This leaflet is for patients, parents and carers considering female fertility preservation.
Please ask your nurse specialist or doctor any questions. We are here to help.
More information is available on our website:
What is fertility?
Fertility is the ability to have children. After your periods have started it is possible to get pregnant naturally. Periods are the sign that your ovaries have started to release their eggs. You have two ovaries, which contain millions of eggs, and all the eggs you will ever have are in your ovaries from when you are born. As you get older, the number of eggs reduces until, by around the age of 50 years old, when they have all gone. Your periods will stop and your hormone levels will change and this is known as the menopause.
Sometimes you may be at risk of losing your eggs more quickly due to a medical condition or treatment for an illness, for example:
- Turner’s syndrome.
- Sickle Cell Disease.
- Thalassaemia.
- Chemotherapy or radiotherapy.
Sometimes the medical condition or the treatment can mean that your ovaries and eggs are damaged before your periods even start and you may have an early menopause.
Your eggs are important as they contain half of the building blocks, or genetic material needed to develop into a baby. Your egg needs to join with a sperm to complete the building blocks that are needed to create a baby.
Your doctors are concerned that your medical condition or treatment may mean that your eggs and fertility are at risk of damage. It may not be possible for you to have a baby naturally when the time is right for you. We are here to talk to you about your options to try and protect your fertility.

What is fertility preservation?
It can be really hard to know who will have problems having a baby. This depends on the condition you have, your age and what treatments you need to have.
The fertility clinic can offer you treatments to try to protect your chances of getting pregnant and having a baby in the future.
There are different options depending on your circumstances. These can include:
a) Freezing individual mature eggs.
b) Freezing of whole or part of an ovary containing
immature eggs.
c) Medication to try to protect your ovaries during chemotherapy.
Freezing individual eggs
After you have gone through puberty your hormones make the ovaries release eggs. One egg is developed each month and when it is not fertilised the period comes.
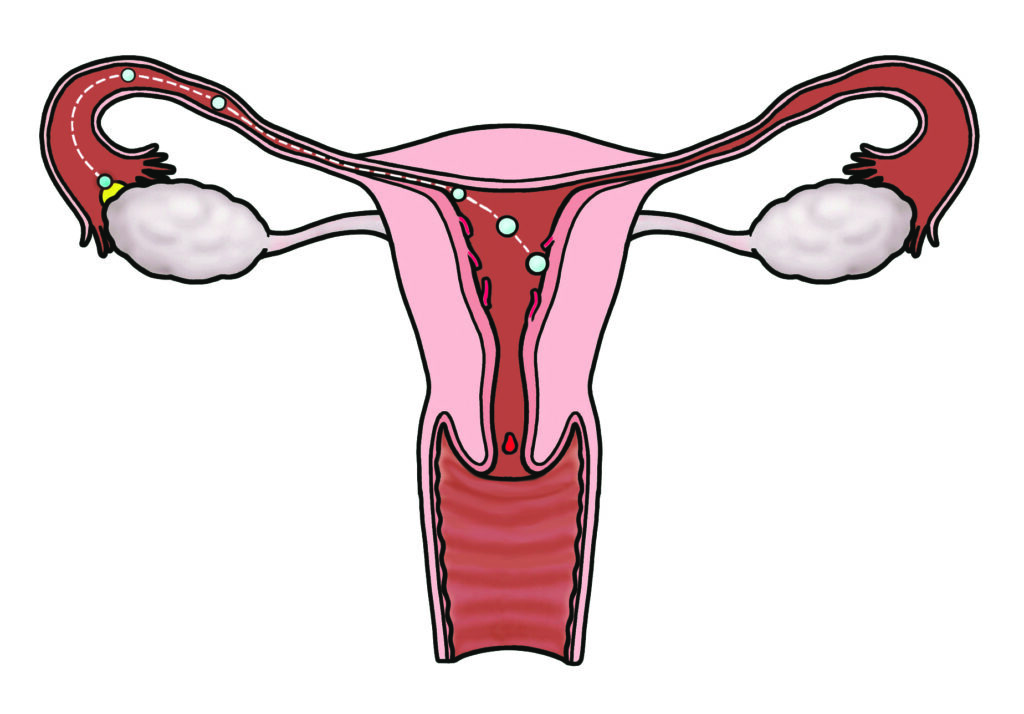
It is possible to make the ovary produce 10-15 eggs at the same time with extra hormone treatment. This is done with small injections into the skin of the tummy or thigh over
10-12 days.


