Your doctor has recommended that you have a Colonic Dilatation. This leaflet will explain the procedure and what to expect on the day of your test. If you have further questions, please ask the nurses or doctors on the ward or discuss them with a member of the endoscopy staff on the day of your procedure
What is a Colonic Dilatation?
A colonic dilatation is a procedure where a narrowing (stricture) within the colon (large bowel) or at the end of the small intestine is stretched open. A specially designed balloon is used to stretch open the part of the bowel that is narrowed or blocked due to disease at the site of a previous surgical join (anastomosis). It is difficult to predict how long the procedure will take but it can take up to 1 hour.
Why am I having a Colonic Dilatation?
Before your dilatation other tests such as a colonoscopy, CT scan or x-ray have shown that your bowel has become narrowed. Your doctor will have discussed with you the likely cause of the narrowing within your bowel. There are different treatments available for people with a narrowed bowel but a colonic dilatation has been proposed as the best treatment option for you. You should make sure that you have had the opportunity to discuss your treatment options with your doctor and if you feel uncomfortable about having this procedure carried out, then you can decide against it. Your decision will be fully respected and you doctor will be happy to discuss alternative options.
What are the benefits and alternatives to having a Colonic Dilatation?
A colonic dilatation is usually a simple, straightforward and comfortable means of stretching a narrowed area in the colon. The only alternative would potentially be an operation.
What are the risks of having a Colonic Dilatation?
Having a colonic dilatation involves a small risk of haemorrhage or perforation (tearing) of the bowel. If this does occur, it may require an operation. The risk of this happening is difficult to predict. Studies have reported that the risk of a perforation may be up to 5%. In Leeds, we carry out a significant number of these procedures.
Bleeding is usually mild unless you take medication to stop clots from forming. Examples of such medication would include Warfarin, Sinthrone (Acenocoumarol), Dabigatran, Apixaban, Rivaroxaban, Edoxaban or Phenindione. Other medication which may cause bleeding includes Aspirin taken together with a second aspirin-like tablet such as Plavix (Clopidogrel) Dipyridamole (Persantin) or Asasantin.
A sore abdomen after the test is very common and should resolve after a few hours. A reaction to the sedative drugs used is another complication and although very rare, if it did occur, you would be required to stay in hospital. A reaction may vary from a simple skin rash, to difficulty in breathing.
Back to topWill I be asleep for my Colonic Dilatation?
The procedure is usually carried out under sedation by using a combination of a sedative (such as Midazolam) to relax and a painkiller (such as Pethidine or Fentanyl). Sedation is not a general anaesthetic and will not put you to sleep; however, it may make you feel relaxed and possibly, a little drowsy. We can only give sedation if you have a responsible adult to accompany you, take you home (not via public transport) and look after you for the next 24 hours. If you are unable to arrange this you, should contact the Endoscopy Unit for advice.
Another option that you may want to consider is Entonox (gas and air). Entonox is commonly used by women during childbirth and can help with any discomfort during your colonic dilatation. The gas is administered by a special mouthpiece which you will hold during the procedure. The Entonox gas works within 30 seconds and you may feel light headed and sleepy. You control the amount of gas that you have yourself by simply removing the mouthpiece but the nurse looking after you will monitor you closely throughout the procedure and make sure that you are using the gas successfully.
One of the benefits of Entonox is that when the procedure is over, the gas is quickly eliminated from the body so you can usually leave the department soon after your procedure as long as you feel well enough. Unlike sedation, you can drive 30 minutes after the test or use public transport as long as you feel back to your normal self. You will not need anyone to look after you.
Entonox is not suitable for everyone (particularly if you have COPD or a collapsed lung). You can discuss your options of Entonox or sedation with the nurse or your endoscopist before your test, or alternatively ring the department for advice (see telephone numbers at the end of this leaflet).
Occasionally, your procedure will be carried out under a general anaesthetic. Your appointment letter will inform you if your procedure has been arranged with a general anaesthetic.
