We realise this is an anxious time for you and your relatives. We hope that by providing accurate information you will know what to expect before and after your operation, and feel better prepared.
If there is anything that you do not understand, have forgotten or are particularly worried about, please ask.
What is the stomach?
The stomach is a muscular baglike organ that joins the gullet (oesophagus) to the intestine. After food has been swallowed, it passes down the gullet and enters the stomach.
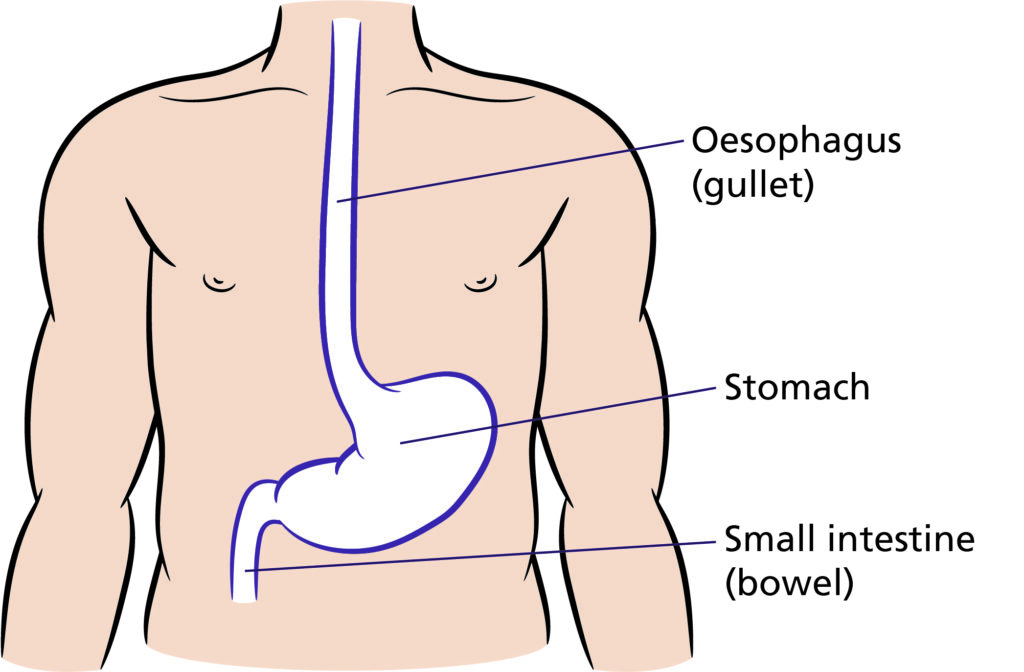
The stomach stores and mixes the food and begins the digestion process until it is passed into the intestine, where it is further digested and absorbed into the blood stream.
What does the operation involve?
This operation involves removing part or all of the stomach, (figure A and figure B) along with some surrounding tissue and lymph nodes.
Part of the small intestine is then joined to the remaining part of the stomach or directly to the oesophagus.
