This information leaflet is for patients who have been offered or are considering hysterectomy (hyster=womb and ectomy = removing).
This operation is offered for several reasons so please ask and make sure that you understand the procedure, why it is being offered to you as well as its risks, benefits and the alternative treatment options available to you.
What is a hysterectomy
A hysterectomy is an operation to remove your womb (uterus). After the operation you will no longer be able to bare children. If you have not yet gone through the menopause, you will no longer have periods.
A hysterectomy is an operation to remove your womb (uterus). After the operation you will no longer be able to bare children. If you have not yet gone through the menopause, you will no longer have periods.
Types of hysterectomy
There are several gynaecological conditions where you may be recommended a hysterectomy including:
- Heavy periods where other treatment options have not worked (see leaflet on heavy periods)
- Chronic pelvic pain thought to be caused by endometriosis (see leaflet on endometriosis)
- Chronic pelvic pain caused by chronic pelvic inflammatory disease also known as PID (see leaflet on PID)
- Prolapse of the uterus see leaflet ‘vaginal hysterectomy for vaginal prolapse)
- Cancer affecting the womb, cervix, fallopian tubes and ovaries.
How is a hysterectomy performed?
A hysterectomy can be carried out through a cut in your abdomen also known as ‘tummy’ (this is called an open hysterectomy), or through minimal access surgery including through the vagina (this is called a vaginal hysterectomy), by vNOTES (aka vaginal natural orifice transluminal endoscopic hysterectomy), or by keyhole approach (this is called a laparoscopic hysterectomy) or by robotic hysterectomy.
The type of surgery you have will depend on your personal circumstances and will be discussed with you by your gynaecologist before your operation.
You will usually have a general anaesthetic which means you will be asleep for the entire operation.
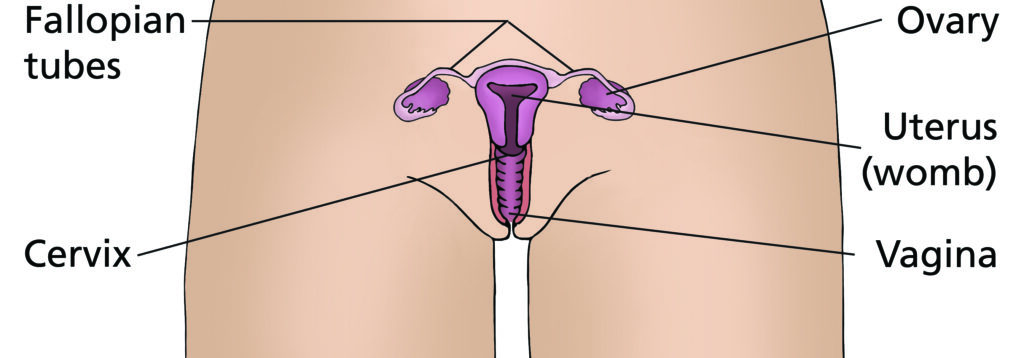
Female reproductive system
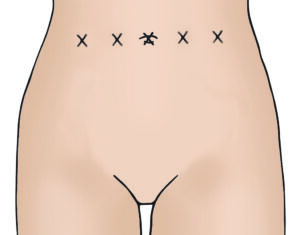
Incision sites for open hysterectomy


Incision sites for minimal access hysterectomy
This is scarless on the abdomen
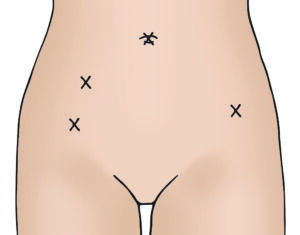
(keyhole) incisions
Regardless of the approach a vaginal/ internal examination should be performed as part of the hysterectomy procedure. This is to:
- Insert a catheter into your bladder (this may be removed soon after your procedure or may stay in for a day or so).
- Perform an examination to assess the size of your womb and pelvic organs and to see is they are mobile or stuck down (suggesting scar tissue). This helps in planning the surgery including the best surgical approach or route.
- Insert a uterine manipulator – for laparoscopic and robotic hysterectomies a tube like instrument might be placed into your uterus through your vagina in order to control the position of your uterus in order to perform the surgery.
