Welcome to the Dialysis Unit
Welcome to the Haemodialysis Service. Dialysis treatments vary, however the majority of
patients attend for treatment three times a week.
All units are open Monday to Saturday with the exception of Ward J48 which runs 24 hours, 7 days a week.
Appointment times are:
- Morning
- Afternoon
- Early Evening Shift
- Twilight – 7pm (Ward J48 at St James’s only)
- Night – Midnight (Ward J48 at St James’s only)
Each dialysis treatment takes four hours although this can sometimes be longer or shorter. You will be allocated an appointment time – on the same day and at the same time each week. However, this may need to be altered in order to accommodate new patients who also require lifesaving treatment.
We have a number of dialysis units across the region; these are:
- Ward J48 Dialysis Unit – 1st Floor, Lincoln Wing, St James’s Hospital, Leeds, LS9 7TF.
- Beeston Dialysis Unit – James Reed House, Beeston Village Medical Centre, Town Street, Beeston, LS11 8PN.
- Dewsbury Dialysis Unit – Staincliffe Wing, Dewsbury District Hospital, WF13 4HS.
- Halifax Dialysis Unit – Calderdale Royal Hospital, Salterhebble, Halifax, HX3 0TW.
- Huddersfield Dialysis Unit – Acre Street, Lindley,
Huddersfield, HD3 3EA - Pontefract Dialysis Unit – Friarwood Lane, Pontefract, WF8 1PL.
- Seacroft Units – R&S Ward/B Ward – Seacroft Hospital, Leeds, LS14 6UH.
Despite receiving dialysis at one of these units your care will remain the responsibility of Leeds Teaching Hospitals and their Consultants.
There may be a need to change where you have your treatment and/or your appointment times. We will discuss this with you if the need should arise.
Back to topWhat to expect
When you arrive at the dialysis unit for your appointment time, you will be asked to wait
in the waiting area. The nursing staff will call you when your dialysis station is ready.
Please be patient, there may be a wait, as staff need time to make sure all areas are thoroughly cleaned and prepared for you.
We are keen to support ‘Shared Care’ on the dialysis unit. This means we support patients to participate and learn any aspect of the dialysis preparation and/or therapy.
- Before treatment you will need to be weighed and have your blood pressure and pulse taken. Your hands will need to be washed.
- Your fistula or graft will need to be washed and dried before being settled on your dialysis chair or bed.
- It is advisable to wear comfortable, loose fitting clothing when you attend for treatment.
- Please bring with you any medication you may need, particularly your phosphate binders, as you will be offered a light snack during your treatment.
While you are with us some of the people you may see will include:
- Renal consultant
- Renal nursing staff
- Renal matron
- Specialist renal dieticians
- Advanced clinical practitioners
- Research nurses
- Yorkshire Ambulance Service staff
Kidneys – How do they work, what do they do?
Most people have two kidneys, bean shaped organs about 12 centimetres long, 6cm wide and 3cm thick.
Each kidney weighs about 150grams and lie deep inside the body and sit under the lower ribs at the back.
The left kidney is located slightly higher than the right kidney due to the larger size of the liver on the right side of the body.
Normal healthy kidneys:
- Clean waste products from the blood
- Remove excess fluid
- Help to control blood pressure
- Help to make red blood cells
- Produce vitamin D for healthy strong bones

Haemodialysis
Haemodialysis treatment involves the blood being cleaned or filtered using a haemodialysis machine.
Haemodialysis is usually undertaken three times per week and takes approximately four hours on each occasion. Dialysis slots are Monday, Wednesday and Fridays or Tuesday, Thursday and Saturday.
Some patients have haemodialysis in their own homes. If you would like to explore this treatment option please mention this to the staff on the unit who can arrange for you to meet the Home Haemodialysis Team.
Haemodialysis is usually commenced gradually over three sessions and a treatment programme will be prescribed to your individual needs.
You will be allocated an appointment time – on the same day and at the same time each week. However this may need to be altered to accommodate new patients who also require lifesaving treatment.
Back to topVascular access
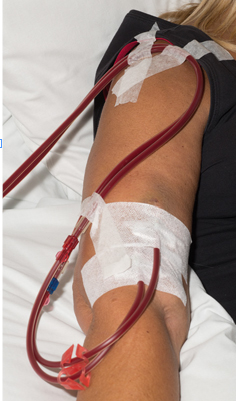
Haemodialysis requires access to the blood system; we refer to this as the vascular access. There are three different options for this: a fistula (preferred first choice), a graft or a dialysis line.