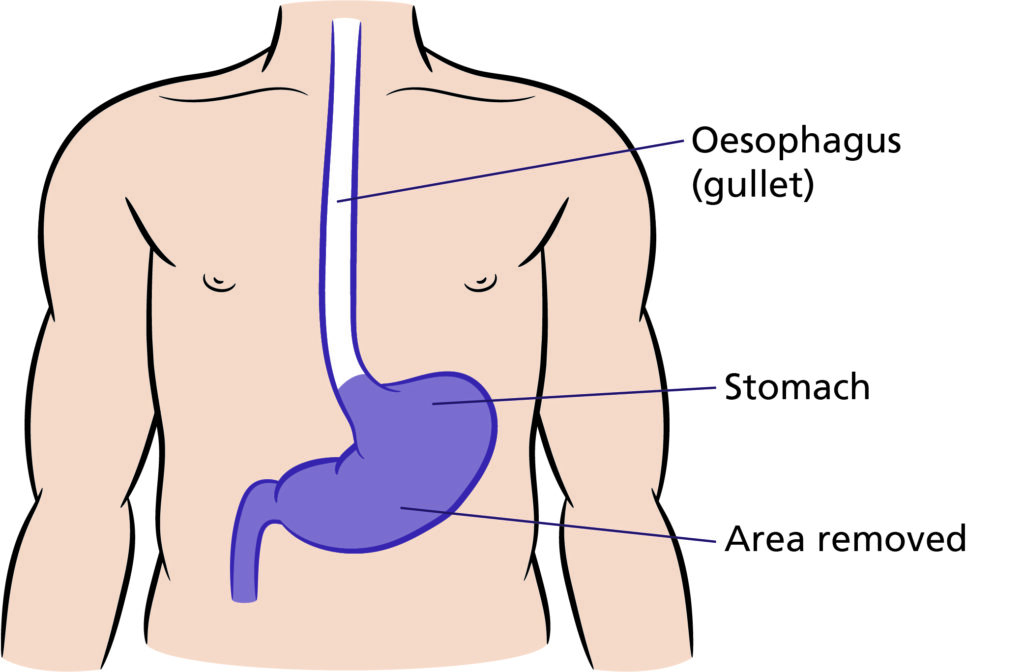
Illustration that shows the area to be removed for full gastrectomy which is the entire stomach (Shaded in purple).
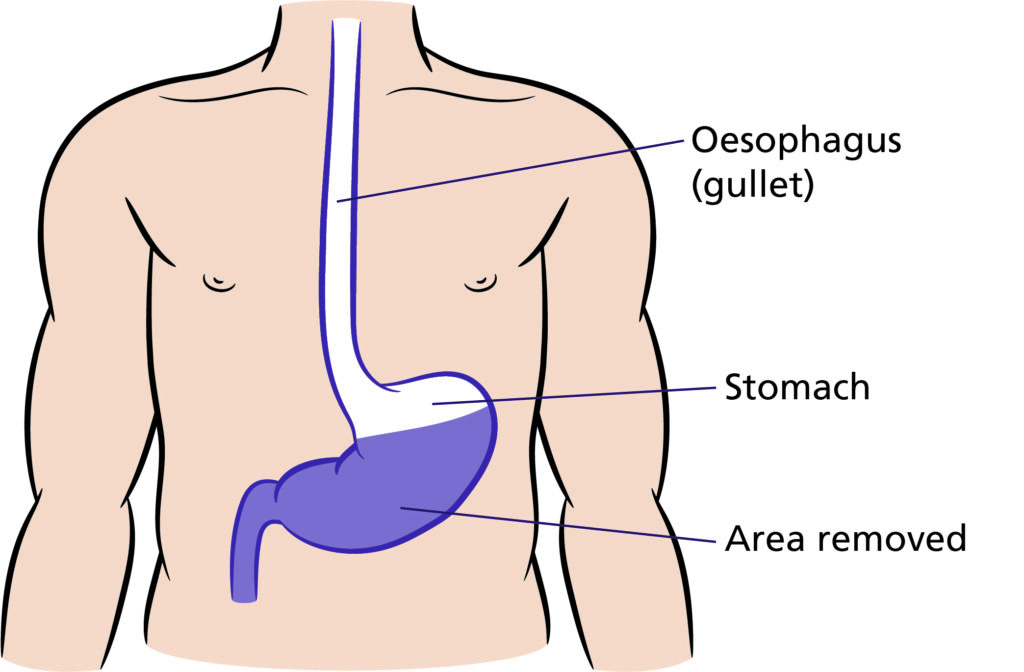
Illustration that shows the area removed for partial gastrectomy which is partial stomach (Shaded in purple)
How long will I be in hospital?
You should expect to remain in hospital for 1 – 2 weeks after the operation. Rates of recovery from this surgery vary from person-to-person and are dependent upon several factors.
Up to half the people undergoing this operation can develop a ‘complication’, some of which may prolong their stay in hospital.
