What is an Abdominal Aortic Aneurysm (AAA)?
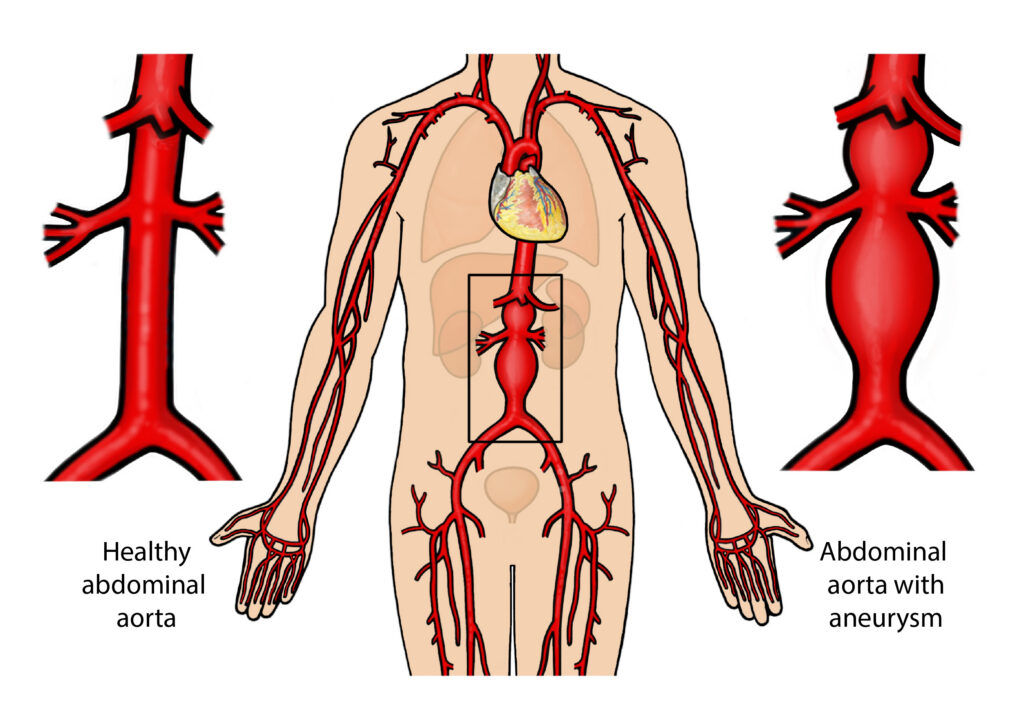
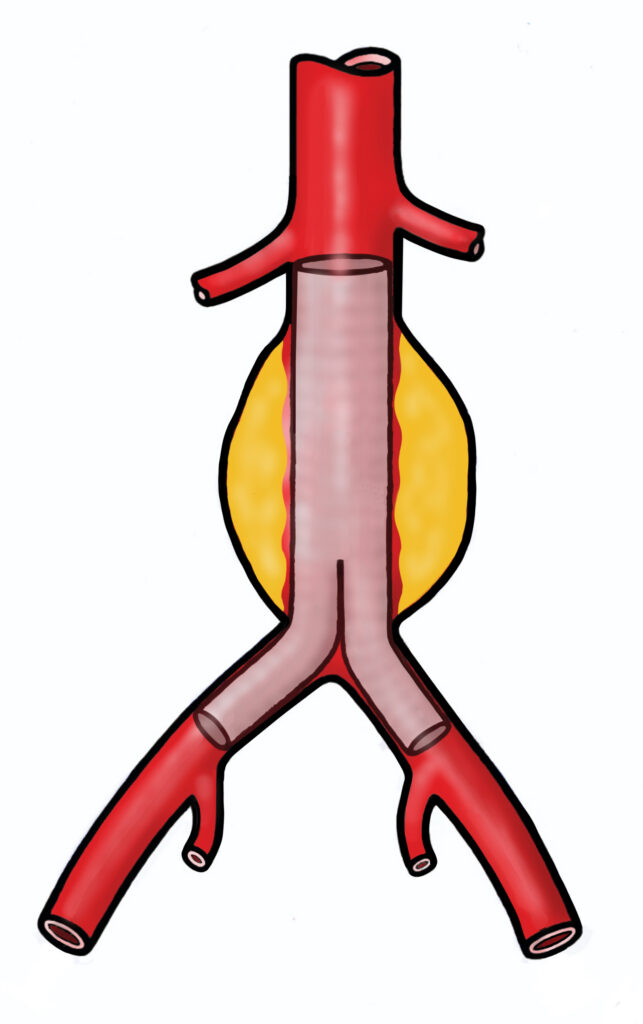
The aorta is the main blood vessel from the heart. When the artery wall weakens, it can develop a swelling, commonly in the abdominal aorta (the region of the aorta which passes through the abdomen).
When this occurs, it is called an abdominal aortic aneurysm (AAA).
This condition is most common in men over 65 who are therefore routinely invited for ultrasound screening. Women and younger men are less frequently affected.
Small aneurysms tend to be assessed with ultrasound to monitor their size. If the aneurysm reaches a size of 5.5cm there is a small chance that they could burst (rupture), this can be life-threatening, so treatment is considered to prevent this from happening.
There are two broad treatment options:
- Open surgical repair.
- Endovascular Aneurysm Repair (EVAR) which is a “key-hole option”.
How do I prepare?