Fistula

A fistula is formed during an operation. During the operation the surgeons join a
vein and an artery together; this is usually in the lower or upper arm. This increases the
blood flow into the vein which enlarges the vein enough to make it suitable for the insertion of dialysis needles. This operation is not always possible for every patient and an alternative procedure of a graft may be offered.
How will I get a fistula?
An appointment will be made for you to have an ultrasound scan of the veins in your arms. Following this you will receive further information from the specialist team to discuss the options available to create a fistula. Depending on where the fistula will be, it may be created under a local anaesthetic or nerve block (which numbs the whole arm) and you would be discharged the same day. Alternatively you may require a general anaesthetic which may require you to stay overnight. Your fistula will be monitored at outpatient appointments to assess how it has developed and further ultrasounds may be required.
Benefits of having a fistula
A fistula is the best possible form of access for haemodialysis and provides the safest, most efficient way to receive regular treatment. However if a problem does occur you need to report this to the dialysis staff, so that they can act quickly.
Risks of having a fistula include:
- Clotting – Occasionally fistulas can clot. If you cannot feel the usual ‘buzzing’ over the fistula or if it weakens contact the dialysis staff. Clots can be removed by surgery or by other procedures where clots can be dissolved.
- Bruising or swelling – This often occurs when the fistula is new and is due to the needle piercing the fistula or graft wall allowing blood to leak into the tissue. All bruising and swelling should be reported to the dialysis staff.
- Allergies – If your fistula becomes red, itchy or sore it may be due to the application of creams, cleaning products or dressings, let your nurse know.
- Aneurysm – This is a swollen area that can occur over time due to the needles being put in the same area. If the skin becomes thin or shiny or you can see a pulse under the skin or swollen area appears suddenly, please tell the dialysis staff.
- Steal Syndrome – This can occur if your hand is not receiving a good enough blood supply. When a fistula is created some of the blood supply is diverted or ‘stolen’ by the fistula. Let the dialysis staff know if you experience pain, coldness or tingling in the fingers or hand on your fistula arm.
- Redness or heat – Sometimes together with swelling and pain, can be signs of infection. Please contact the dialysis unit immediately.
- Narrowing of the fistula – Narrowing of a fistula can result in poor flows when you are on the dialysis machine, bleeding post dialysis or swelling of the arm and hand. This condition may require a procedure called fistulaplasty to open or widen the narrowing. If this is something that is required you will have further discussion with your team.
- Scab – If a scab over your needle site does not heal quickly or gets larger let the dialysis staff know as this can lead to a risk of bleeding.
- Bleeding – The flow of blood through the fistula is much stronger than through ‘normal’ veins which can increase the risk of bleeding:
- Bleeding during dialysis – If blood starts to ooze around your needles during dialysis or it takes longer to stop bleeding at the end of treatment tell the dialysis staff immediately.
- Bleeding at home – Occasionally a fistula may start to bleed at home, if this happens it should stop quickly when firm pressure is applied. However, although this is a very rare occurrence, you should know what to do if profuse bleeding occurs from your fistula or graft site unexpectedly between dialysis sessions.
This is a medical emergency
Apply firm pressure at the bleeding point. Use gauze or two fingers. Do not use a large dressing like a towel as this may stop you applying enough pressure in the right place.

Get help from anyone that is around, the blood flow can be fast and make you feel faint so DO NOT delay in alerting others.
Ring ‘999’ for paramedic assistance
Where will my fistula be?
Preferably your fistula will be formed in your non-dominant arm unless this is unsuitable. The surgeon will discuss with you the most appropriate site after assessments of both arms have been made.
What to expect after the fistula operation?
On returning to the ward, the nursing team will check your temperature, pulse and blood pressure as well as regular checking of the fistula itself. This will involve listening to the ‘bruit’ which is a whooshing sound heard through a stethoscope around the fistula. The presence of a bruit is an indicator that there is a good blood flow through the fistula. On touching the fistula you may feel a buzzing sensation. The nursing staff will show you how to feel for this sensation and check your fistula.
