EMR is a useful endoscopic method for removing flat tissue from the lining of the food pipe, stomach or small bowel.
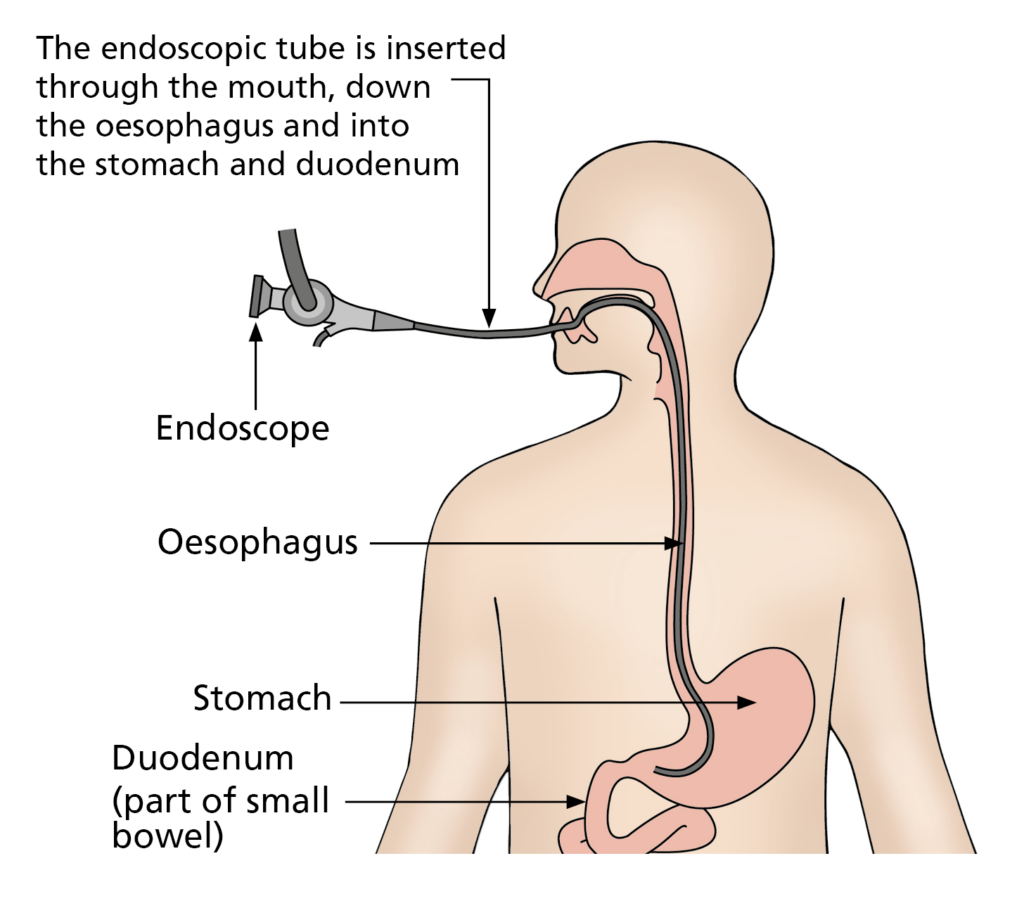
The procedure will be carried out using a gastroscope (flexible camera) that is passed through the mouth to access the area of irregularity. When the lesion or polyp has been located, it is raised by injecting fluid into the tissue underneath the lesion. The injection increases the thickness of the gut wall, making it easier and safer to remove the lesion.
The lesion is then removed using diathermy (heat treatment), which allows the lesion, along with some of the tissue underneath to be cut. This is a useful endoscopic method for removing flat tissues from the lining of the food pipe, stomach and small bowel. You will not feel this.
Why am I having an EMR?
Your previous endoscopy or test has found a lesion or polyp in your oesophagus (gullet), stomach or duodenum (small bowel). In most cases, biopsies (small samples of tissue) have already been taken and sent to the laboratory for analysis. Sometimes, these samples are too small for the laboratory to make a diagnosis and a larger sample is required for a more precise diagnosis. Alternatively, the previous biopsies have indicated that the lesion requires removal.
All tissue samples have to be sent away to the laboratory so the results will not be available straightaway. You will be able to discuss the results of your EMR with the doctor who referred you.
What are the benefits to having an EMR of the digestive tract?