Abdominal (open) hysterectomy
A cut is made in your abdomen that is either along the bikini line (horizontal) and at least 10 cm long or vertically (midline) from the bikini line and up to or beyond your belly button. A midline cut is made when there are large fibroids or for some types of cancer. Your uterus is removed through the cut once it has been freed of all its tissue, ligament and blood vessel connections. The cut is then closed up in layers. The skin layer is either closed with stitches or staples. An open hysterectomy is most commonly performed under general anaesthetic.
Vaginal Hysterectomy
Your uterus and cervix are removed through a hole that is made at the top of your vagina and is normally offered in women with a uterine (womb) prolapse. Special surgical instruments are placed into the vagina to remove the womb from the ligaments and blood vessels and tissues that hold it in place.
After the womb and cervix have been freed of their connections and removed, the cut at the top of the vagina is stitched up. This procedure is most commonly performed under general anaesthetic. Occasionally it is performed under regional anaesthetic (when you are numbed down from the waist down).
If you are suitable for it, your surgeon may recommend it over a open abdominal hysterectomy as it is a less invasive operation with a shorter stay in hospital, less associated pain and faster recovery.
Laparoscopic hysterectomy
A small telescopic tube with a video camera is inserted through a small cut in the abdomen (normally through the belly button) measuring 1-2 cm. Gas is inflated into your abdomen to allow visibility and access to your abdominal organs. Instruments are then inserted through other small cuts (normally 2 to 3) measuring approximately 0.5-1 cm, in the abdomen to free the uterus and cervix from its tissue, ligament and blood vessel connections so that it can be removed from the vagina. The top of the vagina is then closed laparoscopically or through the vagina.
- A laparoscopic hysterectomy is performed under a general anaesthetic.
- Laparoscopic hysterectomy is less invasive than open hysterectomy and is associated with a shorter stay in hospital (see leaflet ‘Daycase Total Laparoscopic Hysterectomy’), shorter recovery and less postoperative pain.
Vaginal NOTES hysterectomy
Vaginal natural orifice transluminal endoscopic surgery to perform hysterectomy is where a vaginal hysterectomy is performed using keyhole instruments through the vagina. Gas is passed into the abdominal cavity (as with laparoscopic and robot assisted procedure to improve visibility and access during surgery. Like a vaginal hysterectomy, vNOTES has no abdominal scars. However, vNOTES allows better access to ovaries and fallopian tubes which may not be possible to remove during a vaginal hysterectomy. Once your uterus and cervix are freed of their connections they are removed from your vagina and the top of your vagina is stitched up.
- V-NOTES is a highly technical procedure, therefore, it is currently limited to carefully selected complex cases.
- V-NOTEs hysterectomy is performed under general anaesthetic.
Robot assisted hysterectomy
This approach bears similarities to laparoscopic surgery because small cuts (about 0.8 and 1 cm are made into the abdomen (normally 4 or 5) that allow insertion of a telescope and operating instruments. The telescope cut may be bigger (1-2cm). Gas is inflated into the abdomen to allow for visibility and access to abdominal and pelvic structures during the operation. Once the instruments are set up, the surgeon sits at a control console to perform the procedure by directing the instruments with extreme precision. This route allows for better views of the pelvis and uses more advanced surgical instruments that can articulate (move into angles) that laparoscopic ones can not. It is, therefore, considered, for specific patients where complex surgical tasks are involved.
- Robot-assisted hysterectomy is performed under general anaesthetic.
What are the risks of hysterectomy?
There are general risks associated with hysterectomy; however, there are also some minor complications specific to each route. Risks are different depending on the reason for your operation, your overall health, your previous surgeries and your weight. Women who are obese, who have significant pathology, who have had previous surgery or who have pre-existing medical conditions must understand that the risks will be increased.
Rate of risks below are for abdominal hysterectomy
(Risks are usually lower for other routes of hysterectomy).
| Overall risk of serious complication | 4 in 100 (common) |
| Damage to the bladder and/or the ureter and/or long-term disturbance to the bladder function | 7 in every 1000 (uncommon) |
| Damage to the bowel | 4 in 10000 (rare) |
| Haemorrhage requiring blood transfusion | 23 in 1000 (common) |
| Return to theatre with complication | 7 in 1000 (uncommon) |
| Pelvic abscess/infection | 2 in 1000 (uncommon) |
| Venous thrombosis or pulmonary embolism | 4 in 1000 (uncommon) |
| There is a risk of hernia formation | <1 in 100 (uncommon) |
| Risk of death within 6 weeks | 32 in 100000 (rare) |
| Serious complication of the general anaesthetic | 1 in 10000 (rare) |
Frequent risks
- Infection: in the chest, urine, scars or pelvis.