Initially there may be some bruising but this should resolve within a couple of weeks. You may feel some discomfort and you can have pain relief for this, inform the nursing staff if you do have pain or discomfort.
After Discharge
There will be a small sterile dressing over the incision site which can be removed after 48 hours after your operation and kept clean and dry. You can shower after 48 hours providing you carefully pat the wound dry.
Important Points

- You need to check the thrill/bruit of the fistula every four hours initially, by placing your first two fingers gently over the wound site or just above. You will need to check your fistula at least once a day. Please contact your dialysis unit immediately if your hand becomes excessively swollen or becomes painful, if the appearance changes or you cannot feel the usual thrill.
- Avoid any pressure on your arm or wrist as this may cause the thrill/bruit to stop or a clot to form inside. This includes tight fitting clothing or jewellery, shopping bags looped over your arm.
- Avoid any heavy lifting for the first two weeks to allow healing to take place.
- Avoid sleeping on your fistula arm.
- Do not let anyone use this arm for taking blood samples or checking blood pressure.
Skin Care
The frequent use of antiseptic skin cleansers and tapes used at dialysis can lead to a disruption in the normal barrier function of the skin. As a result skin can become itchy, sore, red and flaky which can increase the risk of developing a skin infection.
We recommend that you apply a non-perfumed moisturiser to the skin on your fistula arm each day.
Always wash your hands before touching your fistula and make sure staff do the same. The arm should be washed with soap and water when attending for dialysis.
Graft
A graft is an artificial tube inserted during an operation, one end is attached to an artery and the other end attached to a vein. Again this will usually be in the upper or lower arm, sometimes in the thigh.
How will I get a graft?
A graft operation will always require a general anaesthetic and an overnight stay. Grafts can sometimes be used immediately or within a couple of weeks.
Dialysis Line
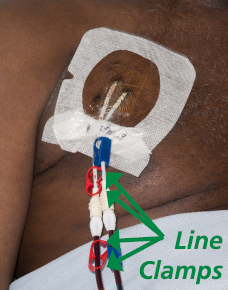
A dialysis line is a flexible tube, which is put into one of the large veins in the neck and held securely in place by a cuff under the skin or by two stitches.

As soon as the line has been inserted, it can be used for haemodialysis.
The line is divided into two ‘lumens’. During dialysis, blood flows to the machine through one lumen and back into your body through the other lumen. Your line provides a way for the dialysis machine to clean your blood. The point where the tubing enters the skin is called an ‘exit site’. Lines can be temporary or more long term.
Risks of having a line include:
- Infection – The nursing staff will check your line and the exit site at each dialysis session for any signs of infection. You must contact your dialysis unit immediately if you notice:
- The skin around your dialysis line is sore, red or has a discharge
- You have fevers or chills
- You are generally unwell
- There is pain or swelling around the line site
These symptoms could indicate that you have a serious infection and it must be treated urgently as you may need intravenous antibiotics.
- Bleeding – If there is bleeding from or around the tube apply pressure to the exit site, and contact the renal unit for advice. If you are unable to control the bleeding please call 999.
- Clamp fallen off/hole or tear in line – Apply firm pressure above where the clamp has fallen off or the hole/ tear to prevent air from entering the blood stream , call 999 and lie down on your left side with your feet up and head down until help arrives. This is to help prevent any air in your blood stream from causing any damage.
- Cap Dislodgement – If the caps should come off ensure the clamps on the line are closed. Cover the end of the line with a sterile gauze and cling film or plastic bag and contact the dialysis unit immediately.
- Line movement – If the length of line appears longer than normal do not attempt to push it back in. Occasionally lines can be pulled out or fall out especially in the days following insertion before the line has been secured to your skin.
In the event of a line falling out, apply firm pressure (preferably sterile gauze) and call 999.
Important Points
- Your dialysis line may contain heparin (a blood thinning drug). It is important that you (or a relative) inform any healthcare staff that may need to access this line in an emergency. Any heparin in the line needs to be removed before this can be done. Your line should not be used for any other purpose than dialysis or in the event of an emergency, alternative access must be used.
- Avoid touching your line or the area around it. Line dressings are usually changed weekly, unless they are soiled or the site looks infected. Only change the dressing at home if absolutely essential and if you have been trained to perform this task.