There are known adverse effects from the intravenous drugs administered during the procedure, ranging from mild and common to rare and serious. These include: headaches, nausea, fainting, depression of respiratory and nervous system, which may result in aspiration pneumonia, anaphylaxis and coma. Although these serious complications are rare, they are common in patients with deeper sedation and / or general anaesthesia.
What preparation will I need for my Colonic Dilatation?
For the endoscopist to see the bowel wall clearly, it is essential that the bowel is completely empty. You may be asked to drink a preparation such as “Kleen Prep” or “Moviprep” to clean your bowel. Sometimes, the doctor may decide that you also need an enema to clear the bottom half of your bowel.
If you are preparing for your procedure at home, your bowel preparation medicine and instruction sheet will have been sent to you. Please follow the instruction sheet carefully. It is very important that this preparation works, failure to follow these instructions may result in an unsuccessful procedure.
You will need to wear a gown and remove any tight clothing for your comfort. Please inform the nurse or endoscopist about any allergies or reactions to medications you may have had.
Back to topDo I keep taking my tablets?
You must keep taking any essential tablets as normal.
- If you are taking iron tablets (ferrous sulphate), please stop them 5 days before your test.
- Please telephone the Endoscopy Unit if you are diabetic, have sleep apnoea or are taking tablets that prevent blood clots. Examples of blood thinning tablets are Warfarin, Aspirin, Clopidogrel (Plavix), Dipyridamole (Persantin), Prasugrel (Efient), Ticagrelor (Brilligue), Dabigatran, Apixaban, Rivaroxaban, Edoxaban or Acenocoumarol (Sinthrome).
- Women taking the oral contraceptive pill should be aware that taking bowel preparation might prevent the absorption of the pill. Additional contraceptive precautions should be taken until the next menstrual period begins.
Please continue to take all your other medication as normal.
Will I need to stay in hospital after my Colonic Dilatation?
The doctor doing your colonic dilatation will decide if you will need to stay in hospital after your procedure. You should expect to stay in hospital overnight, this is only for observation and to ensure that you have no problems after your procedure.
Your appointment letter will inform you if you have to stay in hospital. If you are, you should arrange for someone to collect you from the ward the following day.
If you are not staying in hospital and having sedation, you must bring someone with you and also go home in a car / taxi, not on public transport as you may be unsteady on you feet due to the sedation. You must also have someone at home to care for you for 24 hours and must rest indoors. This means no work, no driving, no alcohol and you shouldn’t operate machinery. Sedation will not be given if the above are not arranged before the test.
What should I bring on the day?
You may wish to bring your dressing gown and slippers. You will be asked to change into a hospital gown that is open at the back, before your test.
Please bring a list of medication that you take and also any medication that you may require, whilst in the department such as GTN spray, inhalers and insulin. Please do not bring valuables to the department or wear lots of jewellery. Please can you also ensure that you remove nail varnish as this interferes with the signal we receive from our monitors about your oxygen levels.
What will happen on the day of the procedure?
When you arrive at the Endoscopy Unit, your personal details will be checked. The assessment nurse will check your medical history and any allergies. You will be able to ask any questions and discuss any worries or questions that you have about the test. You will be asked for your consent form, which will be attached to your medical notes and taken into the procedure room with you, the endoscopist will discuss the procedure and allow you time to ask questions. If you have not already done so, you will be asked to sign the consent form for the procedure.
Back to topWhat happens in the procedure room?
You will be greeted by two nurses who will remain with you during the test. You will be asked to remove any dentures or glasses and lay on a trolley on your left-hand side with your knees slightly bent towards your chest. You will be given some oxygen via a small cannula that sits in your nose and your pulse and oxygen levels will be monitored by a probe placed on your finger during the test. If you are having sedation, a cannula will be put into your arm so that sedation can be given. If you have chosen Entonox, you will be shown how to use it.