These ‘complications’ vary in their severity. Your risk of developing them will be explained to you in more detail by your surgeon and nursing team.
Briefly, they can include:
- bleeding problems. You may require a blood transfusion;
- chest Infections and other respiratory (lung) problems;
- wound infections;
- anastomotic leak (delayed healing of the new ‘join’ between oesophagus and bowel);
- heart problems; and
- Deep Vein Thrombosis (blood clot developing in the veins in the leg).
As with all major surgery there is a small risk to life.
Preparing for your operation
Before your operation, it is important that you stay as fit and well as you can. Taking regular, gentle exercise and eating well is very important. If this is difficult for you, please ask for advice.
If you smoke, you should stop at the earliest opportunity. Stopping smoking, even just a few weeks before your operation will make a big difference to your ability to recover from the surgery and reduce your risk of developing complications.
Pre-admission visit
You may have already undergone a series of tests to check your fitness for surgery. You will need to attend the hospital again before your operation to complete further tests. This is known as pre-assessment.
Being admitted to hospital
You may be asked to stay in the hospital hotel on the night before surgery. Alternatively, it may be appropriate for you to be admitted on the day of surgery.
The arrangements will be discussed with you during your outpatient appointment by your surgeon. You will be asked to sign a consent form. This is proof of your understanding and agreement to undergo the operation.
An anaesthetist will usually visit you before your operation. He / she is the doctor who will put you to sleep for your operation. You will commence daily injections to help prevent you developing blood clots in your legs.
Usually, it is only necessary to stop eating and drinking six hours before surgery.
Your nurse will give you a gown to put on and some stockings to wear. The stockings help prevent blood clots in your legs (Deep Vein Thrombosis).
A porter will come to the ward with a trolley to take you to the operating theatre. Your ward nurse will go with you and will usually stay with you until you are asleep.
What to expect after your operation
The operation usually takes between 3 – 5 hours and with time in the anaesthetic room before the operation, and time in the ‘recovery room’ after the operation. You are likely to be off the ward for at least 4 – 6 hours.
You are likely to return from theatre to the High Dependency Unit (HDU). This is a similar area to the wards but has more nursing staff and the equipment needed to monitor your condition more carefully. The High Dependency Unit (HDU) is on Ward 81, Level 2, Bexley Wing, St. James’s University Hospital.
You will usually stay on the HDU for between 1 – 4 days. Occasionally, patients may be nursed on the Intensive Care Unit (ICU), for the first 24 – 48 hours if more careful monitoring is required.
On arrival to the HDU, you will be awake and able to talk but will also probably be quite sleepy. You will be attached to various tubes and monitors, your nurses will help explain these to you.
Oxygen therapy
You will wake up from your operation with an oxygen mask on. This fits over your nose and mouth and ensures that you receive sufficient oxygen to help you to recover from the anaesthetic. Your nurse or physiotherapist will inform you how long you need to use it.
Intravenous fluids (drip)
These are used during the period when you are ‘nil by mouth’ or taking restricted fluids by mouth. They prevent you from becoming dehydrated and will be removed when you are drinking normally. They are usually given by a thin tube that is placed in the vein at the side of your neck (central line). Medications can also be given via your drip such as antibiotics.
Catheter
During your operation, a catheter will be inserted. This is a tube which drains your urine into a bag enabling us to make accurate measurements. Having a catheter means that you will not need to get out of bed to pass urine. It will usually stay in place for 4 or 5 days.
Naso-gastric tube
This is a thin plastic tube which enters via a nostril, down the back of your throat and into your stomach or bowel. It enables the nurses to empty the contents of your stomach. This helps to relieve sickness and also aids the area of the operation to heal. It usually only stays in for a few days.
Abdominal drain
This is a thin plastic tube that is inserted through your abdominal (tummy) wall. It helps you to heal by draining fluid away from the area of the operation.