- Pain, bruising, swelling on the abdomen or in the vagina, delayed wound healing or keloid formation.
- Numbness, tingling or burning sensation around the scar (this is usually self limiting, but occasionally can take weeks or months to resolve).
- Frequency of micturition and urinary tract infection.
- Ovarian failure: This is because ovaries receive some of their blood supply through the womb, which is removed during the operation.
- Vaginal vault haematoma: this is when blood collects at the top of vagina. This usually resolves and many patients will not require treatment apart from antibiotics. Occasionally, this blood collection might require surgical drainage. If your bleeding gets heavier or becomes smelly, please contact either the hospital or your GP.
- Internal scarring (known as adhesions) in the abdomen and pelvis can form, which may cause problems such as painful sexual intercourse or pelvic pain. Rarely adhesions can cause bowel obstruction.
- Women who have had a hysterectomy for pelvic pain may find that their condition has not improved. Some women may develop chronic pain after hysterectomy.
Specific risks for Laparoscopic and Robotic assisted hysterectomy
On top of the previous mentioned general risks of hysterectomy, hysterectomy via
key-hole approach (laparoscopy, robotic assisted) carries some additional specific risk:
- There is a small chance that we may not be able to gain entry to your abdomen laparoscopically or might not be able to complete the intended procedure.
- Conversion to open surgery: sometimes it is difficult or unsafe to complete the operation through keyhole surgery. Your surgeon might decide to convert to open surgery.
- Some of the injuries (up to 15%) to the surrounding organs (bladder, bowel, ureter) might not be diagnosed at the time of operation and may require addition surgery/intervention at a later date.
- Risk of urinary tract injury is greater in total laparoscopic hysterectomy than in another route of hysterectomy.
- Carbon dioxide (used during surgery) could become trapped in your abdomen. This can cause pain in one or both shoulders but disappears as the gas is reabsorbed by your body.
- In some case where the womb is too big to be extracted through the vagina or contains multiple large fibroids, it can be broken down into small pieces inside the abdomen and taken out laparoscopically using an instrument called a “morcellator”. This method avoids a big cut to your tummy and usually takes place in a bag to ensure that all the fibroid tissue is removed through one of the small cut made in your tummy.
Morcellating in a bag may also reduce the risk of spread if the fibroid tissue is found to be a malignancy (‘leiomyosarcoma’) when the tissue sample is tested in the laboratory after the operation. This precaution is taken even through the risk of a leiomyosarcoma is very low (between 1 in 500 and 1 in 7400) in women with fibroids.
Specific risks for Robotic assisted hysterectomy
- Mechanical issues with the robot
These are very rare, and the robot is monitored by Intuitive Surgery during your operation. This enables any issues to be identified and rectified. If an issue were to occur that could not be resolved, the robotic instruments are removed, and the surgery performed through open or standard keyhole surgery.
General risk of hysterectomy, specifically vaginal hysterectomy
- Vaginal vault prolapse and another prolapse
Although these operations are successful in treating uterine prolapse, they do not always stop you from getting a prolapse of the vaginal walls in the future. Recurrence of the same prolapse probably occurs in about 1 in 10 cases and it is generally believed that about 3 in 10 women who have an operation for prolapse will eventually require treatment for another prolapse.
Specific risks for vNOTES Hysterectomy
Carries the general risks of hysterectomy and some additional risks, including:
– Conversion to keyhole surgery or open surgery.
– Shoulder tip pain due to carbon dioxide entrapment.
Is there anything I should do to prepare for the operation?
Make sure that all of your questions have been answered to your satisfaction and that you fully understand what is going to happen.
Ensure that your body has all the nutrients it needs by eating a healthy balanced diet. A healthy diet is high in fibre (fruit, vegetables, wholegrain bread and cereal) and includes up to two litres of fluid a day, mainly water. Remember to eat at least five portions of fruit and vegetables each day. There is no reason to gain weight after your operation if you follow the dietary advice and take regular exercise.