- Avoid getting your line and dressing wet as this can increase the risk of developing an infection. The dressing must be covered for showering or bathing. Nursing staff on your unit can advise you on how to do this.
- Avoid pulling the line or catching your line on clothing when dressing or undressing. You can wear a vest or a cropped bra under your clothes to help keep your line close to your chest. If you need a securing device to stop the line moving, discuss with the nursing staff.
- Ensure that the clamps and caps remain closed at all times when your dialysis line is not being used for dialysis. These prevent air and germs from entering the blood stream. Do not let people other than your dialysis team handle or touch the line (especially young children/babies or pets).
Shared Care in Haemodialysis

At Leeds Kidney Unit we are committed to delivering the highest quality of dialysis care and promote Shared Haemodialysis Care.
Shared Haemodialysis Care means working with you in partnership to be more actively engaged in your treatment. The idea is that shared care gives you the opportunity and encourages you to learn more and participate in any aspect of your dialysis care. You will gain a greater understanding of your condition and treatment, gain greater confidence and have more control of your dialysis.
You will be supported and educated to be as involved as you choose, to a level you would feel safe and comfortable with, choosing which aspects you want to be more involved with.
There are many ways in which patients can engage in their own dialysis care from learning about their condition and how haemodialysis works to participating in any of the tasks involved such as:

Patient experience
Patients involved with Shared Care tell us that they enjoy being involved and that it helps them to understand and feel in control of their condition:
One of the down sides of being on dialysis is that you feel you have lost control of your life. Taking part in Shared Care has given me back some control, a feeling of self- esteem and achievement and a better understanding of my care.
For more information visit: www.shareddialysis-care.org.uk/
Back to topAttending for dialysis
Like healthy kidneys, the dialysis treatments clean the waste products and excess water to prevent them from building up in the body. It keeps a safe level of certain chemicals in your blood, such as potassium, sodium and bicarbonate from your blood.
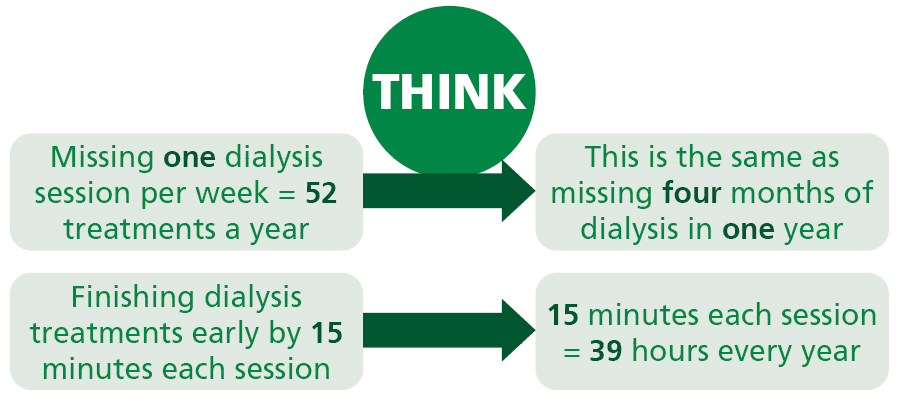
You need to know that missing dialysis or coming off treatment early has risks and can lead to complications which can put additional stress on your body. Symptoms you may experience if you’re not having enough dialysis include:
- Shortness of breath – build of fluid in the lungs.
- Cramp and low blood pressure – as a result of removing more fluid at the next session.
- Heart problems – such as irregular heartbeat, cardiac arrest and death due to high potassium levels and excess fluid that has built up.
- Weakness and lethargy – as a result of worsening anaemia due to not having iron and aranesp medications.
- Loss of body/flesh weight.
- Poor appetite/ a taste of ammonia in the mouth.
- Nausea.
Missing dialysis may result in you not being fit enough to have kidney transplant surgery if you are on the list. Your life depends upon you receiving the right amount of dialysis treatment, the doctors and nurses and other members of the team will encourage you to attend for all your treatments and to remain on dialysis for the amount of time you have been prescribed. If you are having difficulties in attending for your treatment please speak to a member of staff.
Patient Knows Best
Patient Knows Best allows patients in certain specialities and locations to look up test results and info about their disease and its treatment, both online and via mobile. It began as a renal (kidney) project, and now covers 90% of UK renal units. All you need is access to the internet via a computer terminal.