After your ovaries have been stimulated your eggs need to be taken out in order to be frozen. The procedure requires some sedation and pain relief or an anaesthetic. It takes about 20 minutes. Your eggs come out through a needle that either goes through the tummy or the skin inside the vagina.
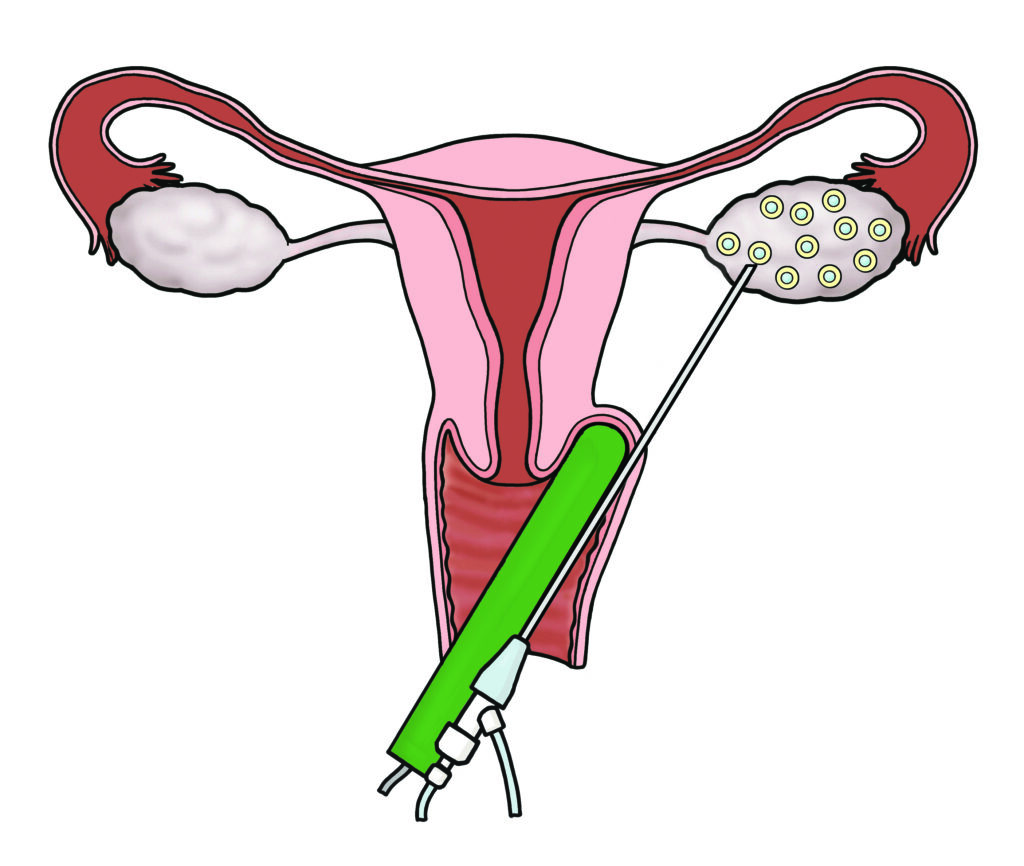

After your eggs have been taken out an embryology scientist will clean and process them for freezing. Your eggs are then safely stored at the fertility clinic until you want to think about having a baby.

How are my eggs used to have a baby in the future?
When you are ready to try to get pregnant, your eggs will be thawed and each injected with a sperm to try to fertilise them.
The embryos (fertilised eggs) that result will be looked after in the fertility laboratory for five days.
