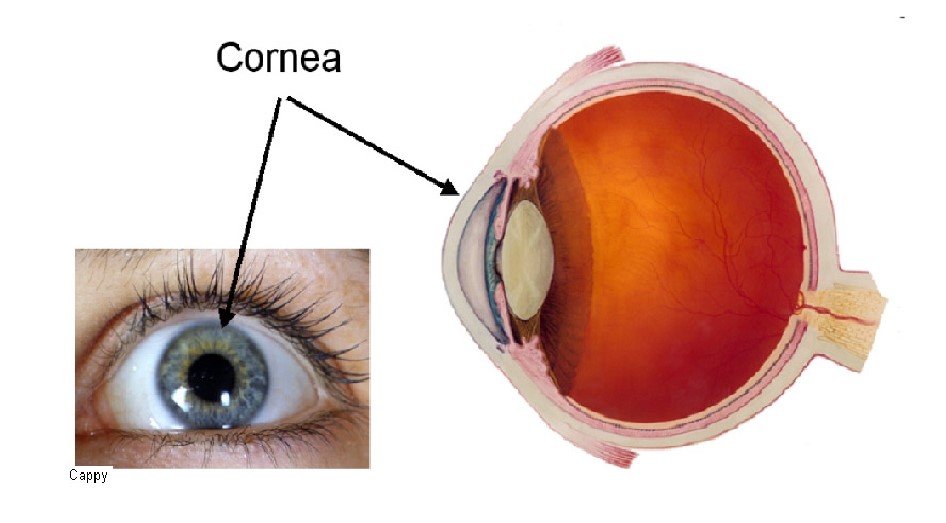
Cornea
The cornea is the clear dome-shaped window at the front of the eye.
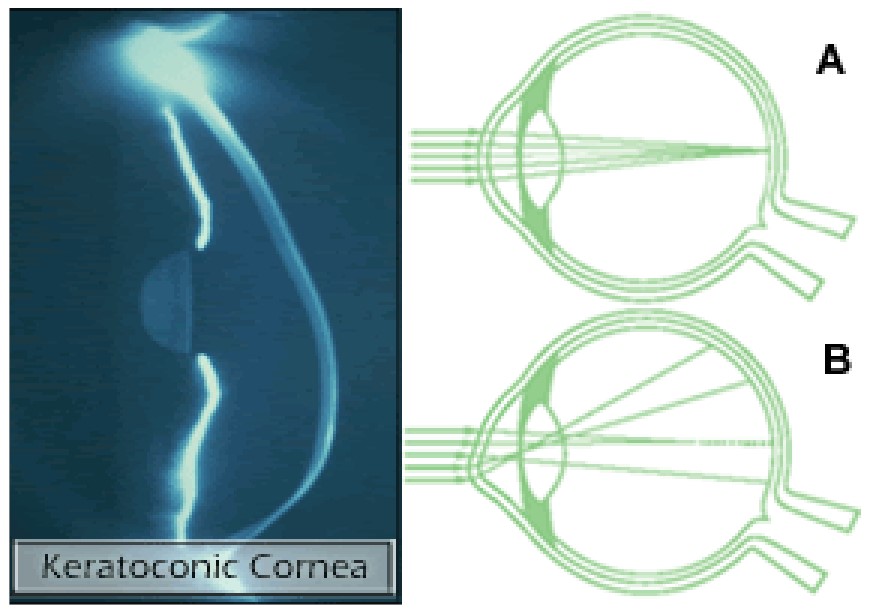
Keratoconus
Keratoconus is a genetically inherited disease (it is however only rarely found in other members of the same family) that effects the normal shape of the cornea. A healthy eye (fig. A) is more spherical in shape, allowing an image to come into focus clearly. The cornea of an eye with keratoconus (fig. B) bulges outward, creating a cone-like shape and distorted vision.
Keratoconus normally affects both eyes, although at differing points of onset and rates of progression. In most people keratoconus begins during their teenage years and progresses at varying rates until stabilising in the 30s or 40s. In the past up to 20% of all patients with keratoconus required a corneal transplant. This was either because of corneal scarring preventing useful vision, or because of intolerable side effects related to the use of contact lenses or spectacles.
