Developmental Dysplasia of the Hip (DDH) is a condition where the hip’s “ball and socket” joint does not form properly in babies and young children.
What is Developmental Dysplasia of the Hip (DDH)?
DDH was previously known as congenital dislocation of the hip (CDH). The name was changed because many hips are not dislocated at birth (congenital) but become dislocated due to abnormal growth (dysplasia) of the hip joint as the child develops. Because it is a spectrum of conditions from mild shallow acetabulum or socket (dysplasia) through a complete displacement / dislocation of the femoral head (ball); hence, developmental dysplasia more accurately describes this condition.
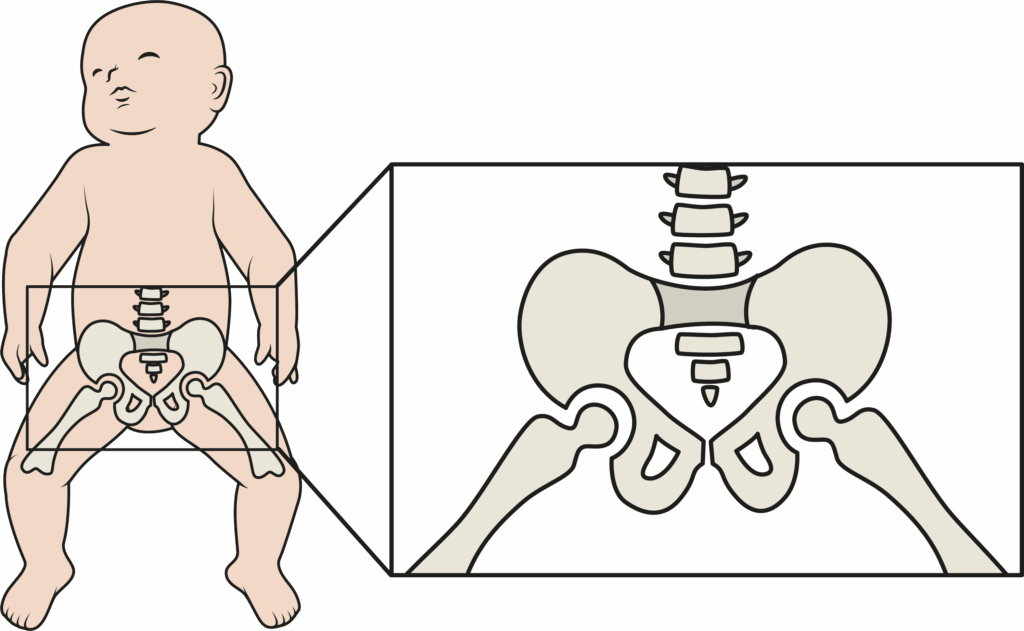
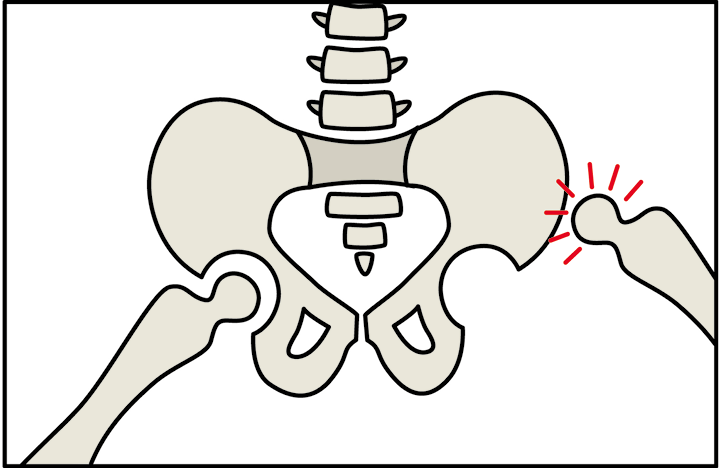
The hip joint consists of a ball-shaped upper end of the thigh-bone (femoral head) and a cup-shaped socket (acetabulum) in the pelvis, which normally fit together snugly as shown in Figure 1.
DDH, may lead to abnormal hip development. Like many other conditions, DDH can vary in severity.
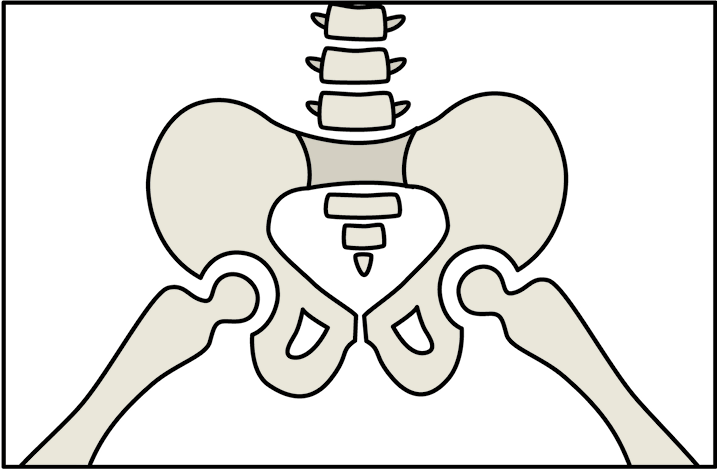
- In the mild form, the acetabulum is too shallow, being shaped like a saucer instead of a cup (Figure 2). In these cases, the hips are said to be dysplastic.