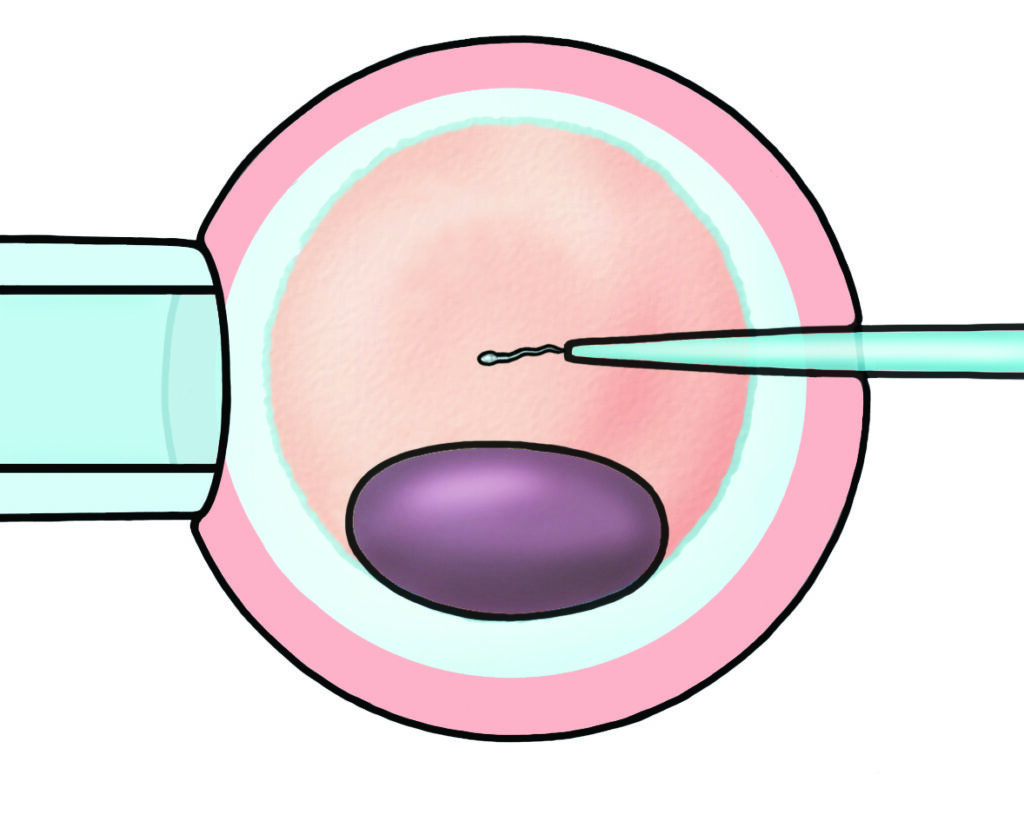

Not all of your eggs will be suitable for injection with sperm. Not all of these will fertilise normally. During the 5 days of laboratory growth and observation, not all of these will continue to develop normally. This is why quite a large number of eggs is needed to have a reasonable chance of a good-quality embryo being made, which may then have a good chance of developing into a baby.

Not all of the eggs harvested will fertilise; not all those fertilised will continue to divide and grow; not every embryo returned to the womb is strong enough to implant and produce a pregnancy.
The scientists will identify the best embryo and the doctor will put it into your womb. If there is more than one good one, the others can be frozen again for use at a later date.
Unfortunately this treatment does not always result in a pregnancy, but hopefully you will have produced several embryos to have several attempts.
Embryo transfer is a quick and painless procedure similar to having a smear test.

Freezing part or all of one ovary
It is possible to remove an ovary or small pieces of your ovary before any treatment that could damage your fertility starts. This is done with an operation under a general anaesthetic (asleep). Doctors remove the ovary / piece of ovary by keyhole surgery.
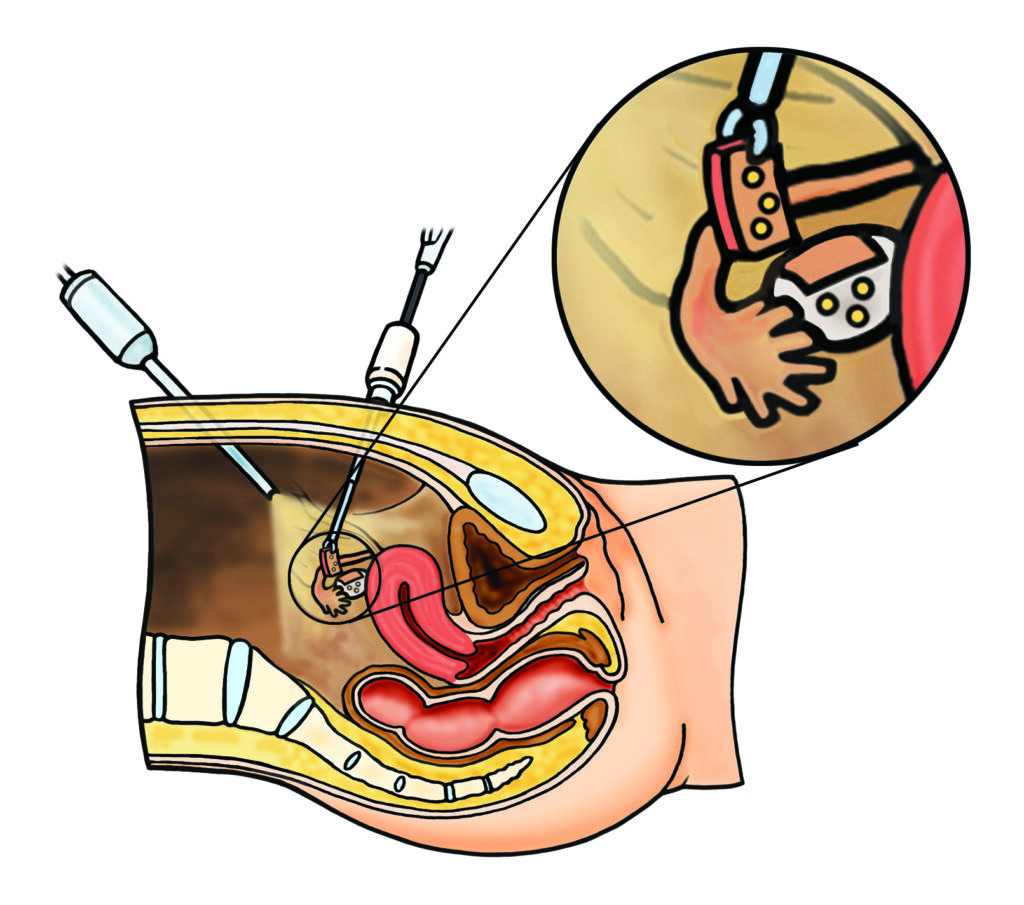
The tissue containing your eggs is then frozen and stored. These pieces of ovary contain thousands of immature eggs. After your other treatment has been completed, and you have recovered you may decide to try to have a baby.
This could be many years later.
The pieces of ovary can be put back into your body. This can make it possible to conceive naturally or with fertility treatment. This technique is suitable for most people and it is especially suitable if you have had to start fertility-damaging treatment quickly or before you have reached puberty.
It may not be suitable if there might be cancer cells already in your ovary or cancer cells that might be carried to your ovary in the blood (e.g. leukaemia) which could be reintroduced years after you have been cured.
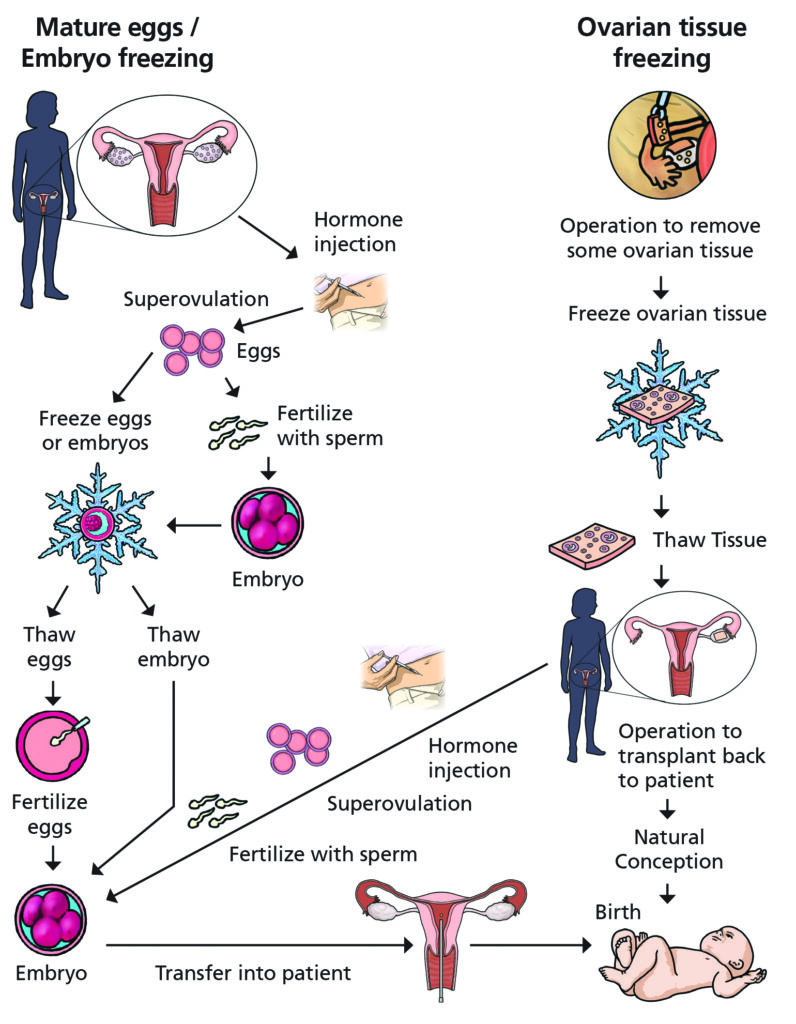
Summary of fertility preservation options
How is my frozen ovary used to try to have a baby in the future?
