 months post op and an evidence based return to sport criteria is met. Those under 18 years of age, should not return to sport for at least 12 months.
If you have any concerns following surgery
Please feel free to contact Ward C3 for advice and assessment if indicated. Alternatively, contact your GP or your local Emergency Department.