Brugada syndrome is an inherited heart condition that causes an unusual pattern on the heart trace (ECG).
What is Brugada syndrome?
Brugada syndrome doesn’t cause any problems in most people. However, it can lead to symptoms, such as palpitations or faints. Palpitations in general are the sensation of a sudden fast heartbeat because of a change in the heart rhythm. Palpitations and faints can be common in people who don’t have Brugada syndrome so they may be unrelated. But in Brugada syndrome, it may represent a fast heartbeat, and therefore, it is important to let your cardiology team know if you faint.
How common is it?
In this country, it affects around 1 in 5000 people, but in other parts of the world, it is much more common, particularly in parts of Southeast Asia. Although it is a genetic condition and is passed on to men and women equally, men tend to be more affected than women.
What does the typical Brugada ECG look like?
To recognize the characteristic changes of Brugada syndrome, you need to know a bit about how the heart works, how it beats, and what we look at on the ECG.
The heart has four chambers – two top chambers called atria, and two bottom chambers called ventricles. Blood returns to the heart from the body into the right atrium. The blood passes through a valve into the right ventricle and is then pumped to the lungs. Once the blood has picked up oxygen from the lungs, it returns to the left atrium, passes through a valve into the left ventricle, and is pumped back around the body.
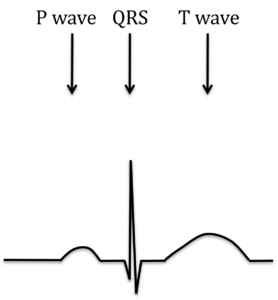
For the heart to pump blood around the body, an electrical impulse is needed to stimulate the heart muscle. This electrical impulse happens automatically and starts in the top right-hand corner of the heart. It spreads smoothly over both atria, and this causes a blip on the ECG called a P wave. The impulse is then channeled through a special signal box in the heart’s center and down the specialized electrical cables that trigger the ventricles to contract and pump blood. This causes a sharp spike on the ECG called the QRS complex. The heart now relaxes in preparation for the next heartbeat. This is seen as a broad hump on the ECG called the T wave.
Back to topFigure 1: The normal heart trace (ECG)
In Brugada syndrome, part of the QRS complex, labelled the J point is elevated, the ST segment slopes downwards, and the T wave is upside down. This makes the ECG looks very different (Figure 2).
Figure 2: Normal ECG (A) and Brugada ECG pattern (B)

The ECG appearance is very variable and can change from day to day. Sometimes it is very obvious, and sometimes it is barely detectable at all. The most obvious Brugada ECG pattern is called a Type 1 pattern, and when we see this, the diagnosis is straightforward. At other times, though, less obvious patterns called Type 2 and Type 3 may be seen. These do not prove the diagnosis but make us suspect it.
Back to topHow is Brugada syndrome diagnosed?
Sometimes, an individual may have symptoms such as palpitations or fainting, and tests have shown signs that they have the condition. In other people, the diagnosis is made purely by chance. For example, if they are having a heart trace (ECG) for another reason.
What causes Brugada syndrome?
- Brugada syndrome is a genetic condition that can be passed down from one generation to the next. In a small number of people (about 20%), an alteration in the genetic code can be detected. Our genetic code (or DNA) is like a list of instructions for building our body and how it can function. If there is an alteration in the genetic code, it can change how the gene functions. The most commonly altered gene in Brugada Syndrome is the sodium channel gene (SCN5A).
- The sodium channel allows sodium (salt) to flow into each heart cell, which is the signal for the heartbeat to spread across the heart and so causes the heart to pump blood around the body. If this sodium channel isn’t working properly because of a gene alteration, it can affect how the electricity moves through the heart, leading to changes in heart rhythm (extra beats or faster heart rhythms). These changes in heart rhythms can then lead to some of the symptoms associated with Brugada syndrome (such as palpitations and faints) and can occasionally be dangerous.
- Our genetic code is very long, providing the instructions for building about 20,000 proteins, including the sodium channel. Genetic alterations occur in everyone, and most of them cause no problems. Occasionally, however, an alteration occurs which changes how a gene functions. This can cause inherited conditions such as Brugada syndrome.
- We inherit a copy of all of our genes from each parent. An alteration can be passed down from one generation to the next. There is a 50% (1 in 2) chance that a Brugada syndrome alteration will be passed on to a child. If you have another child, again, there is a 50% chance of passing on the alteration.
If a person has been diagnosed with Brugada syndrome, in most cases, one of the parents will also have the alteration, and there is a 50% chance that any brothers or sisters will also have the alteration. Having the alteration alone does not give a diagnosis of Brugada syndrome. Most people with the alteration never have any signs of the condition and lead perfectly normal lives. This is because we have a number of other genes that interact to give your unique presentation. If someone has the gene alteration, they can still pass it onto children even if they don’t have a clinical diagnosis of Brugada syndrome
What tests might I need?