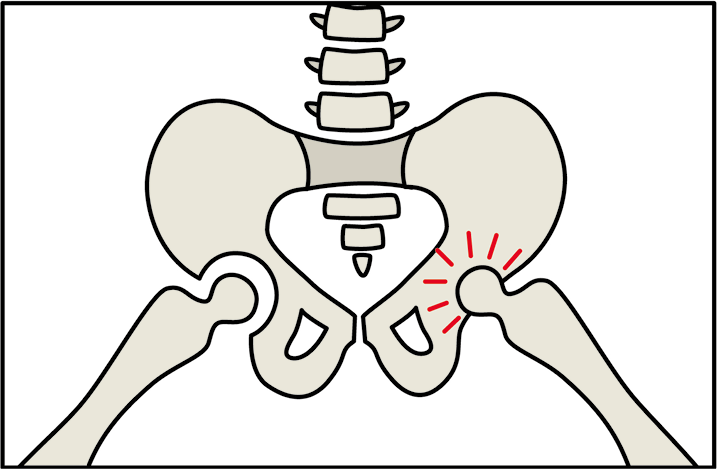
- In subluxated hips, the femoral head comes partially out of its socket, making the joint unstable (Figure 3).
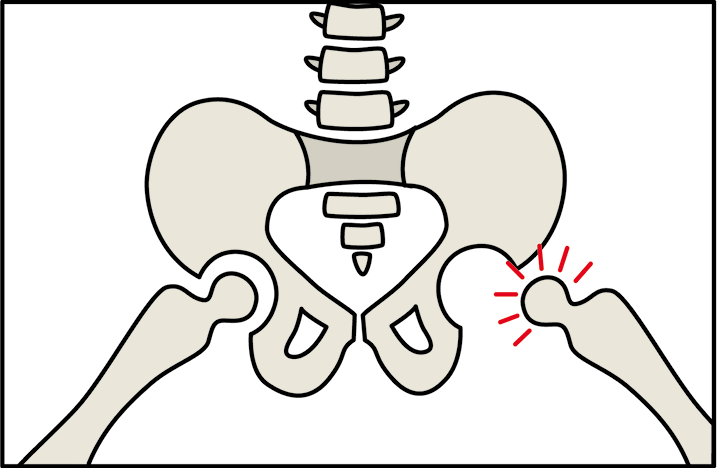
- The hip is said to be dislocated when the femoral head rests completely outside the acetabulum (Figure 4).
The hip joint abnormalities in DDH
 What causes DDH?
What causes DDH?
The exact causes are unknown. DDH may develop between birth and the time of walking. It is most commonly caused by looseness (laxity) of ligaments which hold together the hip joint or a shallow socket (acetabulum), which may allow the femoral head to dislocate. DDH is more commonly one-sided but in 35% of cases, both hips are affected.
Back to topSome risk factors for DDH
- Girls are 4 – 5 times more likely to be affected than boys.
- It is more common in first-borns (six in 10).
- Breech presentation (bottom-first position).
- There is a familial tendency.
How common is DDH?
- One in 10 infants are born with hip looseness but 80% of them become stable within a few weeks.
- One in 100 infants are treated for hip dysplasia.
- One in 500 infants are born with a completely dislocated hip.
How is DDH detected?