This is a newer technique and it isn’t widely available in the UK. Only a few hundred babies in the world have been born using this method. There are not many people who have tried to use their samples yet because the tissue was stored when they were young and they are still growing up.
We expect that more young people will want to use their stored tissue in the future. We know that it is possible to return some ovary years later as a ‘transplant’ and it produces normal hormones and eggs, for a little while (months or years).

During this window of time it is possible to get pregnant and have healthy babies, naturally or with the assistance of fertility (test-tube baby / IVF) doctors. Depending on how much ovary is taken, it may be possible to have several transplants one after the other to lengthen the time of hormone and egg production, and to try to have more than one child.
In the future, it may be possible to mature eggs from the thawed ovary in the laboratory (in vitro maturation IVM). The eggs would then be fertilised outside the body (ICSI) and the embryo transferred to you. Scientists are working on this now but this technique has not been successful yet.
What are the risks?
Unfortunately there are no guarantees that everything will go according to plan. Problems can occur along the way. These could include:
Problems with getting eggs / ovary tissue out
- Failure to harvest eggs – The ovaries may be too weak to give any eggs up or the eggs that are there may be of poor quality and unsuitable to freeze.
- Complications of surgery – egg retrieval and ovarian tissue collection are usually safe and straight-forward but occasionally infection, bleeding or damage to nearby structures can happen.
Problems with the storage and thawing of the eggs / ovary
- The eggs / ovary may not recover from the freezing and thawing process.
Problems with using the samples
Eggs
Not all the eggs frozen will survive and be able to accept a sperm and fertilize properly. Not all of those that fertilise will produce healthy embryos that can become healthy babies.
The chance of a single transferred embryo producing a healthy baby is about 30-45% per attempt. When the time comes, much more information will be provided, and tailored as far as possible to your circumstances.
Ovary
There are many steps between transplanting the tissue and having a baby.
- It is not possible to be sure that many eggs (and in particular, good quality ones) will be present in the tissue to be transplanted.
- The transplanted tissue may not attach properly to be able to produce hormones and mature eggs.
- For patients who have recovered from cancer, extra tests will be done on the tissue to be as sure as we can that it is free of any cancer cells before you have it transplanted back inside you.
- You may not manage to get pregnant naturally and eventually may be advised to think about IVF.
- Separate information is available about IVF the providers’ websites: www.carefertility.com/clinics/leeds and www.leedsth.nhs.uk/services/fertility/
What are the chances that the treatment will work?
Eggs
The chances of having a baby are higher with frozen and thawed mature eggs because this technique is tried and tested and we know that it can work. Success depends on many things but especially on the genetic quality of the egg which is related to its age: the younger, the better. We also need a good number of eggs to work with (e.g. 20) as not all of them will be perfect. It is fair to say that success rates are steadily increasing and will continue to improve.
Ovarian tissue
Ovarian tissue freezing is still new and the techniques are being improved all the time. This opportunity offers hope but it is important to be realistic about the chances of success. At the moment, only a few hundred people worldwide have received their own ovarian tissue back as a transplant. About 1 in 4 managed to have a baby (half of these got pregnant naturally and half had IVF assistance).