On the day of the procedure, you will be admitted to a ward before going to the operating theatre. Your team will check you in, and you can ask any questions you have. You will need to fast if you require general anaesthesia or sedation. You will be given an antibacterial wash to use for the days leading up to your surgery to minimise the risk of infection. A cannula will be inserted into a vein for medications during the procedure. A urinary catheter may also be needed.
How is it performed?
EVAR works by relining the aorta. Stents are placed inside the aorta to exclude the aneurysm from circulation.
Consent
An EVAR usually takes between 2 – 4 hours, though every patient is different, and some procedures can take longer. The operator will explain this to you in more detail, along with the risks and intended benefits before you provide your permission to go through the operation via a signed consent form.
Anaesthetic
The procedure can be undertaken under local, regional, or general anaesthesia. The choice of which approach will be made between you, the operator, and the anaesthetist.
Operation
Small incisions are made in the groins to allow access to the blood vessels, using x-ray guidance. Stents are placed inside the aorta to exclude the aneurysm.
The stent starts above the aneurysm and ends below it, sealing the aneurysm. Blood can flow freely through the stent, but the aneurysm is prevented from growing further or rupturing. This procedure avoids open abdominal surgery, which gives quicker recovery time.
Depending on your individual anatomy, your doctor may recommend that you undergo a Fenestrated Endovascular Aneurysm Repair (FEVAR) or a Branched Endovascular Aneurysm Repair (BEVAR). The procedures are carried out in the same way, but additional stents are implanted to maintain blood supply to organs such as your liver, intestines, and kidneys. Your doctor will discuss the type of EVAR most suitable for your aneurysm.
Staff involved
Interventional Radiology (IR) procedures are performed by a multidisciplinary team. The team includes the following key Staff:
- Interventional Radiologist (Consultant/Fellow): A doctor specially trained in minimally invasive, image-guided techniques who performs the procedure.
- Radiology Nurses: Highly trained nurses who care for the patient before, during, and after the procedure. They assist with sedation, monitor vital signs (heart rate, breathing, oxygen levels), and may “scrub in” to assist the radiologist directly.
- Radiographers: Experts in imaging equipment who operate the machines to provide real-time guidance for the doctor.
- Senior Clinical Support Workers (SCSWs): Assist with the setup of the room, patient positioning, and maintenance of sterile conditions.
What are the risks?
There are risks involved with any procedure and your doctor will discuss them with you before you consent to the procedure.
Common
- Groin bruising and mild post operative discomfort.
Rare
- Nephrotoxicity – x-ray dye can reduce kidney function, this is usually transient.
- Significant endoleak – a leak around the stent.
- Blood vessel injury.
- Future reintervention.
Very rare
- Severe allergic reaction.
- Stent infection.
- Heart attack, stroke, blood clot and death.
What to expect from this operation?
Admission
You come to the hospital on the day of the procedure. You must not eat or drink anything for six hours before surgery.
When you come into the hospital, bring the following items in a small, labelled bag: all your medications (including insulins and inhalers), nightwear and changes of clothes, toiletries, dentures, glasses, and hearing aids. There is limited storage space on the ward, so keep the bag small. We recommend that you do not bring valuables with you.
Recovery
After surgery, you will be transferred to the post-anaesthetic care unit (PACU) and in due time can be moved on the ward or, if needed, the high dependency unit (HDU). Pain relief medication will be given as needed.
Aftercare
You can eat and drink normally after surgery and will be encouraged to move around as soon as possible. Most people stay one night in the hospital after EVAR. Blood tests and a team check-up the next day will determine if you can go home. If you have a more complex FEVAR or BEVAR, expect a longer hospital stay of about three days.
Before discharge, a doctor will advise on pain relief. Most EVAR patients can go home the day after the procedure, but recovery can be slow and tiring. Discuss support options with your doctor, family, and GP. Groin stitches are usually dissolvable and do not require removal.
Care at home
Full recovery after an EVAR is usually two weeks, but can be up to two months, depending on your age and general fitness. It is important to have restful periods and gradually increase your activity each day. Discuss your support options with your doctor, family, and GP to prepare for the recovery period.
- Exercise – Start slowly, avoiding heavy lifting and strenuous activities initially. Walking is excellent for recovery, benefiting your muscles, heart, and lungs. Begin with short walks, gradually increasing your activity. You can manage light tasks at home, in the garden, and at work when you feel able. Excessive activity may cause pain but is very unlikely to cause damage.
- Work – Most people can return to work two weeks after their procedure, though it may take longer. Speak to your GP for advice and a fit note if you need time off.
- Driving/travel – If you have had to surrender your driving license prior to the operation due to the size of your aneurysm, you will have to reapply for a license prior to resuming driving.
- Medicines – You will probably be prescribed aspirin which can help to prevent blood clots by thinning the blood and a statin to lower cholesterol. These medications help reduce the risk of further arterial disease and are usually taken for life.
- Follow-up – We will arrange for a CT scan one month after your procedure, we will review you and your scan a couple of weeks after this in clinic, either by telephone or face to face. If everything is satisfactory, you will then be on lifelong annual surveillance, initially with a CT scan at one year and then by annual ultrasound alone.
- Please seek immediate medical attention if you experience severe symptoms such as uncontrollable pain, oozing or reddening around the wound site, which could indicate a wound infection.
Contact information
We hope some of your questions have been answered by this leaflet. If there are any questions you would like to ask before you come for your operation, please get in touch.
Interventional Radiology LGI
Ward 15 LGI
Aortic Coordinator
Your GP or NHS direct
How to get to our department
We are located in the Jubilee Wing of LGI, Ground Floor.