We strongly advise that you stop smoking before your operation. The longer you are smoke free before your operation, the better. Continuing to smoke before surgery can increase the risk of complications involving your heart, lungs and surgical wounds. Any of these may result in you having a slower recovery and a longer stay in hospital. Speak to your GP, practice nurse or local pharmacist for advice about stopping smoking. You can use nicotine replacements during your hospital stay if required.
Before you come into hospital for your operation, try to organise things ready for when you come home. If you have a freezer, stock it with easy to prepare food.
Arrange for relatives and friends to do your heavy work (such as changing your bedding, vacuuming and gardening) and to look after your children or other dependents if necessary. Arrange for somebody to take you home when you are discharged.
What happens after my operation?
Most modern anaesthetics are short lasting. You should not have, or suffer from, any after-effects for more than a day after your operation. During the first 24 hours you may feel more sleepy than usual and your judgement may be impaired. You will usually be given oxygen, to help you breathe comfortably, immediately after your operation.
The nursing staff will regularly check your blood pressure, pulse, temperature and any blood loss from your vagina or wound. They will also check that you are comfortable.
Catheter
You may have a catheter (tube) in your bladder to allow drainage of your urine. This will usually be removed the day after your operation when you are able to walk to the toilet to empty your bladder. If you have any problems passing urine, you may need to have a catheter for a few more days.
Vaginal pack
If you have had a vaginal hysterectomy or LAVH, then you may have a pack (a length of gauze, like a large tampon) in your vagina to reduce the risk of bleeding. This is usually removed by a nurse the day after your operation.
Vaginal bleeding
You can expect to have some vaginal bleeding for 1-2 weeks after your operation although it can sometimes last for up to six weeks. This is like a light period and is red or brown in colour. Some women have little or no bleeding initially and have a sudden gush of old blood or fluid about 10 days later. This usually stops quickly. You should use sanitary towels rather than tampons, as using tampons could increase the risk of infection.
Drain
Occasionally a drain (small tube) is inserted through your abdominal wall to drain off any blood or fluid which can accumulate immediately after your operation. This is usually removed by a nurse after your operation while you are still in hospital.
Pain and discomfort
The degree of pain or discomfort experienced by patients following surgery varies a great deal. A common side effect of laparoscopic surgery is to have some pain in your shoulders.
You may have a device that you use to control the pain yourself (Patient Controlled Analgesia System or PCAS). Alternatively you may have pain killers in the forms of tablets, injections or suppositories. Taking painkillers as prescribed to reduce your pain will enable you to get out of bed sooner, stand up straight and move around – all of which will speed up your recovery and help to prevent the formation of blood clots in your legs or your lungs.
Examples of post operative pain relief to take (you can buy these from a Chemist). Please make sure that you do not have allergies to these medications before taking them
Paracetamol
Adults weighing more than 50 kilograms can take two tablets (each tablet is 500mg), 4 times in 24 hours. You must wait at least 4 hours between doses. Do not take more than 8 tablets in 24 hours.
Ibuprofen
Adults weighing more than 50 kilograms can take two tablets (200mg tablets) every 4 to 6 hours, but shouldn’t take more than 1,200mg (6 x 200mg) tablets in the space of 24 hours.
Trapped wind
Following your operation your bowel may temporarily slow down causing air or ‘wind’ to be trapped. This can cause some pain or discomfort until it is passed. Getting out of bed and walking around will help. Peppermint water and peppermint tablets may also ease your discomfort. Once your bowels start to move, the trapped wind will ease.
Eating and drinking
You may have a drip in your arm to provide you with fluids. You may be offered a drink of water or a warm drink and something light to eat, a few hours after your operation. If you are not hungry initially, you should drink fluids. Try eating something later on.
Washing and showering
If you have had an abdominal hysterectomy, you will be assisted to have a wash the day after your operation. You can then shower independently on the following days. If you have had a vaginal or laparoscopic (keyhole) hysterectomy then you can have a shower the day after your operation.
Scars, stitches and dressings
Abdominal (open) hysterectomy
Is usually carried out through a cut which is at least 10cm long. This is usually made across the top of your pubic hairline (‘bikini line’ incision) but may sometimes run up and down from up to and beyond your belly button (midline incision). You will have a dressing on your wound which can be removed five days after your operation. Most patients have dissolvable stitches which do not need removing. If you have non-dissolvable stitches or staples/clips, you will have to get them removed 7 to 10 days after surgery through your practice or district nurse. Any stitches in your vagina will not need to be removed as they are dissolvable.