Patient Knows Best shows your latest test results. Set up alerts, monitor symptoms and download your records. You can view Patient Knows Best from anywhere you want and share your information with anyone you want. For more information go to www.patientsknowbest.com/renal or ask the nursing staff.
You will have bloods taken whilst on dialysis every month which are then looked at in monthly meetings by the doctors, nurses and dieticians.
The information below will help you to interpret your routine blood test results. The ‘normally preferred’ range is a guide but for more information ask the doctors or nurses on the unit.
Back to topBlood tests and what they mean
For more information on your blood test results please ask the nursing staff or doctors at your unit.
Back to topCarbapenemase-producing enterobacteriaceae (CPE) screening
What is CPE?
CPE is short for carbapenemase-producing Enterobacteriaceae. Enterobacteriaceae are bacteria that usually live harmlessly in the gut of humans. This is called colonisation (a person is said to be a carrier). However, if the bacteria get into the wrong place, such as the bladder or bloodstream they can cause infection.
Carbapenems are one of the most powerful types of antibiotics which are used to treat some types of infection. Carbapenemases are enzymes (chemicals), made by some strains of these Enterobacteriaceae bacteria, which allow them to destroy carbapenem antibiotics and so the bacteria are said to be resistant to the antibiotics. This means that the Carbapenem antibiotics would not be effective in treating infections caused by CPE.
Why does carbapenem resistance matter?
Carbapenem antibiotics can only be given in hospital directly into the bloodstream. Until now, doctors have relied on carbapenem antibiotics to successfully treat certain difficult infections when other antibiotics have failed to do so. In a hospital, where there are many vulnerable patients, spread of resistant bacteria can cause problems, so we want to take action to minimise the risk of these bacteria being spread between patients.
Do people who are carriers of CPE require any treatment?
If a person is a carrier of CPE, they do not need any treatment. However, if the bacteria have caused an infection then other types of antibiotics will be required.
How will I know if I am at risk of being a carrier or having an infection?
There is an increased chance of picking up these bacteria if you have been a patient receiving treatment in a hospital or haemodialysis unit abroad or in a UK hospital or haemodialysis unit that has had patients carrying the bacteria, or if you have been in contact with a carrier elsewhere. If any of these apply to you, screening will be arranged for you and you will be accommodated in a single room where ever possible at least until the results are known.
Why do I need to be screened for CPE?
If you are going away to receive haemodialysis or other medical treatment in another medical centre either in the UK or abroad they may ask for you to be screened for CPE prior to your visit and you will be rescreened on your return.
What does screening involve?
Screening usually involves taking a rectal swab (a sample taken by inserting a swab briefly just inside your rectum (back passage) because CPE live in the gut). Three swabs are required and will be usually be taken on three consecutive dialysis treatments. We will normally be able to give you the results within seven days.
What will happen if my screening results show that I am a carrier for CPE?
If you are a carrier of CPE, you will usually be placed in a single room if you are admitted to hospital, and also when you attend for your haemodialysis treatment. Hospital patients with a weakened immune system (such as renal patients), or those who have had an operation or who have
undergone another invasive procedure are at a greater risk of developing an infection caused by CPE. We may need to make special arrangements for your care, for example, in scheduling planned procedures.
It is important for us to know if you are carrying CPE because if you develop an infection, we can choose the right antibiotic straight away to treat you appropriately.
How did I get CPE?
It can be difficult to say when or where you picked it up. However, there is an increased chance of picking up these bacteria if you have been a patient in a hospital abroad or in a UK hospital that has had patients carrying the bacteria, or if you have been in contact with a carrier elsewhere.
How is the spread of CPE being controlled?
We can reduce the number of patients affected by CPE by following simple prevention and control measures:
- Thorough hand hygiene before contact with every patient.
- Screening to identify patients who are carriers of CPE.
- Using single rooms for patients infected with or carriers of CPE. If no single rooms are available, you may be cared for in an area where you are with other patients who also have CPE.
- Ensuring healthcare workers use contact precautions (personal protective. equipment PPE) when caring for patients who are infected with or carriers of CPE.
- Effective cleaning and disinfection of surfaces and equipment that may be contaminated with CPE.