There are several tests we can do in patients with Brugada syndrome.
- ECG: An ECG (or heart trace) is a quick test that uses 10 wires or electrodes to record your heartbeat for a few seconds. You will usually have an ECG with the wires in the normal position, as well as some with the wires placed a little higher on your chest. This makes it easier to see the pattern associated with Brugada syndrome that we look for.
- Echo (echocardiogram): An echo (or heart scan) is a totally harmless ultrasound of the heart. We don’t expect to see any changes in Brugada syndrome, but it is a good way of checking that there isn’t anything else going on with the heart that can mimic Brugada syndrome.
- Holter monitor: A Holter monitor is a heart monitor that you take away with you and records your heart rhythm over a period of time (usually about 24 hours). It is useful if you are having palpitations.
- Ajmaline test: Ajmaline is a short-acting drug that blocks the defective sodium channels in Brugada syndrome. If you already have Brugada syndrome, then this test is not necessary, but if your ECG is not diagnostic or unclear, then we can give you this drug through a drip in the arm over 10 minutes and monitor the heart trace. If you have Brugada syndrome, the typical ECG pattern usually becomes apparent within a few minutes. The drug wears off quickly, and the heart trace returns to normal. This is particularly useful if testing family members. It is very safe, and we do this on the day-ward.
Is there any treatment?
For most people, Brugada is managed by simple lifestyle modifications. However, people who are thought to have had a collapse or cardiac arrest caused by Brugada Syndrome are offered devices such as an implantable cardioverter defibrillator (ICD).
Lifestyle modifications:
- Avoid taking any of the drugs that can increase the chance of a Brugada pattern on ECG. These are found on the Brugada drugs list which can be found on the website www.brugadadrugs.org You should mention this list to any Healthcare Professional prescribing new medication for you. You should also check the ingredients of over-the-counter medicines, such a cough and cold remedies and antihistamines.
- Avoid amphetamines or amphetamine based drugs.
- Avoid binge drinking alcohol.
- Treat any illness associated with raised temperatures or fever with medication that can lower your temperature. These are Paracetamol (maximum of 4 doses a day) or Ibuprofen (maximum of 3 doses a day). Rarely, if your temperature remains very high after taking paracetamol, a short period of monitoring in hospital may be recommended.
- Minimise the risk of raising the body temperature by avoiding prolonged endurance exercise events such as marathons, triathlons, ironman, prolonged periods in saunas, steam rooms or bathing in hot tubs or hot water for long periods.
- Avoid sleeping less than 2 hours after a large meal. This may be particularly important if you are participating in Ramadan.
- If you have an episode of sickness and diarrhoea, you should keep well hydrate and use electrolyte replacement sachets (such as Dioralyte) to replace essential salts.
If you do have fast heart rhythms or faints, then these can sometimes be potentially dangerous. Part of your assessment in the clinic will be to assess your risk of these dangerous heart rhythms, and if we feel you are at risk, then we will discuss the option of an ICD with you. More information can be found about these devices here: https://www.bhf.org.uk/informationsupport/treatments/implantable-cardioverter-defibrillator
Rarely, people are offered medication or other treatment as part of their management. This will be discussed with you if needed.
Other than endurance events, you can exercise as normal with Brugada Syndrome.
Can I drive with Brugada Syndrome?
You are required to inform the DVLA if you have a diagnosis of Brugada Syndrome. You will still be able to drive, and it shouldn’t affect your insurance.
You can find the DVLA form here: https://www.gov.uk/brugada-driving
If you have any faints, you should stop driving until these have been investigated.
Back to topDo my relatives need to be tested?
Brugada syndrome is usually inherited; therefore, other family members may also have it. We recommend simple tests to check them out so we can advise them. Each first-degree relative (children, siblings, and parents) has a 50% (1 in 2) chance of carrying the alteration but a much lower chance of having the disease. Testing might help to clarify a person’s chance of having a dangerous heart rhythm.
We would see your relatives in the clinic, ask about symptoms, and perform an ECG, echo scan, and arrange an Ajmaline test, which will be done at a later date. If these tests are all normal, we can reassure your relative, and they would not require any further follow-up. If the tests showed Brugada syndrome, we would continue to see them periodically in the clinic and give any specific advice or treatment recommendations.
Not everyone with Brugada syndrome has a known genetic cause. This is why clinical tests (ECG, echo scan and Ajmaline test) are helpful to assess your family. In a small number of families, a gene alteration may be identified and so genetic testing alongside clinical tests may be offered.
How can I get further information?
Point of contact for clinical questions:
Adults:
Annabel Nixon & Rachel Walker, ICC Nurse Specialists,
Children:
Beth Lunn, Paediatric ICC Nurse Specialist
Charities:
The British Heart Foundation, SADS UK and CRY have information about Long QT syndrome and provide help and support for patients and families