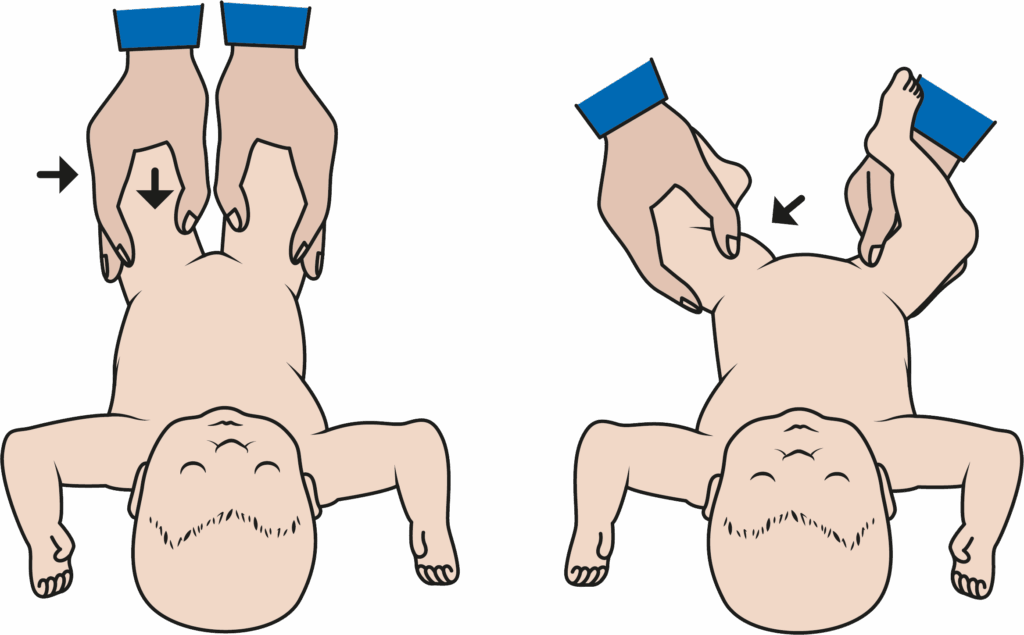
As with many other conditions, the earlier DDH is detected, the easier it is to treat and the better is the prognosis. It is a painless condition and the signs are subtle. Children are examined by a doctor for hip instability at birth, 6 weeks and about 12 months of age. The doctor performs some simple manoeuvres to test the stability of the infant’s hip joints as shown in Figure 5. By moving the infant’s legs into various positions, the doctor is able to detect if the hip joints are dislocated or loose.
Infants who have specific risk factors for DDH such as a family history or breech presentation also have their hips assessed with an ultrasound scan within the first 2 months of birth.
In children over 6 months of age, the hips are starting to change from cartilage to bone and DDH can be detected with an x-ray. Unfortunately, even with these examinations, not all children are diagnosed before they begin to walk. In addition, some older babies develop hip dislocation due to unknown causes.
What are the symptoms and signs of DDH, in a child?
DDH may be suspected in children in whom one leg appears shorter than the other, or if there are asymmetric skin creases in the inner thigh or buttock. With the onset of walking, a child with undiagnosed DDH may walk with a limp or with the affected leg looking outward, although this is painless. There will also be some restricted movement in the affected hip. Hip clicking could be normal or a sign of DDH.
If your doctor thinks your child might have DDH, they will refer you to an orthopaedic surgeon (bone specialist) who will check your child’s hips, make a diagnosis and start any treatment if necessary.
Back to topWhy is it important to diagnose and treat DDH?
Hips that are abnormal after the newborn period and remain untreated wear faster than normal hips. Adults with untreated DDH will walk with a limp, have legs of unequal length and may develop early arthritis in the hip.
What is the treatment for DDH?
Essentially, the treatment for DDH aims to put the femoral head (the ball) back into the acetabulum (the socket) as early as possible and to hold the joint in place until it becomes stable.
A stable hip joint will allow the bones to develop normally.
The methods used to achieve this depend on the age of the child.
Age: 0-6 months
In some infants with mild laxity just after birth, the hips stabilise on their own within the first 2 – 6 weeks of life and no interventions are necessary. For children in whom this does not occur, the treatment involves placing the child in a Pavlik harness, shown in Figure 6. This is a Velcro splint that gently holds the hips up and outwards to help normal development of the acetabulum or ‘socket’.

The Pavlik harness is worn continuously for 6 week periods and is successful in 90 – 95% of cases. Treatment stops when the ultrasound is normal. A small minority of children may require an operation.
Back to topAge: 18 months – 3 years
In this age group, treatment is more difficult because the soft tissues around the hip have tightened and these older children are too big for a Pavlik harness.
Some of the tight tendons around the joint may need to be lengthened before attempting to place the hip back into position with closed or open surgery and hold it with a hip spica cast (Figure 7). These procedures are done under general anaesthesia. If this treatment is unsuccessful, then further surgery may be required.

Age: 18 months – 3 years
Surgical treatment is almost required for children with persistent or with previously undetected DDH in this age group. In addition to the open reduction of the hip into the socket, bone re-shaping procedures of the pelvis and sometimes, the femur (the thigh-bone) are required. Then, the position is protected in a hip spica cast. As a general rule, the earlier the treatment in this age group, the better the results.
Age: over 3 years
For children with late presentation or recurring cases, there are various procedures which can be performed and you can discuss with your orthopaedic surgeon which is the best for you and your child. Whilst at this stage, the treatment is technically more demanding, the long-term outcome can still be good but it depends on the severity of the dysplasia and the age of your child.
Tips for parents
- Don’t panic! Most cases of DDH are treated successfully and without operation.
- Please ask questions.
- Follow instructions about harnesses and casting carefully.
- Treat your child as normally as possible and encourage your child to resume normal activities as soon as medically recommended.soon as medically recommended.
 Useful contact numbers
Useful contact numbers
If you have any questions or concerns, please contact: