This leaflet provides information to potential donors about the Live Donor Liver Transplant Service at the Leeds Teaching Hospitals.
Introduction
Your friend, relative or child has been diagnosed with severe liver disease and the doctors looking after them have explained that a liver transplant is now necessary. Patients requiring a liver transplant are placed onto a liver transplant waiting list and are regularly reviewed until a cadaver or deceased donor (someone who has died and donated their organs) becomes available.
This information booklet will tell you about the living donor liver transplant program and the donor assessment procedure. It will identify the risks and benefits of the surgery and you should spend time considering and understanding what impact this procedure may have on you. It is important that you read this booklet carefully.
Members of the medical team, including the transplant coordinators will be available to explain any aspects which you do not fully understand or that require further explanation.
When you have read through this information booklet there is a section at the end called ‘What next’? this tells you what to do if you want to be considered as a donor.
What is Live Donor Liver Transplantation?
Most livers available for transplantation are from deceased donors, sometimes referred to as cadaver donors, i.e., they come from a person who has died because of overwhelming and irreversible brain damage.
In such circumstances it is possible for organs, such as the liver to be donated for transplantation.
The timing of a donor becoming available is very unpredictable and the quality of these organs, although generally very good, is not always certain.
Your relative or friend will be placed onto the national waiting list, while a decision on the suitability of the live liver donor is made. If a suitable matched liver becomes available from a deceased donor then we would use this organ rather than continue with the live donor assessment.
Undergoing a live liver donor assessment will not affect your friend or relative’s position on the national waiting list.
Living liver donation is considered a good option as the availability of deceased donor organs is unpredictable, some patients simply cannot wait long enough for such a liver to become available.
Nationally the number of patients who are waiting for a liver transplant is ever increasing. Patients may have to wait more than a year for a deceased donor liver to become available. As a result of this, approximately 10% of patients on the waiting list either die before an organ becomes available or are removed from the waiting list because they become too sick to survive the operation.
The liver has two important features that make living donation possible.
- It is much larger than we need (so it has a great ‘reserve’).
- It can regenerate within weeks if part of it is removed.
Live donor liver transplantation (sometime abbreviated to LDLT) involves removing part of your healthy liver and transplanting it into another person with liver failure.
The remaining liver, or remnant in the live donor will re-grow within weeks back to nearly its original size.
LDLT is carried out in many countries, including the United Kingdom. The Leeds LDLT programme opened in 2007 and is the leading centre for this service in the UK.
It has three distinct advantages in comparison to waiting for an organ from a deceased donor;
- It provides a unique opportunity to restore good health to a close friend or relative.
- It provides a guaranteed high quality organ.
- The transplant can take place at a specific time before the recipient’s health deteriorates.
One big disadvantage however is that a healthy person, the donor, has to undergo major surgery. This decision requires some careful thought and consideration on the impact that live liver donation may have on you and your family.
What does Live Donor Liver Transplantation involve?
As your friend, relative or child is seriously ill from liver disease, your first thought when considering becoming a donor will have been to help them recover. This is, of course, a very natural reaction and one that most people will understand.
However, live donor liver donation is not possible for every potential donor; only 1 in 3 relatives or friends are able to donate for a variety of reasons.
This booklet is designed to help you understand the following:
- The living donor assessment, including the risks and benefits.
- The living donor operation itself, including the risks of surgery.
- The long-term outcome of donor liver surgery.
As you read through this booklet you must be clear that:
- Starting an assessment to become a donor, does not obligate you to be a donor. You can stop the process at any point, right up to the day of surgery.
- We would expect you to discuss your intention to potentially donate part of your liver with close family members.
- As a live liver donor you must not be under any pressure to become a donor. If the team undertaking the assessment have any doubt that this is happening then the process will stop.
For directed live liver donor
- You do not have to tell your intended recipient at this stage as hopes may be dashed if you are not suitable or decide not to donate.
- If you are not suitable as a live liver donor, your friend, relative or child will remain on the deceased donor waiting list. If a deceased donor becomes available during the assessment process, then we will go ahead with that and so avoiding the need for live liver donation.