Epidural
This is a very fine tube inserted through your back for pain relief. Through this tube, we are able to give a local anaesthetic that will numb the nerves around the tummy. You will not be aware that this tube is in position other than feeling lots of sticking plaster securing it in place on your back. Epidurals are usually inserted in the anaesthetic room before your operation and stay in place for 4 – 7 days.
PCAS – Patient Controlled Analgesia System
This is a system of giving a strong painkiller through your drip.You may be given a handset with a button on it which when pressed will give a set dose of the painkiller. Your nurses will advise you on how best to use it. It has a safety ‘lock-out’ system which means you can press it often without risk of overdose. Some surgeons use a wound irrigator that delivers pain relief directly to the wound.
Wound (cut down the abdomen)
Your wound is initially covered by a dressing. Your nurses will inspect the dressing regularly. Your dressing will be removed on the 2nd day after your operation and will only be replaced if there are signs of leakage. You may have clips (small metal staples) holding the edge of the wound together. These are removed by the nurses 10 – 14 days after your operation.
Your nurses will continue to examine your wound, checking for signs of healing (you should inform your nurse if you notice any redness, leakage, heat or increased pain around your wound as this may indicate a wound infection).
Keyhole surgery
Some surgeons use a keyhole approach to assist surgery. The operation is exactly the same as with the open approach but on the surface, the abdomen may have five tiny cuts rather than the long traditional cut.
Recording observations
Initially, your nurses will record your pulse, blood pressure and temperature regularly. These recordings help your doctors and nurses to monitor your condition.
Personal care
After your operation, you will need to rely on your nurses to help you with washing, bathing and changing your clothes. When you start to feel stronger and have fewer attachments (drips, catheter etc), you will be encouraged to participate in your care more. If you have any special needs or are worried about this aspect of your care, please speak to one of your nurses.
Eating and drinking
You will not be allowed to eat or drink for approximately 4 – 5 days after your operation. This is to ensure that the join inside is allowed to heal.
The nurses will help you to brush your teeth and tongue, and use mouthwashes regularly to prevent your mouth and lips from becoming dry and sore. Your ‘drip’ will prevent you from becoming dehydrated.
If you have had all your stomach removed, you may need to go the X-ray department to have a ‘contrast swallow’ approximately 5 days after your operation. This test involves drinking a special ‘dye’ while standing in front of an x-ray machine. The pictures taken enable the doctors to check that the new join inside has healed (NB: this ‘dye’ can give you diarrhoea an hour or two after the test).
After the doctors have confirmed that the join inside has healed, you will be allowed to start drinking sips of water. The amount you are allowed to drink will increase daily until you are eating a ‘light diet’.
In a small number of patients (up to 10%), the x-ray pictures show that the new join inside has not healed after 1 week. This is called an ‘anastomotic leak’. If this happens, your doctors will advise you further.
Helping your recovery
Before your operation, a nurse will explain to you some things that you can do to aid your recovery and to prevent problems after your operation.
Smoking
You should stop smoking at the earliest opportunity before your operation. This helps to prevent you getting a chest infection after your operation. Chest infections are one of the most common and most serious complications following this surgery.
Deep breathing exercises / coughing
The nurses and physiotherapists will show you how to breathe deeply to expand your lungs fully and how to cough, supporting your wound. Doing this regularly after your operation will aid your recovery and help lower the risk of developing a chest infection.
Leg exercises and mobility
After your operation, it is important that you regularly perform gentle leg exercises whilst in bed. Your nurse will show you how to do these and will help you to regularly change position in bed. These actions help prevent you developing ‘pressure sores’ and clots in the legs (Deep Vein Thrombosis).
After ensuring that you are pain-free, your nurses will help you get out of bed and have a short walk within the first few days after your operation. This will increase over the following days. Although you may not feel like getting out of bed after your operation; remember, walking helps your lungs expand and so helps to prevent chest infections. It helps the blood to circulate preventing clots and also helps to prevent you becoming sore or stiff from lying in bed.