The most important measure for you to take is to wash your hands regularly, especially after using the toilet and before eating food. Avoid touching any areas of broken skin, wound dressings, and your dialysis line, particularly at the point where it is inserted into your body or skin and maintain good general hygiene.
As CPE does not usually cause infections in healthy people, your family/friends are at a low risk of CPE infection. However, visitors to dialysis units should wash their hands before and after touching you or your immediate environment.
What about the future
You should carry on as normal, maintaining good hand hygiene using soap and warm running water. You should wash your hands before preparing food or eating and directly after using the toilet.
Good personal hygiene is important; this will help protect you from infection and reduce the risk of spread to others
Here in Leeds where ever possible, you will be accommodated in a side room if you are found to be CPE positive.
Further information
Please speak to your doctor or nurse if you have any questions or concerns about CPE or other aspects of your treatment. For general infection prevention and control information, please contact the hospital’s infection prevention and control team on 0113 392 2691.
Back to topCOVID-19 (Coronavirus) information
Haemodialysis Services
Due to the Coronavirus pandemic we have to adjust our services and look at new ways of
working. Our main objective is to deliver a service that continues to meet the needs of our patients whilst keeping you and staff as safe as possible.
To help with this if you are due to attend any treatment sessions please contact the staff at your dialysis unit before your appointment if you or someone in your household have a:
- high temperature
- new, continuous cough
- loss or change to your sense of smell or taste
Do not enter/attend your dialysis unit.
The staff at your dialysis unit will give you instructions on what you will need to do. This may include arrangements to attend the dialysis unit at St James’s Hospital as you will still require your dialysis treatment.
Additional advice can be found on the NHS website:
www.nhs.uk/coronavirus
Medications
As a person with kidney problems you may have to take a large number of medications
each day which will be prescribed by your doctor.
When buying ‘over the counter’ medications, please let the pharmacist know that you are a kidney patient.
Common drugs used in kidney disease
- Blood Pressure Controlling Medications – people with failing kidneys may have high blood pressure because the kidneys are not working properly. It is important to control blood pressure to avoid further damage to the kidneys and also cardiovascular disease (heart attacks and strokes). Some of the common blood pressure tablets include:
- Beta-blockers (atenolol, bisoprolol etc)
- Calcium channel blockers (amlodipine, diltiazem etc)
- Alpha-Blockers (doxazosin)
- Ace-inhibitors (lisionpril, ramipril, perindopril etc)
- Angiotensin Receptor Blockers (losartan, candesartan etc)
- Diuretics – If kidneys cannot get rid of excess fluid in the urine, it can be helped by water tablets called diuretics, most common Furosemide. Patients on dialysis may also benefit from them.
- Sodium bicarbonate – The kidneys are involved in keeping the acid levels in your body within a specific range. In kidney failure this does not happen as well and tablets of Sodium Bicarbonate can help manage this.
- Phosphate binders – Phosphate is a chemical found in everyone’s blood but with kidney failure the levels can rise. Most patients will need to take phosphate binders to ‘mop up’ phosphate before it is absorbed from the stomach. It is important to take these just before eating, with the meal or immediately afterwards.
- Vitamin D – Kidneys are involved in making Vitamin D into a form the body can use. Without this patients can suffer from low levels of calcium in the blood and bone disorders similar to osteoporosis. Patients may need to take Alfacalcidol or Calcitriol which are active forms of Vitamin D.
- Erythropoietin – Kidneys are involved in the making of red blood cells by releasing Erythropoietin (EPO). In kidney failure this no longer happens and patients often suffer with anaemia. This is usually treated by injecting EPO on dialysis.
- Iron – Many patients will need iron supplements such as Ferrous Sulphate. In some patients including haemodialysis patients, it may be necessary to ‘top up’ iron levels with an infusion of iron.
Whilst you are on dialysis you will be seen by the renal pharmacist who will support you with any queries you may have your medications.
Nurses and doctors can also help with any queries you may have.
This is not an exhaustive list of medications used.
Back to topDietary information and guidance
Diet and fluids are an important part of your dialysis treatment.
When kidneys are not functioning properly, fluid and waste products will build up from the food and drink you have.
The haemodialysis machine will clean the blood of this waste and excess fluid but they are not as effective as normally functioning kidneys so you will need to make changes to your diet and fluid intake.