The main benefit of this procedure is that the lesion can be removed without the need for a major operation. In the majority of cases, the EMR is performed as a day case procedure, which means you are discharged after a few hours of observation following the procedure. Time taken to recover and discomfort after the procedure is far less when compared with surgery.
What are the alternatives to having an EMR of the upper digestive tract?
Alternative treatments may already have been discussed with you. These include, removing the lesion surgically by “keyhole” or “open” surgery, which means an operation. This is generally associated with a longer recovery and may carry greater risks. Alternatively, you may opt not to have the lesion or polyp removed and instead keep it under close review; however, this decision must be carefully considered after discussion with your consultant.
Will I need to stay in hospital after my EMR?
The procedure is usually undertaken as a day case but sometimes the doctor will make the decision that you need to stay in hospital after your EMR for further observation.
Your appointment letter will inform you if you have to stay in hospital. If you do, you should arrange for someone to collect you from the ward the following day.
If you are not staying in hospital, you will need an escort with you and you must also go home in a car / taxi (not public transport) as you may be unsteady on your feet.
Remember
If you have sedation, you will need an escort with you, transport home and someone to look after you for 24 hours after the test.
If you are unable to make these arrangements, please contact the Endoscopy Unit for advice as we may need to arrange a hospital bed for the night.
Do not
- drive a vehicle;
- drink alcohol;
- operate machinery (applies to sedated patients only);
- go to work (applies to sedated patients only);
- sign legal documents.
What are the risks of having an EMR?
The most common side-effect following an EMR is a sore throat for a day or two. Less commonly, you can experience rare reactions to the drugs used for sedation or anaesthesia. Very occasionally, there can be damage to crowned teeth or bridgework.
The two more serious risks are bleeding during or after the EMR and perforation (tearing) of the gut wall. This usually occurs during the procedure and is dependent on the size and location of the lesion or polyp being removed.
A recognised late complication is stricturing (narrowing) of the oesophagus (gullet) after EMR.
What preparation will I need?
An EMR must be performed on an empty stomach
Your appointment letter will tell you when you will need to stop eating and drinking. This is very important.
We may have to cancel the procedure if we find food or fluid in the oesophagus or stomach as we will not be able to see the lesion or polyp clearly.
Do I keep taking my tablets?
You must keep taking any essential tablets unless your doctor tells you specifically not to.
If you are diabetic, this should have already been highlighted by your referring doctor and you should receive additional information of what to do with your medication and the steps you need to take to prevent hypoglycemia (low blood sugar).
Please telephone the Endoscopy Unit if you have sleep apnoea or are taking tablets that prevent blood clots. Examples include: Aspirin, Clopidogrel (Plavix), Dabigatran, Edoxaban, Ticagrelor, Dipyridamole (Persantin), Warfarin, Heparin, Rivaroxiban (Xarelto) or Apixiban (Eliquis).
What should I bring on the day?
Please bring a list of medication that you take and also any medication that you may require, whilst in the department such as GTN spray, inhalers and insulin.
Please do not bring valuables to the department or wear lots of jewellery. Please also ensure that you remove nail varnish as this interferes with the signal received from equipment we use to measure your oxygen levels. If you are staying in hospital, please bring an overnight bag and any medication that you take with you.
Will I be asleep for my EMR?
EMRs of the oesophagus (gullet), stomach or duodenum (small bowel) are usually carried out with sedation, which means that you will be relaxed but not asleep. In addition, we offer a local anaesthetic spray to reduce any discomfort in your throat.
In most cases, it is possible to carry out an EMR with sedation; however, some larger lesions or polyps can take up to one hour to remove and can be uncomfortable. These may be removed whilst you are under general aesthetic (GA).
There are known adverse effects from the intravenous drugs administered during the procedure. These range from mild and common (for example, headache, nausea, dizziness) to rare and serious (for example, depression of respiratory and nervous system, which may result in aspiration pneumonia, anaphylaxis and coma. Although these serious complications are rare, they are more common in patients with deeper sedation and / or general anaesthesia.
Your appointment letter will inform you if a general anaesthetic has been arranged for your procedure.
What will happen on the day of the test?
When you arrive at reception in the Endoscopy Unit, your personal details will be checked. The assessment nurse will collect you and take your medical history, discuss and explain the test, and take your blood pressure and pulse.