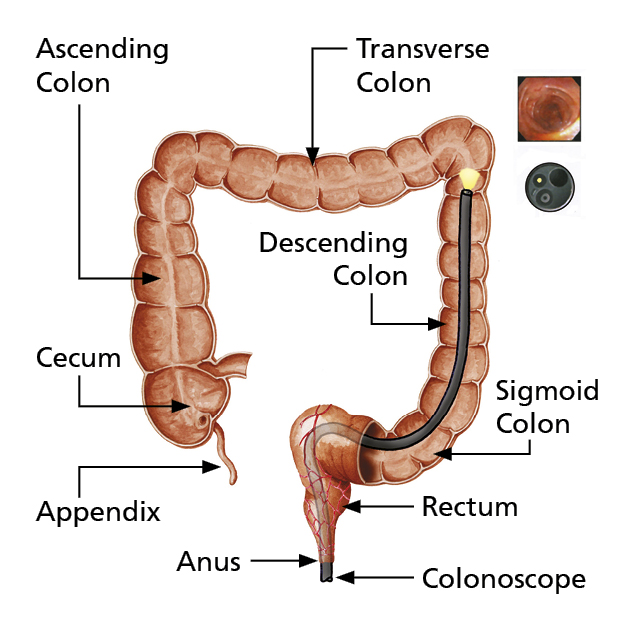
When you are comfortable, a colonoscope (camera) will be passed in to the bowel and advanced to the area that is narrow. A wire is then passed through the endoscope and across the narrowed area. A thin balloon is then passed over the wire and through the narrowed part of your bowel. The balloon is then inflated to stretch the narrowing. In some cases, the procedure is carried out under x-ray guidance.
If you are finding the procedure more uncomfortable than you would like, please let the nurse know and you may be given more medication to make you feel comfortable.
Please note
All hospitals in the trust are teaching hospitals and it may be that a trainee endoscopist performs your procedure under the direct supervision of a consultant, registrar or nurse practitioner.
What happens after the procedure?
You will be transferred to the recovery room after the procedure. The length of your stay is dependant on how you recover from the procedure and from any sedation you have been given. The nurse in the recovery room will monitor you during this period. If you are staying in hospital, you will be transferred to the ward when you have recovered. If not, you will be allowed home when the nurse in recovery is happy with your progress.
Any discomfort will soon disappear and no painkilling medication should be needed after the procedure.
Remember: if you are going home, you will need an escort with you, transport home and someone to look after you for 24 hours after the test.
You must not
- drive a vehicle;
- drink alcohol;
- operate machinery;
- sign legal documents; and
- go to work.
The recovery nurse will prepare you for discharge home and give you after-care instructions.
When will I get my results?
A full report of your procedure will be offered to you after the procedure. Another copy will be sent to your consultant and to your GP. The endoscopist or nursing staff will usually have the opportunity to speak to you after the test regarding the results.
What should I do if I become unwell after the procedure?
If you experience any unusual pains in the abdomen, not relieved by passing wind or significant bleeding from the back passage following your dilatation, you should go to the nearest hospital Emergency department. Bleeding or perforations can occasionally present several days after the procedure took place.
For further information or advice during office hours, please contact us on one of the direct numbers below (9.00 am – 5.00 pm). For advice, outside of normal office hours, you should contact your GP or the agency providing out of hours care on behalf of your GP.
LGI Endoscopy
St. James’s Endoscopy
This leaflet has been designed as a general guide to your test. If after reading this you have any questions that you feel have not been answered, please contact the Endoscopy department on the numbers below.
Administration Team
For any enquiry about your appointment including cancellation. Also, contact this number if you require an interpreter or transport. Monday – Friday, 9.00am – 4.00pm
Nursing Team
Please contact this number if you would like advice on your medication, your bowel preparation or any other medical question or worry. Monday – Friday, 9.00am – 4.00pm