Vaginal hysterectomy and vNOTES hysterectomy
Is carried out through your vagina so your scar will be out of sight. The stitches in your vagina will not need to be removed as they are dissolvable. You may notice a stitch or part of a stitch coming away after a few days or weeks. This is normal and nothing to worry about.
Laparoscopic hysterectomy and Robot Hysterectomy
If you have keyhole surgery as part of your operation you will have between three and four small scars on different parts of your abdomen. Each scar will be between 0.5cm and 1cm long. Your cuts may be closed by glue or stitches which are usually dissolvable. Initially your cuts will be covered with dressings. You should be able to take these off about 24 hours after your operation. Any stitches in your vagina will not need to be removed as they are dissolvable.
Formation of blood clots – how to reduce the risk
There is a small risk of blood clots forming in the veins in your legs and pelvis (deep vein thrombosis) after any operation. These clots can travel to the lungs (pulmonary embolism) which could be serious. You can reduce the risk of clots by being as mobile as you can, as early as you can, after your operation. You can also do exercises when you are resting, for example:
- Pump each foot up and down briskly for 30 seconds by moving your ankle
- Move each foot in a circular motion for 30 seconds
- Bend and straighten your legs – one leg at a time, three times for each leg
Whilst you are in hospital you will be given a daily injection of heparin and you will be asked to wear compression stockings (known as TEDS). Both of these measures also help to reduce the risk of blood clots.
When can I go home?
If you have had a laparoscopic or vaginal hysterectomy you may be able to go home 1-2 days after your operation depending on your circumstances.
If you have had an abdominal hysterectomy you can usually go home three days after your operation.
Will I need Hormone Replacement Therapy (HRT)?
If your ovaries have been removed during your operation you may be offered HRT if you are premenopausal at the time of surgery. This will be discussed with you by your gynaecologist and together you can decide the best way forward. Your GP will be advised on an HRT treatment plan.
Should I continue to have cervical smears?
If you have a subtotal hysterectomy (where your cervix is kept) you will need to continue having cervical screening unless you have completed the cervical screening programme.
If you have had a total hysterectomy (where your cervix is removed) you may need to continue to get smears of the top of your vagina if you have a history of abnormal cervical smears or if the biopsy of your removed cervix shows abnormal cells. Check with your GP or gynaecologist whether this applies to you.
Having sex
You should usually allow 4-6 weeks after your operation to allow your scar to heal. It is then safe to have sex – as long as you feel comfortable. If you experience any discomfort or dryness (which is more common if your ovaries have been removed at the time of the hysterectomy) you may wish to try a vaginal lubricant. You can buy this from your local pharmacy.
Tiredness and feeling emotional
You may feel much more tired than usual after your operation as your body is using a lot of energy to heal itself.
You may need to take a nap for the first few days. A hysterectomy can also be emotionally stressful and many women feel tearful and emotional at first – when you are tired these feelings can seem worse.
Pelvic-floor muscle exercise programme
Your pelvic floor muscles span the base of your pelvis. They work to keep your pelvic organs in the correct position (prevent prolapse), tightly close your bladder and bowel (stop urinary or anal incontinence) and improve sexual satisfaction.
It is important for you to get these muscles working properly after your operation, even if you have stitches. To identify your pelvic-floor muscles, imagine you are trying to stop yourself from passing wind and at the same time trying to stop the flow of urine. When you do this you should feel your muscles ‘lift and squeeze’.
It is important to breathe normally while you are doing pelvic floor exercises. You may also feel some tightening in your lower abdominal muscles. This is normal. Women used to be told to practise their pelvic-floor muscle exercises by stopping the flow of urine midstream. This is no longer recommended, as your bladder function could be affected in the longer term.
You can begin these exercises gently once your catheter has been removed and you are able to pass urine on your own.
You need to practice short squeezes as well as long squeezes:
- Short squeezes are when you tighten your pelvic-floor muscles for one second and then relax.
- Long squeezes are when you tighten your pelvic-floor muscles, hold for several seconds and then relax.
Start with what is comfortable and then gradually increase – aiming for ten long squeezes, up to 10 seconds each, followed by ten short squeezes.