- Your friend or relative must agree to receive a live donation.
Your safety as a potential donor is the top priority of the live donor team throughout the assessment. The whole process may take about 6-8 weeks to complete. This may be longer if any unsuspected abnormalities are found that require further investigation. We will keep you informed at every stage throughout the process.
All members of the live liver donor team must be certain that living liver donation is a safe and appropriate option for you and the recipient.
The flow chart on below, shows the donor assessment pathway.
Donor Assessment Pathway
- Process takes between 6-8 weeks.
Initial Enquiry
- Donor Information Booklet provided.
Register interest
Call or email to register interest.
- Complete Medical Health Questionnaire
- LDLT team will contact you. Donor Education provided.
Stage 1
- Attend LDLT clinic at SJUH. Blood work up.
- Hepatology/Surgical/Live donor coordinator review.
Stage 2
- Complete psychiatry questionnaire.
- Psychiatry review.
Stage 3
- Attend SJUH for CT/MRI Liver/CXR/ECG.
- Anaesthetic review.
Stage 4
- Independent Assessment (IA) for HTA.
Stage 5
- Multidisciplinary Case Review.
- Donor Advocate Physician Review.
- Donor Surgery Date set.
Initial Enquiry
If you would like to be considered as a potential live liver donor you must meet our inclusion criteria. You must be aged between 18-60 for directed donation or 18-50 for altruistic donation. You must have a BMI of less than 30, be a non-smoker and be in excellent physical and psychological health. We will email you a medical health questionnaire to complete.
We would ask that when you return it you include proof of your BMI.
The medical questionnaire looks at your current and past health status to ensure you have no significant medical problems that may exclude you from further evaluation.
We would at this stage ask your permission to get in touch with your GP, we will ask the GP to complete a medical health questionnaire about you.
Smokers must cease smoking for at least 4-6 weeks before we could consider you as a potential donor.
A donor must be blood group compatible with the recipient. You can check your blood group if you don’t know it using an at home testing kit called an Eldon Kit.
The result of this Eldon test is evidence of your blood group and should be returned with the completed health questionnaire. Details on how to obtain one of these kits are available at the back of this leaflet.
Blood Type Compatibility
Blood Type: 0
- Can receive a liver from blood type: O.
- Generally can donate a liver to blood types: O, A, B and AB.
Blood Type: A
- Can receive a liver from blood types: A and O.
- Generally can donate a liver to blood types: A and AB.
Blood Type: B
- Can receive a liver from blood types: O and B.
- Generally can donate a liver to blood types: B and AB.
Blood Type: AB
- Can receive a liver from blood types: O, A, B and AB.
- Generally can donate a liver to blood type: AB.
When we have received your health questionnaire, we will give you a 15-30 minute telephone call to discuss your answers, this will also provide you with an opportunity to ask any questions. We will agree a date to attend a face-to-face outpatient clinic appointment.
We will also agree a time before your planned clinic appointment to have a virtual appointment, at this we will give you some important information to consider before your clinic appointment.
Stage 1
- When you attend the live donor assessment clinic you will be seen by a hepatologist and liver transplant surgeon who both specialize in live liver donation. You will also meet one of the live donor transplant coordinators. This is the Live Liver Donation Assessment Team (LD team). At the end of your assessment all team members must unanimously agree that you are medically and psychologically suitable to donate.
- The purpose of this appointment is for you to meet the team and to ensure that you understand all the contents of this booklet and talk through any concerns you have.
- We will discuss the risks of live donor surgery, both for the donor and the transplant recipient. We will also explain to you that if you commence the assessment process that you can withdraw at any time without further explanation.
- If you are wanting to embark upon the donor assessment process, we will also do some blood tests at this stage.
- We will ask you to sign a consent form for investigations and blood tests.
- These include tests to see how your liver and kidneys are functioning, tests to exclude the presence of cancer and the presence of any diseases that can be transmitted from donor to recipient.
- The blood tests will include an HIV test. If any of the tests come back as positive or show abnormalities we will inform you and provide you with appropriate support and guidance.
