Your doctor has recommended for you to undergo Image-Guided Lung Tumour Ablation. This leaflet will explain what the operation involves, the outcomes and the possible risks.
What is an image-guided lung tumour ablation?
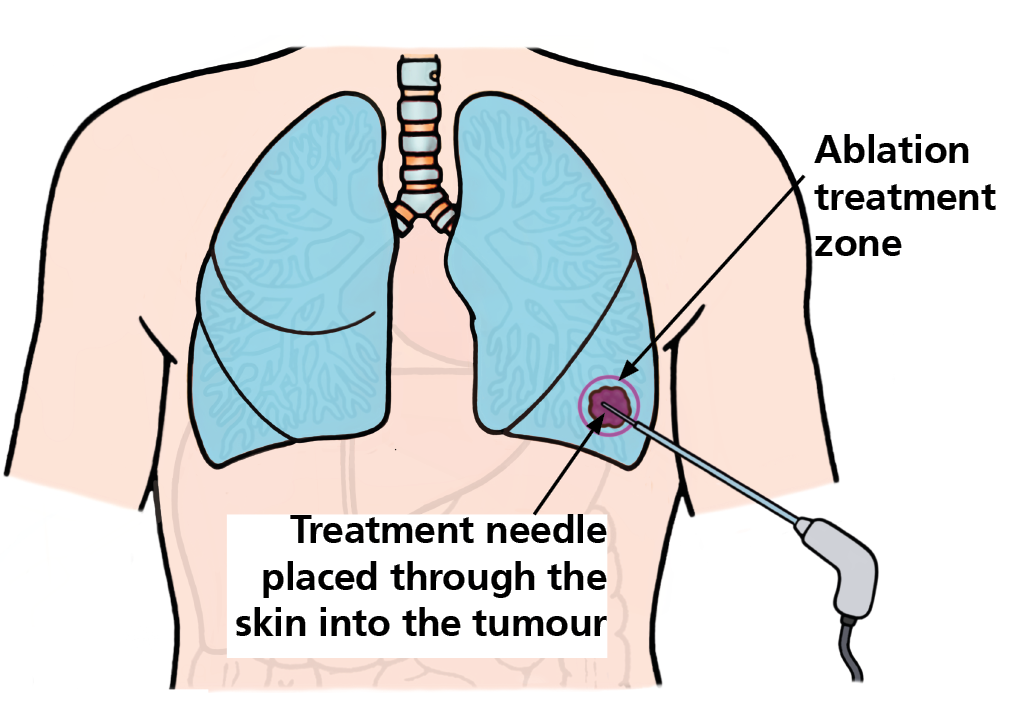
Image-guided ablation is a method of treating cancers within the lungs without conventional surgery. It allows one or more cancers to be treated with minimal injury to the remainder of the lungs.
How is an image-guided lung tumour ablation performed?
This operation is performed in the CT room under a general anaesthetic.
Using CT and X-ray imaging, special needles are placed into the cancer. The number of needles required is determined by the size of the cancer.
Anaesthetic
This operation is carried out under a general anaesthetic. Your fitness for a general anaesthetic will be assessed in the Pre-assessment clinic.
Operation
Once you are asleep, the interventional radiologist will use CT imaging for guidance, pass a special needle through a small puncture in the skin and position it within the cancer.
The needle is attached to a generator which delivers the energy, either heat or electrical, to destroy the cancer. The actual operation takes about 30-40 minutes but the whole operation may take 2-3 hrs. This time may vary depending on how many needle placements are required.
Consent
You will meet the interventional radiologist in the Interventional oncology clinic to discuss image-guided lung tumour ablation. The operating interventional radiologist will explain this to you in more detail, along with the risks and intended benefits before you provide your permission to proceed with the operation via a signed consent form.
What are the risks?
Serious complications are uncommon. Each individual has their own risk factors that will be discussed during your first appointment.
The anaesthetist will discuss with you the risks of having a general anaesthetic for this operation.
Common risks
- It is common for a little air to leak into the space around the lung during the treatment. This may cause the lung to partially deflate, this is called a pneumothorax. This occurs in one out of two treatments and usually whilst you are asleep.
- Occasionally the lung can develop a slow leak which may take several hours to become apparent. This usually requires treatment, which involves putting in a small tube called a chest drain that will stay in overnight. The following morning, a chest x-ray will be performed and if the pneumothorax has reduced, the chest drain will be removed.
- It is not unusual to develop flu like symptom known as ‘post-ablation syndrome’ in the days following the ablation which is related to the death of the cancer cells.
- It is common to produce a small amount of blood-stained sputum after the procedure. Finding blood in your sputum may be worrying for you but this will normally settle after a few days and is very rarely serious.
Less common but serious risks
- The risk of more serious complications is about or 2 in 100 treatments. Sometimes, a persistent puncture of the lung can develop which may require the drain to remain in place longer or very rarely a small operation to treat the problem.