You will be asked for your consent form (supplied with this leaflet). This will be attached to your notes and taken to the procedure room. Please make sure that you have read the consent form through before you come for your procedure as when you sign your consent form, you are agreeing that this is a procedure you want. Remember, you can change your mind about having this procedure at any time. The endoscopist who will be performing your EMR will meet you before the procedure. You will be able to ask any questions and discuss any worries you may have.
If you are staying in hospital after your EMR, there may be a wait before your procedure as we will need to confirm that a bed is available for you afterwards. The nursing staff will keep you informed about when a bed may be available for you.
Please note:
Every effort will be made to see you at your appointment time; however, due to hospital inpatient emergencies, delays may occur. The endoscopy staff will keep you informed of any delays.
What happens in the procedure room?
You will be greeted by two nurses who will remain with you during the procedure. The team in the room will complete a checklist to ensure all your information is correct.
A cannula will be placed in your vein so that sedation or anaesthetic can be administered. You will be given oxygen through a small plastic tube in your nose and your throat will be numbed with an anaesthetic spray. You will then be asked to remove any dentures or glasses and lay on a trolley on your left-hand side. Your pulse and oxygen levels are monitored by a probe placed on your finger during the test.
Before the test starts, a plastic mouthpiece is placed between your teeth to keep your mouth slightly open. With sedation, the drugs used are a combination of Midazolam, a sedative to relax you and Fentanyl, a painkiller.
When the endoscopist gently passes the endoscope through your mouth, you may gag slightly. This is quite normal and will not interfere with your breathing. During the procedure, air is put into your stomach so that the endoscopist can have a clear view.
This may make you burp a little, some people find this uncomfortable.
Any saliva or other secretions produced during the procedure will be removed using a small suction tube, like the one used at the dentist. When the procedure is completed, most of the air is removed and the endoscope is removed quickly and easily. If you become very uncomfortable or withdraw consent, the procedure will be stopped.
Please note:
All hospitals in the trust are teaching hospitals and it may be that an endoscopist training to do EMR performs your procedure under the direct supervision of a consultant. Student nurses, doctors or medical representatives involved with the equipment used during the procedure may also be present during your procedure to observe the test. If you do not wish them to be present, please inform the endoscopist.
What happens after the test?
You will be transferred to the recovery room after the test. The length of your stay is dependant on how you recover from the procedure. The nurse in the recovery room will monitor you during your recovery, prepare you for discharge and give you aftercare instructions. This can take 2-3 hours. You will be discharged home when the recovery nurse is happy that you are ready to be discharged.
If you are staying in hospital after your EMR, you will be transferred to the ward when you have recovered.
Most patients feel some discomfort in the chest or upper abdomen for a few days following the procedure. The Endoscopy Unit will provide you with an information sheet of the best way to manage this. You will be able to restart most of your normal medications immediately following the procedure. If you are taking blood thinning medications, then the endoscopist will decide when it should be safe to restart this medication.
When will I get my results?
You will receive a copy of the endoscopy report before discharge and this will also be sent to your consultant and GP.
The removed lesion will be looked at under the microscope and the result of this will normally be available 1 – 2 weeks following the procedure. You will be contacted with these results, either by a letter, or you may be asked to attend a clinic. All enquiries regarding your outpatient appointment should be directed to your consultant’s secretary. If you feel that you are waiting a long time for an appointment to discuss your results, your GP will also have a report so you can see them too.
In most cases, we would recommend a follow-up endoscopy around six months after the procedure to confirm that the lesion has been completely removed. This procedure may be carried out in your local hospital or in Leeds.
What should I do if I become unwell after the procedure?
Bleeding or perforations can occasionally present several days after the procedure has taken place. If you experience any severe pain in the abdomen, not relieved by passing wind, nausea, vomiting or bleeding, fresh or altered blood via your back passage following your procedure, you should go to the nearest Emergency department, and bring a copy of your endoscopy report with you so the doctors know what procedure you have had.
This leaflet has been designed as a general guide to your procedure. If after reading this, you have any questions that you feel have not been answered, please contact the Endoscopy department on the numbers below.
Administration Team
for any enquiry about your appointment including cancellation. Also, contact this number if you require an interpreter or transport.
Nursing Team
Please contact this number if you would like advice on your medications or any other queries concerning the procedure.