- The Human Tissue Act 2004 forbids payments of any kind for the supply of organs. However, it does permit payment of reasonable expenses to a donor for any travel, accommodation and loss of earnings directly incurred during the assessment process or if surgery goes ahead.
- The transplant coordinator will give you information about this scheme at the beginning of your assessment and will help you throughout your journey with this process.
- When the team have reviewed your blood tests, one of them will contact you to discuss the results. If no abnormalities are present and you wish to proceed you will then be put forward to Stage 2.
Stage 2
- Stage 2 of the assessment involves completing a psychiatry questionnaire. This will be given to you at your clinic appointment or we will email it to you.
- When you return this to the LD team we will arrange either a telephone or video appointment with a psychiatrist.
- The questionnaire looks at both your emotional and physical health and the extent to which either or both impact your normal daily living.
- The psychiatrist will review in depth your motivation to donate.
- The psychiatrist will also explore how you would feel if the recipient outcome was unfavorable, or the transplanted liver failed.
- It is important that all prospective donors understand that the long-term success of a transplant operation can never be guaranteed.
- The psychiatrist will report back to the LD team. Once we have this report and no issues are raised you can move on to the third stage of the assessment.
- We offer all potential live donors the opportunity of being able to talk to a donor who has already been through this process and donated. If you feel you would benefit from this please ask the LD team.
Stage 3
- The team must be certain that the partial hepatectomy (the name given to the operation whereby part of your liver is removed) will be technically possible and safe for you as the donor.
- In order to do this we would ask you to come back to Leeds for a CT and MRI scan of your liver. These scans can only be undertaken here at St James’s Hospital.
- The CT scan will focus on identifying the anatomy and size of your liver, ensuring that the remnant of your liver (the piece left behind) is sufficient for you and that there is an adequate amount of liver to transplant into the recipient.
- The MRI scan looks at the biliary system within the liver, confirming that this can be safely divided for two people.
- Your scans will be reviewed by specialist radiologists who will calculate your liver volumes and report on specific anatomy. The radiologists will present their findings to the surgical team. All have to be in agreement that you can donate part of your liver safely.
- You will also undergo an anesthetic review with a consultant anaesthetist. They will ensure you are fit for a general anesthetic. As part of this assessment you will be required to have an ECG (Electrocardiogram) and chest X-Ray.
- The anesthetist will also talk to you about pain control options in the post operative period.
- Once this is complete you are now ready to move on to stage four.
Stage 4
- The Human Tissue Authority (HTA) is the governing body that over sees all live donor transplant activity in the UK. Stage 4 involves meeting with a person titled ‘Independent Assessor’ (IA) who acts on behalf of the HTA.
- If you know the person who you will be donating to, you will be asked to provide evidence of your relationship to that person. You will also be required to provide photo ID such as a passport or driving license. It may be necessary for you to provide further evidence such as birth certificates or marriage certificates. The transplant coordinator will inform you what is required and help you with this.
- When the IA is satisfied with all the evidence they have collected they will submit this to the HTA to seek permission for the live liver donor transplant to go ahead. The HTA will look at the evidence and then let the donor team know of their decision.
- This can take up to 10 working days from the date of the application submission.
- Whilst we are waiting for your HTA application to come back we will move on the final stage of the process.
Stage 5 – MDT review and donor advocate physician review
- We will arrange for you to have an appointment with a Donor Advocate Physician (DAP). The DAP is a senior medical doctor independent of the LD team. They will review your medical assessment and then speak to you to ensure that you understand the implications of donation.
- The LD team will hold an MDT (Multi-Disciplinary Team) meeting to review your case, if they are happy with everything then they will consider setting a date for surgery.
- Sometimes planned surgeries are unavoidably cancelled but will be rearranged within a short time scale.
The Living Donor Operation
The surgeon performing the operation will explain the procedure to you in detail. The description outlined below is only a basic outline of the procedure.