- Infection following ablation is a rare but may be a serious complication. If you develop coloured sputum or a temperature this may be evidence of a developing infection which will require treatment.
- Rarely more serious injuries or death may result from the treatment. The risk of such a complication is estimated to be about 1% or 1 in 100 treatments.
Are there alternative investigations / treatments?
The alternative treatments to ablation may include observation, surgery, and focused radiotherapy.
There are many factors which favour different treatments including the number, size and position of cancers and your level of general fitness.
The risks and benefits of the different treatments would have been considered by your cancer specialist before referring you for an ablation, and we will review these alternative options with you when you meet our team.
How well does it work?
In general, ablation is most likely to be successful if the cancers are smaller (< 3 cm) and limited in number (three or less). The National Institute of Clinical Excellence (NICE) reviewed the results of this procedure (www.nice.org.uk). From 46 studies that included 1584 patients with a mixture of cancers, NICE demonstrated that on average, 59 for each 100 patients treated were alive 18 months after treatment.
In our centre, 95 out of each 100 tumours were successfully ablated in patients with secondary colon cancer. The overall survival of patients is 94% after 1 year, 69% after 3 years and 55% after 5 years.
What if the cancer grows back?
In a small number of cases, the cancer may not be successfully ablated. The treatment can be repeated, or your cancer specialist may suggest an alternative treatment.
What to expect from this operation?
Admission
You may be admitted the day before or the morning of your operation onto the thoracic ward. On the day, the ablation team will consist of:
- Consultant Interventional Radiologist
- Clinical Nurse Specialist (CNS)
- CT radiographers
- Consultant Anaesthetist
- Anaesthetic Operating Department Practitioner
Pre-operative preparation
You will attend the pre-assessment clinic for an anaesthetic assessment and investigations prior to the operation, which will include blood tests and ECG.
Pre-assessment will take your medical history and review your medication. They will advise you if you need to omit any of your medication on the day or prior to the operation.
If you are taking blood thinners, instructions to stop this medication may be given to you.
You will be assessed for Obstructive Sleep Apnoea (OSA). Sleep apnoea is when your breathing stops and starts when you sleep; this may require you to have further investigations. If you normally use CPAP at home, kindly bring the machine with you on your admission.
You will be assessed for Methicillin-resistant Staphylococcus aureus (MRSA) and you will be given an anti-microbial body/hair wash and nasal cream. This will be discussed during pre-assessment, and you will receive instructions on how to use them.
Carbapenemase-Producing Enterobacterales (CPE) are bacteria that usually live harmlessly in the gut of humans. You will be screened for this, which usually involves taking a rectal swab/stool sample.
You will receive a letter from the hospital with your admission date, ward, and instructions for fasting prior to the operation.
Recovery
After the treatment, when you wake up you may have a sore throat. This is caused by the breathing tube placed in your throat while you were asleep.
You will be transferred to theatre recovery where you will be monitored. Once you are stable you will be transferred to the ward. A chest x-ray will be performed a few hours after your operation or the next day.
Aftercare
Once back in the ward, the nursing staff will continue to monitor you regularly. IV fluids and pain relief will be administered as prescribed by the doctor.
Blood tests may be performed the morning after your operation to review your full blood count and renal function. Most patients are discharged in the next few days.
Care at Home
We would advise that someone is at home with you the first night after discharge. After your operation you may still experience pain or nausea, which can be managed by medications. Please see some of our recommendations below:
- Hydration: drink 2-3 litres of water a day. Adopt this as a lifelong habit as it helps to keep your kidneys healthy.
- Exercise: avoid lifting heavy items and other strenuous exercise for at least two weeks.
- Driving/travel: refrain from driving until you feel well again; it is your responsibility to ensure that you are fit to drive. You should not fly until you have been seen back in clinic — if you need to fly before this time, please contact our team by phone for advice.
- Medicines: you will be advised about restarting your medications before discharge. It is normal to experience mild pain and discomfort, continue your regular painkillers like paracetamol for the first week and reduce as pain decreases. If your pain persists and your painkillers are not working, please contact your GP to review your medications.
- Work: you should be able to return to work within 1-2 weeks, although some people may require a longer recovery period.
- Follow up: arrangements will be made for the Interventional Oncology CNS team to contact you after discharge via telephone to carry out remote follow up following your operation. You will also be invited to attend a follow-up scan between 4-6 weeks after your operation.
Contact information
We hope some of your questions have been answered by this leaflet. If there are any questions you would like to ask before you come for your operation, please get in touch.
Between 9am and 5pm, Monday to Friday:
Clinical Nurse Specialist
Between 9am and 5pm, Monday to Friday:
Interventional Oncology program co-ordinators
Outside 9am and 5pm, Monday to Friday:
Ward J84 at St James’ Hospital