You should do pelvic-floor muscle exercises at least three times a day. At first you may find it easier to do them when you are lying down or sitting. As your muscles improve, aim to do your exercises when you are standing up. It is very important to tighten your pelvic-floor muscles before you do anything that may put them under pressure, such as lifting, coughing or sneezing. Make these exercises part of your daily routine for the rest of your life. Some women use triggers to remind themselves, such as brushing their teeth, washing up or commercial breaks on television.

Seeking medical advice after a hysterectomy
While most women recover well after a hysterectomy, complications can occur – as with any operation. You should seek advice from your GP or the ward you were on if you experience:
- Burning and stinging when you pass urine or if you pass urine frequently: this may be due to a urine infection. Treatment is with a course of antibiotics.
- Heavy or smelly vaginal bleeding or bleeding which starts again: If you are also feeling unwell and have a temperature (fever), this may be because of an infection or a small collection of blood at the top of the vagina, called a vault haematoma. Treatment is usually with a course of antibiotics. Occasionally you may need to be admitted to hospital for the antibiotics to be administered intravenously (into a vein). Rarely, haematomas may need to be drained.
- Red and painful skin around your scars: this may be caused by a wound infection. Treatment is with a course of antibiotics.
- Increasing abdominal pain: if you also have a temperature (fever), have lost your appetite and are vomiting, this may be because of damage to your bowel or bladder, in which case you will need to be admitted to hospital.
- A painful red, swollen, hot leg or difficulty bearing weight on your legs: this may be caused by a deep vein thrombosis (DVT). If you have shortness of breath, chest pain or cough up blood, it could be a sign that a blood clot has travelled to the lungs (pulmonary embolus). If you have these symptoms, you should seek medical help immediately.
Getting back to normal
Around the house
While it is important to take enough rest, you should start some of your normal daily activities when you get home and build up slowly. You will find that you are able to do more as the days and weeks pass.
For the first 1-2 weeks you should restrict lifting to light loads such as a one litre bottle of water, kettles or small saucepans. If you need to iron just do a couple of items at a time. Try to sit down to prepare food or sort laundry. Follow the recovery guides at the back of this booklet for more information.
Establish a daily routine and keep it up. For example, try to get up at your usual time, have a wash and get dressed, move about and so on. Sleeping in and staying in bed can make you feel depressed. Try to complete your routine and rest later if you need to.
Your bowels
Your bowels may take time to return to normal after your operation. Your motion should be soft and easy to pass. You may initially need to take laxatives to avoid straining and constipation. You may find it more comfortable to hold your abdomen (provide support) the first one or two times your bowels move. If you do have problems opening your bowels, it may help to place a small footstool under your feet when you are sitting on the toilet so your knees are higher than your hips. If possible, lean forwards and rest your arms on top of your legs to avoid straining.
Exercise
While everyone will recover at a different rate, there is no reason why you should not start walking on the day you return home. You should be able to increase your activity levels quite rapidly over the first few weeks. There is no evidence that normal physical activity levels are in any way harmful and a regular and gradual build up of activity will assist your recovery. If you are unsure, start with short steady walks close to your home a couple of times a day for the first few days. When this is comfortable you can gradually increase the time while walking at a steady pace. Many women should be able to walk for 30-60 minutes after two or three weeks.
Swimming is an ideal exercise that can usually be resumed within 2-3 weeks as long as vaginal bleeding and discharge has stopped. If you build up gradually, the majority of women should be back to previous activity levels within 4-6 weeks.
More strenuous sports should be avoided for at least six weeks, although this will depend on your level of fitness before your surgery.
Driving
It can be 3-6 weeks before you are able to drive again. Ask your insurance company when you will be insured to start driving again. Make sure you are able to sit comfortably with a seat belt, work the controls and perform an emergency stop. When you are ready to start driving again, build up gradually, starting with a short journey.
Travel plans
If you are considering travelling during your recovery, it is helpful to think about:
- The length of your journey: journeys over four hours where you are not able to move around (in a car, coach, train or plane) can increase your risk of deep vein thrombosis (DVT). This is especially so if you are travelling soon after your operation.
- How comfortable you will be during your journey, particularly if you are wearing a seatbelt.
- Overseas travel: Would you have access to appropriate medical advice at your destination if you were to have a problem after your operation? Does your travel insurance policy cover any necessary medical treatment in the event of a problem after your operation?
If you have concerns about your travel plans, it is important to discuss these with your GP or the hospital where you had your operation before travelling.