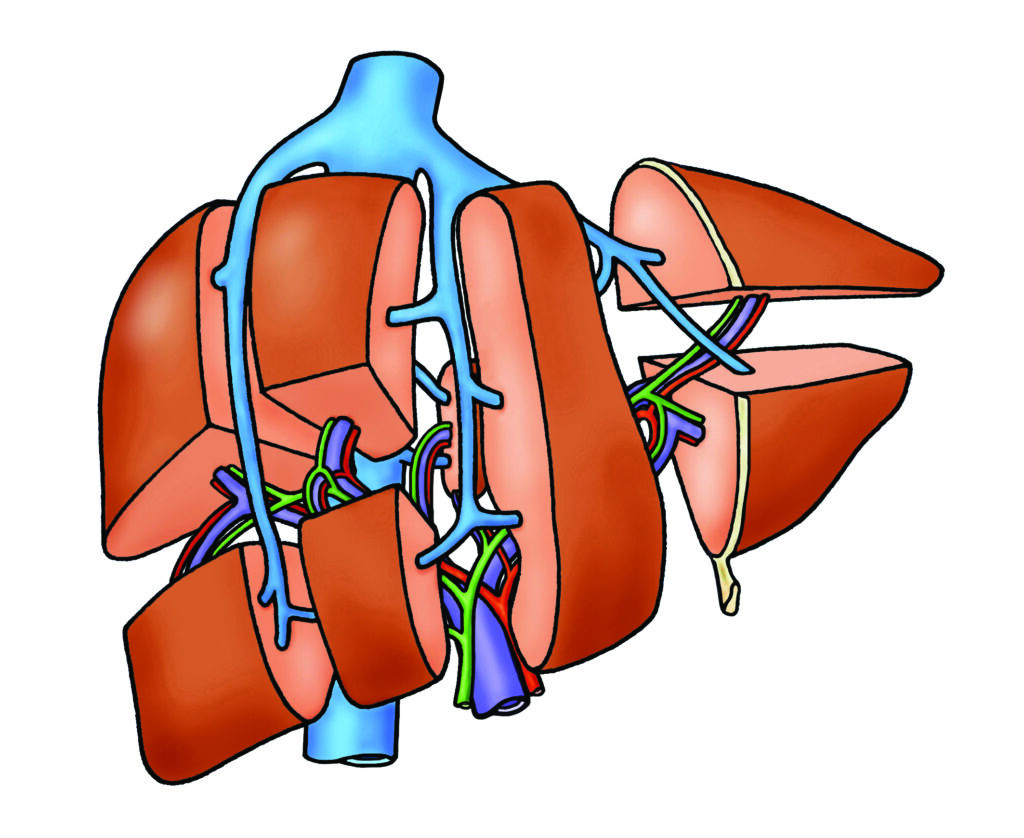
1. Donor Liver
2. Donor Liver Removal
It is possible to split the liver in different ways, the type of surgery depends upon whether the transplant recipient is an adult or child or on the size of the donor liver.
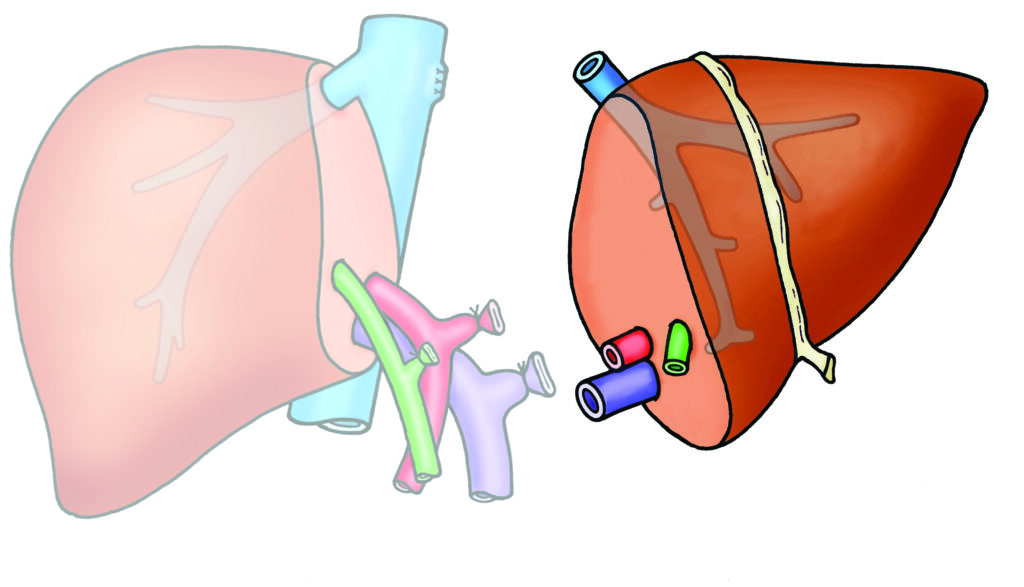
3. Donor Liver (Right Hemihepatectomy)
The donor operation that removes segments 5,6,7 & 8 of the liver is known as a right hemihepatectomy, this operation removes approximately 60% to 70% of the entire liver.