What happens after the storage process is complete?
Maintaining contact
When you are ready to talk about possibly using your eggs / ovary tissue, we will explain the options, risks and chances of success. This will include an assessment of your natural fertility at the time.
We will keep in touch with you over the coming years to make sure that we are doing the correct thing by keeping your eggs / piece of ovary in storage.
We will confirm that:
- You still want it to be kept.
- It still needs to be kept.
- There is funding available to keep it.
- We are still legally allowed to keep it.
The next section explains the responsibilities of the Clinic in charge of storing your eggs or ovary tissue, your responsibilities and where both parties stand legally under a variety of circumstances.
Whilst these details may not seem important now, they are extremely important as time goes by, to make sure that the Clinic is able to give you accurate advice about the safe,
long-term and legal storage of your eggs.
Eggs can be stored legally for up to 55 years (in blocks of 10 years). Currently the NHS funds the first 10 years of storage.
After your eggs have been stored for nine years we will need to discuss whether they need to stay in storage and explore funding options.
Ovarian tissue is currently stored at Oxford Future Fertility Programme.
www.ouh.nhs.uk/future-fertility/patients/ovarian.aspx
What happens if I don’t want to store my eggs / ovary?
This is your decision to make with the support of your family and our Team if needed. Nothing will change in your main treatment if you decide not to store anything.
We can still see you after treatment if you want to know whether the treatment has affected your fertility.
Medication to protect your ovaries during chemotherapy
If you need chemotherapy to treat your illness, a monthly injection of a drug called Prostap may help to reduce the blood supply to the ovaries and provide some protection against the damage to the eggs that chemotherapy can do.
More research is underway to work out how effective this might be. Freezing eggs, embryos or ovarian tissue is much more likely to preserve fertility successfully and for longer.
Prostap is a hormone blocker which brings on an artificial, and temporary menopause.
Side effects can include:
- Hot flushes.
- Sweating at night which can disturb sleep.
- Headaches.
- Mood swings.
- Joint pains.
- Vaginal dryness.
Side effects are temporary and only last for the period of time that chemotherapy is needed.
If the side effects are very unpleasant and you do not want to continue, this medication can simply not be repeated when the next monthly injection would be due. If you cope well with the first month, you can have a single injection in the second month that lasts for three months for added convenience.
Is there anyone else I can talk to?
We know there is a lot of information to take in and this is a difficult time. Some people find it helpful to talk to someone who is not a close family member, friend or doctor / nurse involved in their treatment about how they feel and the decisions they are being asked to take.
You can ask to see someone by yourself or bring anyone else with you, if you prefer. Please ask if you would like to know more.
General legal information about how fertility clinics are regulated and conduct their work
The Human Fertilisation and Embryology (HFE) Act (1990, amended 2008) and the HFE Authority (HFEA) regulate all treatments involving human eggs, sperm and embryos.
The HFEA issues the Code of Practice that we work by and it inspects us regularly to ensure standards are maintained. All UK clinic results are reported to them and are publicly available (www.hfea.gov.uk).
The storage of ovarian tissue
The storage of ovarian tissue is regulated by the Human Tissue Authority under the Human Tissue Act (2004) and The Human Tissue (Quality and Safety for Human Application) Regulations 2007 (as amended).
This requires establishments storing tissue or cells intended for human use to do so under the authority of an HTA licence. (www.hta.gov.uk).
Summary
Fertility is your chance of having a baby. Some diseases and treatments can reduce your fertility. You are being asked to think about options to help protect your fertility and give you choices in the future. There can be problems with these options so there are no guarantees that it will work. This is an area which is progressing fast and is likely to get even better in the future.
We are here to support you to make the right choice for you.
Informed Consent
This leaflet is provided to supplement verbal information that will be given to you by your healthcare provider (Doctor/ Surgeon/Nurse) as part of the consent process prior to your procedure. Information sharing between you and the clinician is essential to ensure that your decision to consent is fully informed. Please ask questions if you don’t fully understand or have any concerns about what is proposed.
You have a right to be involved in these decisions and should feel supported to do so. Please take the time to consider what is important to you to ensure the information you receive is specific and individualised.
Useful resources
Contact us
Leeds Centre for Reproductive Medicine
Monday – Friday 08.00 – 17.00