Support from your family and friends
You may be offered support from your family and friends in lots of different ways. It could be practical support with things like shopping, housework or preparing meals. Most people are only too happy to help – even if it means you having to ask them! Having company when you are recovering gives you chance to say how you are feeling after your operation and can help to lift your mood. If you live alone, plan in advance to have someone stay with you for the first few days when you are home.
Returning to work
Everyone recovers at a different rate, so when you are ready to return to work will depend on the type of work you do, the number of hours that you work and how you get to and from work.
You may experience more tiredness than normal after any operation, so your return to work should be like your return to physical activity, with a gradual increase in the hours and activities at work.
If you have had a laparoscopic or vaginal hysterectomy you may be fit for work after 2-3 weeks. If you have had an abdominal hysterectomy you may be fit for work after 3-4 weeks. Most women are able to go back to normal work after 6-8 weeks if they have been building up their levels of physical activity at home.
Returning to work can help your recovery by getting you back into your normal routine again. Some women who are off work for longer periods start to feel isolated and depressed. You do not have to be symptom free before you go back to work. It is normal to have some discomfort as you are adjusting to working life. It might be possible for you to return to work by doing shorter hours or lighter duties and building up gradually over a period of time. Consider starting partway through your normal working week so you have a planned break quite soon.
You might also wish to see your GP or your occupational health department before you go back and do certain jobs – discuss this with them before your operation. You should not feel pressurised by family, friends or your employer to return to work before you feel ready. You do not need your GP’s permission to go back to work. The decision is yours.
Recovery after a minimal access hysterectomy (vaginal, vNOTEs, laparoscopic and robotic)
| Days after my operation | How might I feel? | What is safe to do? |
| 0-2 days | You will have some aches & pains in your tummy. You will feel sore moving in and out of bed. You may have some light bleeding like a period. You will feel tired and may feel like a sleep in the afternoon. You will usually go home in this time. | Get out of bed and move about. Go to the toilet. Get yourself dressed. Eat and drink normally. |
| 3-7 days | Your pains should be reducing in intensity now and you will be able to move about more comfortably. You will still tire easily. | Go for short walks. Wash and shower as normal. |
| 1-2 weeks | Your energy levels will be increasing. There will be less pain as you move about. | Your energy levels will be increasing. There will be less pain as you move about. |
| 2-4 weeks | There will be even less pain now as you move about more. You will find your energy levels are returning to normal. You should feel stronger every day. | Return to work depending on your occupation. Carry out daily activities like shopping, vacuuming, ironing, light gardening, gentle exercise and driving. Check with your insurance company before you drive and make sure you can do an emergency stop without any pain. |
| 4-6 weeks | Almost back to normal. You may still feel tired and need to rest more than usual. | Usual exercise. Have sex if you feel ready. Swimming if your bleeding has settled. |
Recovery after an abdominal (open) hysterectomy
| Days after my operation | How might I feel? | What is safe to do? |
| 0-2 days | You will have some aches & pains in your tummy. You will feel sore moving in and out of bed. You may have some bleeding like a light period. You will feel tired and may feel like a sleep in the afternoon. | Get out of bed and move about. Go to the toilet. Get yourself dressed. Start eating and drinking as usual. Gentle exercises like moving your ankles up and down to help with circulation. Stand up for 10 minutes at a time. |
| 3-7 days | You will return home. Your pains should be reducing in intensity which will allow you to move about more easily. You will still tire easily. | Go for short walks. Wash and shower as normal. |
| 1-2 weeks | You will have less pain as you move about. | Slowly build up your activity levels (longer walks). Lift a kettle to make tea or coffee. |
| 2-4 weeks | You should feel like you are getting stronger every day. | Continue to build up the amount of gentle activity that you do. Plan for your return to work. |
| 4-6 weeks | You should continue to feel stronger every day. Vaginal bleeding should have settled or be very little. | Carry out daily activities like shopping, vacuuming, ironing and driving. Swimming if your bleeding has settled. Check with your insurance company before you drive and make sure you can do an emergency stop without any pain. Have sex if you feel ready. |
| 6 weeks onwards | Almost back to normal. You may still feel tired. It is ok to rest. | Carry out all normal daily activities. Sport – You may start gently after 6-8 weeks. |
Contact us
Gynaecology Acute Treatment Unit (GATU)
Open 24 hours.