Specialist dieticians will review your blood test results and provide you with guidance and advice on eating the right foods to help limit the build-up of these waste products. This guidance is very specific to your own individual needs and will depend on your current dietary intake and urine output. It is important not to take dietary advice from other sources as this may not be right for you.
Salt Intake
Having too much salt in your diet can cause an increase in thirst, high blood pressure and a build-up of fluid.
Simple steps such as not adding salt at the table or in cooking will help, but the most important way to reduce your salt intake is by avoiding tinned and highly processed foods as the manufacturers of these products often add very large amounts of salt.
Potassium
Not everybody on dialysis needs to follow a low potassium diet. The aim is to keep your potassium between 4-6.5mmol/L before dialysis. If your potassium level is high the dieticians will advise you on what you can do to help reduce this by altering your diet, avoid foods that are high in potassium.
Protein
Patients on haemodialysis require more protein, to meet the basic needs and replace what is lost through dialysis. The dietician will advise you how much protein you need and how to achieve this from your diet. Your urea levels give an indication of how much protein you have eaten.
Fluid Balance
When you first start dialysis, it is important that you inform the nursing staff on the unit if you notice a significant change in how much urine you pass.
You may still be passing urine but over time your urine output will usually reduce. When you drink more than you are passing, the excess fluid will build up in your body causing ‘fluid overload’. This increase in fluid on your body will cause an increase in your blood volume so that your heart has to work harder. Excess fluid can cause swelling around your body, such as your legs, and, in extreme cases, it can settle in your lungs making it harder to breathe.
During dialysis, it is important that the excess fluid is removed and you achieve the target weight in order to reduce the risks of the above symptoms. Your target weight is your weight (bone, skin, fat etc.) without any excess fluid in your body. The dialysis machine can only remove a certain amount of fluid in one dialysis session and some people can only tolerate small amounts so it is really important to manage both your fluid and salt intake as you have been advised.
Back to topWhat can you do?
- If you are diabetic, maintain good control of your blood sugar levels.
- Eat a healthy, low salt diet. The dietician will give advice on your dietary intake.
- Maintain a healthy lifestyle, exercise regularly, stop smoking and drink only in moderation. You may have been advised to restrict your fluid intake.
- Have a yearly flu and COVID jab at your GP practice.
- Have a course of Hepatitis B vaccinations – ask your dialysis team.
Dialysis away from base
Holidays are important to most people and we hope to do everything that we can to help
make this possible and the process smooth so that you can enjoy your break away from your home life and daily commitments. It is important that you are established on dialysis and that you have had a review with your consultant before arranging a holiday.
Due to infection reasons, it may not be possible to travel to all destinations. Not all dialysis units are able to take ‘holiday’ patients due to their own patient’s needs.
We will need as much notice as possible if you are planning a holiday. If you thinking of holidaying in the UK or Europe we will require at least four weeks’ notice and eight weeks for anywhere else. The more notice given the more chance there will be of space being available at your destination.
(Please do not book your holiday until you have had confirmation that your treatment has been successfully arranged)
When planning a holiday, whether in the UK or abroad, we will help to organise your treatment for whilst you are away but there are some important steps that need to be considered:
Back to topRenal Clinical Psychologist
Clinical psychologists can help people manage the emotional aspects of physical illness with practical problem solving techniques as well as counselling and more formal psychotherapy.
Having kidney disease can have a major impact on people’s lives and can be hard to deal with at times. It can be difficult to come to terms with and accept a diagnosis and adjust to the lifestyle changes that may be required. Adjusting to treatment regimens and undergoing medical procedures may make you feel anxious or upset.
Other conditions not related to your kidney disease may also affect how you deal with things. Some people can become depressed, anxious or angry about what is happening to them, such feelings of distress can be overwhelming and it may help to work through these issues with someone experienced in dealing with psychological and emotional difficulties.
What will happen if I am referred?
A referral to the clinical psychologist will be discussed with you beforehand and will only be made with your agreement. Your first meeting with the psychologist will be informal, it will be a discussion about how you are coping with all the changes and treatments, about background information and you may asked to complete a short questionnaire.
Next steps would be agreed as a joint decision between you and the psychologist.
Confidentiality
The psychologist may want to share some of the things you have discussed with other members of the renal team with the intention of helping them understand more about you.