This is the most common type of live donor hepatectomy in adult to adult live liver transplantation.

4. Donor Liver (Left Hemihepatectomy)
The donor operation that removes segments 2, 3 & 4 of the liver is known as a left hemihepatectomy, this operation removes approximately 40% of the entire liver.
This type of donor operation is usually undertaken when an adult donates to a child or an adult with a large liver donates to an adult.
5. Donor Liver (Left Lateral Sectionectomy)
The donor operation that removes segments 2 & 3 of the liver is known as a left lateral sectionectomy, this operation removes approximately 20% of the entire liver.
This type of donor operation is usually done when an adult donates to a small child.

6. Post-operative care
- The donor surgical procedure takes around 3 to 4 hours. When surgery is complete you will be transferred to a High Dependency Area.
- At day 1 or day 2 after your surgery and depending on your condition you will be transferred to a liver ward.
- All donors will be on our Enhanced Recovery after Surgery Program. Donors can usually start eating and drinking as soon as they feel able too. Until then you will be given fluids via a ‘drip’ into a vein. You may have various drainage tubes placed during surgery, like your bladder catheter, stomach tube, or abdominal drain, these will be removed within a few days and when safe to do so.
- You will have various blood tests and maybe an ultrasound scan during this recovery period.
- Some patients may develop mild jaundice after surgery which resolves without any treatment. Occasionally this may persist and an ultrasound scan and other tests will be done to rule out any complications.
- Most patients are discharged from hospital between 5 – 7 days post-op.
- Live donors are given a blood thinning injection daily after surgery; this reduces the likelihood of complications from a blood clot forming. This daily injection continues for several weeks following surgery. Most patients learn to give this injection to themselves and do so at home without difficulty.
- It is important to be physically active after surgery in order to reduce the risk of forming blood clots.
- Donors are advised to avoid air travel and prolonged car journeys for 4 weeks after surgery. If a long car journey is necessary during the first 3 months after surgery, then we advise you to stop the car every hour and walk around for 15 minutes to promote blood flow to the legs. A daily walk is advised after discharge to help build up stamina.
- Most complications are soon after surgery, but some may appear after discharge home. Patients must contact the LD team if they develop new abdominal pain, redness around the wound, yellow skin, fever, cough or shortness of breath or any other medical concern.
- A follow-up clinic visit will be arranged for 4 weeks after discharge.
What are the risks and potential complications of the operation?
The assessment process continues right up to the point of your liver being examined at the time of surgery to check it is still safe to proceed. In a very small number (1%) of cases the surgery is stopped at this point. If an unexpected reaction to the anaesthetic occurs, then surgery will not proceed. This is rare but can occur in anything up to 5% (1 in 20) of such surgical procedures.
The risks associated with the procedure can be divided as Anaesthesia risk (1) and Surgical risk (2).
1. Anaesthetic Risk
You will need an anaesthetic for your operation. During your assessment the anaesthetist will have already explained the anaesthetic and post operative care procedure. You may need special drips and tubes for the operation and these may include:
- An arterial line – (Common) A small drip into an artery in the wrist, this is used to monitor your blood pressure. The main complication is damage to the artery. This is an extremely rare complication, but has potentially serious consequences including the need for repair of the artery.