Pain control
It is our aim for you to be as pain-free as possible after your operation. It is important that you tell your nurses if you have any pain so that we can give you pain relief. It is also important to tell your nurses if your painkillers are not working so that we can try an alternative method.
There are various methods we can use to control your pain (epidural, PCAS, injections, suppositories, finding a comfortable position etc.). Your nurses will explain these in more detail.
Remember, it is important that you tell your nurses if you have pain. If your pain is well controlled, you will feel more able to deep breathe, cough and mobilise; therefore, aiding your recovery.
Going home
It is important that your nurses, together with you and your family, make plans as early as possible for your discharge home. This helps to ensure that you do not have to stay in hospital longer than necessary.
Thinking about going home can be quite an anxious time. It is likely that you and your family will have concerns about how you will manage and what to do if problems arise.
Please discuss any concerns you have with your doctors and nurses. They will be able to offer help and advice.
Tiredness
By the time you are ready to go home, you will be able to walk around and get yourself washed and dressed; however, you will tire easily. Recovery from this operation is not fast and it may be a few months before you feel back to your normal self. During this time you will gradually begin to feel stronger, although it is common to have ‘off days’ along the way.
Getting plenty of rest in the early days of being at home is important. Having an afternoon nap for the first couple of weeks is recommended and will prevent you from becoming overtired.
It is important to gently increase your level of activity over the following weeks and months as you feel able. Taking a short walk each day, increasing the distance gradually, will have positive benefits.
Eating
By the time you are ready for home, you will be eating a sloppy / soft diet following your operation. Starting to eat soft foods can feel strange at first, you are likely to feel full very quickly and have loss of appetite.
A dietician will visit you on the ward before you go home to advise you on how to overcome some of these problems.
Eat ‘little and often’. As you will feel full quickly, it is important to eat several small meals and snacks throughout the day rather than rely on three meals per day.
To help with loss of appetite, concentrate on eating the foods and snacks you enjoy. You should not need to avoid any particular food, although you may be advised to stick to soft /sloppy food initially.
Most patients will lose weight in the first few weeks following surgery and few patients return to the weight they were before their operation. As your appetite improves and if you concentrate on eating ‘little and often’, this weight loss should stop.
Pain
You may continue to feel ‘tender’ around your wound for some time after you go home. You will be given painkillers to take home to have as needed. Further supplies can be obtained from your GP. The nerves around your wound take some time to heal and you may notice that parts of your wound remain numb for some months.
Dumping syndrome
This is the name given to a variety of symptoms that some patients may experience, following a gastrectomy. With all or much of the stomach gone, food and fluids can pass too quickly into the small intestine causing symptoms including:
- cramping;
- diarrhoea;
- dizziness;
- nausea and vomiting;
- shortness of breath; and
- sweating.
Dumping syndrome may resolve on its own after a few months and is often relieved by dietary changes. If these symptoms persist, you should speak to your doctor or nurse specialist who will be able to advise you.
Vitamin B12 is an essential substance that the stomach usually processes. After gastrectomy, it will be necessary to have an injection to replace this every 3 months. Your GP should arrange this for you.
Returning to normal
It is understandable to want to know when things will start to feel normal again, following your operation. You may want to know when you can resume work, go on holiday or begin driving again. Although we know that recovery from this surgery takes a few months, the rate of recovery varies from person-to-person and it is difficult to predict how long this will take in your case. If you are concerned about your rate of recovery, please speak to your doctor or nurse specialist.
Follow-up
Following your operation, you will return regularly for
check-ups at the hospital. Your 1st clinic appointment will be within 4 – 6 weeks after going home and will give you the opportunity to discuss any problems or worries that you have.
In the meantime if you want advice, information or support, you can contact the nurse specialists (Monday to Friday, 8.00 am – 5.00 pm).
Out of normal working hours advice can be obtained from the ward on which you stayed, following your operation. For more urgent help or medical care, you are advised to contact your GP or local Emergency Department.