However, for things that you want to remain confidential, this will be respected wherever possible subject to the need to consider the safety of yourself and others.
If you would like to your referral to a clinical psychologist further, ask the nursing staff in your dialysis unit.
Back to topRenal Wellbeing Team
The renal unit now has a dedicated social worker and citizens advice worker who are
happy to offer support and advice on any of the following:
The team work to enable renal patients to make the best possible use of services available
so they can remain independent in the community and enjoy a good quality of life.
How they support
- Care planning
- Mental health
- Employment and support
- Benefits and financial queries
- Immigration
- Debt advice
- Connecting with services
- Housing and adapted housing
- Guidance and support
Where we work
St James’s Hospital, Wards J48, J49 and J50. Seacroft Hospital Wards B, R & S. Renal units at Beeston, Pontefract, Dewsbury, Huddersfield and Halifax, Conservative Management, Renal Outpatients across West Yorkshire.
How to contact us
Should you wish to contact the wellbeing team they would be happy to hear from you directly or you can request a referral be made by your renal team.
Tel: 0113 206 4119
What happens to your information?
We collect information about patients from renal units and hospital systems. This statistical information is part of an annual report that helps to educate those who plan, deliver and use services for kidney patients by;
- Identify areas of best practice.
- Support research for the benefits of patients.
- Help patients and health care professionals to make decisions and plan for the future.
- Reveal areas of the country where treatment may not be available.
We do not:
- Publish information that could lead to your identity being revealed.
If you wish to opt out of sharing your information please speak to the renal unit staff or you can contact the renal registry by telephone or email:

End of Life Care (Conservative Management)

Everybody has different experiences, stories and journeys and we want our care to reflect things that are most important to you at each and every stage of your illness.
End stage kidney disease is a long term condition that can have a significant impact on your quality of life in many different ways. People can live for years on dialysis however there may come a point where the focus of your medical care changes from medical interventions, such as dialysis which prolong your life, to ones which aim to focus on maintaining your comfort.
We recognise that these can be difficult topics to discuss and may not be relevant to you until a long time in the future. However, an important part of ensuring excellent care is providing you, your family and carers with the right support, advice and medical interventions at each stage of your illness. Talking about how end stage kidney disease may affect you in the future is an important part of this process. If anything within this section is upsetting or worrying please talk to any member of the team.
There may be a point when you are seriously ill and this may affect your capacity to be involved in decisions. When we think ahead to these possibilities it may be important for you to write down what your future wishes and preferences would be so we can provide you with the best care possible.
Stopping Dialysis
You may choose to stop dialysis if:
- Your health has deteriorated making dialysis difficult.
- You feel the impact of dialysis has on the quality of your life has become unbearable.
- The Kidney team are concerned about your health and want to discuss stopping dialysis.
Whatever the reasons we want to ensure this decision making is guided by your specific wishes and preferences. We recognise that these discussions are difficult and can be emotional and upsetting. You may wish to speak with your family or friends regarding these issues before speaking with the kidney team. You may have religious or spiritual concerns about stopping this treatment and we can arrange for you to see a religious advisor if needed.
What happens when you stop dialysis?
Stopping dialysis is like stopping any other life sustaining treatment. Without dialysis your health will begin to deteriorate (get worse), eventually causing you to pass away.
On stopping dialysis you may notice that initially things are much the same however over time you will become more unwell and this can vary from person to person and will be discussed with you. Medications can be used to keep you comfortable, manage and minimise any discomfort and distress.
We may ask advice from the palliative care team regarding controlling your symptoms and support for you, your family and carers. On stopping dialysis other things to consider can include where you would like to be cared for where you would like to be cared for at the end of life. This can be in your home, a nursing home, hospital or hospice.
Documenting your wishes and preferences
As well as discussing your wishes and preferences of care, you may wish to document these in an advanced care plan. Not everyone will choose to have a conversation about their wishes and that is fine. However, talking about your wishes and planning ahead means you can make sure that what is important to you is known by the people who care about you. It can help you write down your wishes and preferences and these can be recorded and shared on a form called ReSPECT. Further advice regarding this process can be discussed with your kidney team at any point.
If you wish to talk this through more please speak with a member of the kidney team. You may wish to discuss this through with your family and friends or with your family doctor.
Back to top