- A central line – (Rarely) This is a drip through the vein in the side of your neck which passes down into your heart. This is used for monitoring pressures during the operation, and to give drugs. There are small risks associated with insertion of this line; these include bleeding, puncture of lung and infection. Central lines are used commonly in surgery, and serious complications are rare.
- Epidural catheter – (Rarely) This is placed between the bones of your back for pain relief and to control your blood pressure and minimise blood loss during the operation. There is a small risk of complications with this procedure, the most serious is permanent nerve injury resulting in loss of sensation or partial paralysis, this may occur once in every 30,000 cases. Infection is also a rare complication.
- Wound catheters – (Common) These are placed at the end of surgery, they are narrow tubes that will deliver a continuous infusion of local anaesthetic into the wound and surrounding area, they usually last for approximately 48 hours and are then removed.
2. Surgical Risks
Any abdominal surgery causes pain and discomfort and carries a risk of bleeding, infection and injury to nearby organs. Infections can include pneumonia, urinary tract infections and skin infections. The most common surgical complications after donor surgery are:
- Bile leak – this is because bile can leak from the cut surface of the divided liver. This occurs in 5-15% of operations and may require a further procedure afterwards (usually done in the X-ray department). Further surgery might be required also.
- Deep vein thrombosis / pulmonary thrombosis – patients having operations on their abdomen are at risk of developing blood clots in their legs and lungs whilst recovering. These are potentially serious complications. You will wear special stockings during and after surgery to help prevent this complication, and you will be encouraged to get up and move around as soon as possible. You will also be given a small injection of heparin once a day after your operation to prevent this possible complication.
- Gallbladder removal – during surgery it may be necessary to remove the gall bladder. This is more common in right liver lobe donation. Gall bladder removal is a very common operation but there are some risks involved with this procedure. The most common risk it that for a period of time the person develops diarrhoea. This usually only lasts for a short period of time but for a small number of people this can be persistent. This condition is known as post-cholecystectomy syndrome and it occurs in about 4% – 18% of donors.
- Gastro-intestinal problems – can occur in the post-operative period, these can occur in about 0.8 % to 9 % of donors.
- Insufficient liver – very rarely (less than 1:200 cases) removing part of the liver leaves insufficient healthy liver and causes liver failure in the donor. If the donor’s liver does not recover; the donor may require an emergency transplant (0.4%) The purpose of all the tests performed prior to surgery is to minimise the chance of this happening.
- Death – every step is taken to minimise this risk to you as a donor having surgery. However, it is impossible to eliminate every risk. It is estimated that the risk of dying from this type of surgery is between 1:200 and 1:500. This must be carefully considered and discussed with your family.
The Long-Term Outcome of Living Donor Surgery
The following long-term outcomes of this type of surgery should be considered:
- Most donors are fit to return to work after about 4 to 8 weeks depending upon their type of work. And return to heavy manual work and normal sporting activities by three months. However, this does vary from person to person.
- Your abdominal scar will fade over time but will always be visible and a small number of people complain of long term wound pain. Anybody with an abdominal surgical wound has the potential risk of developing a hernia.
- Becoming a living donor should not affect your Life Insurance Policy but might affect other insurance policies such as health insurance, mortgage policies etc. Potential donors should check their own policies and discuss their intention with the companies involved.
- We would also recommend that you discuss your intention to donate with your employer.
- Donors will be reviewed in the outpatient department early after discharge home and regularly reviewed in the first year. After that we would expect donors to be followed up life long, this will mean an annual telephone clinic consultation.
What Next?
If you have further questions or want more information please contact the live donor team, contact details below.
If you have understood the process and have discussed the potential of live liver donation with family and friends and feel ready to proceed, you can:
- Get in touch via email or telephone and complete a donor health questionnaire.
- Check your blood group using an Eldon Kit.
- Check you BMI, you can get a print out of your BMI at many large pharmacy stores, this can be sent in with your donor health questionnaire.
Leeds Live Donor Liver Transplant Program
Please follow the link below to visit our webpage
- Eldon Kits can be obtained from shops such as Amazon.