There are now two new methods to treat keratoconus that are much less invasive than a corneal transplant: Keraring implants (which you can read about in the Keraring information leaflet) and Corneal cross-linking.
Cross-Linking
Corneal collagen cross-linking with riboflavin is a new treatment that increases the stiffness and rigidity of the cornea and stabilises keratoconus. Patients who previously had progressive keratoconus have now been treated and followed for over five years with 95% showing no progression of their condition.
Collagen cross-linking has been used in dentistry for many years. Prof. Theo Seiler and Prof. Eberhard Spoerl at the University of Dresden first developed cross-linking as a treatment for the conea in 1993. The first patients were treated in1998. Today corneal cross-linking is performed in more than 500 centres around the world. In many centres it is the standard treatment for keratoconus, reducing the need for a corneal transplant.
How does cross-linking work?
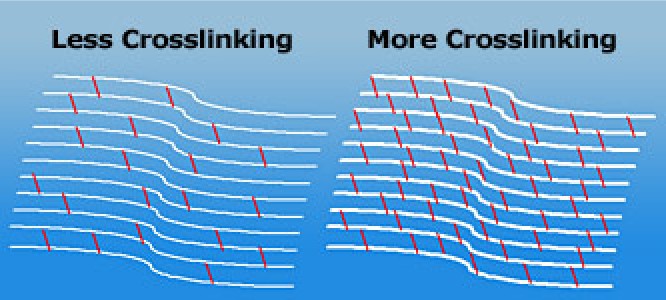
The bulk of the cornea is made from collagen fibres which are arranged in bundles. The strength and rigidity of the cornea is partly determined by how strongly the fibres are linked together. Over the course of a lifetime one’s cornea become progressively stiffer due to natural cross-linking between the fibres.
Riboflavin (vitamin B2) is a naturally occurring compound which strongly absorbs UV light. By applying riboflavin to the cornea at the same time as exposing it to a UV light source, the riboflavin enhances the cross-linking effect of the UV light.
How is Cross-Linking treatment applied?
The cross-linking treatment is carried out with topical anaesthesia (eye drops), which numb the surface of the eye. The patient feels no discomfort during the procedure.
The surface epithelial cell layer is removed from the central part of the cornea, and the riboflavin drops applied.
Once the riboflavin has penetrated into the cornea, the UV light is focussed onto the central area of the cornea for 10 minutes.
Riboflavin (vitamin B2) drops are instilled onto the cornea before and during the cross-linking procedure.

Ultraviolet light at 365 nm is used to activate the riboflavin within the cornea to induce cross-linking.
Finally a bandage soft contact lens is applied. The contact lens is worn for up to 2 weeks until the surface epithelial cell layer has re-grown. During the first few days the eye will be sore and watery.
We advise resting with both eyes shut for as much of the time as possible during the first 48 hrs after the operation. This will significantly improve your comfort in the initial period.
Eye drops will be given that are preventive against infection and inflammation. The use of the eye drops will be discussed with you before you leave the clinic.
You can return to work after 1 week, resume sports activities after approximately 2 weeks, and swimming and sauna after approximately 3 weeks.
You may drive a vehicle again only with the doctor’s permission, normally after the first week.
After the operation
In the first period (1-3 months) after cross-linking, you are much more sensitive to light (glare), and the vision is worse for a short time. Only once the cornea has become stable should you consider glasses or contact lenses for definitive correction of any residual spectacle error. Some people choose to seek temporary glasses or contact lenses during the recovery period. In general, a hard contact lens can be worn again after 1- 2 months.
Benefits of Cross-Linking
Cross-linking is effective in stabilising the progression of keratoconus in the majority of patients. Studies have shown that for about 95% of Keratoconus patients the cross-linking procedure prevents further vision loss.
In a minority of patients the treatment gives an additional small measure of benefit in reducing the corneal steepness and irregularity. This in turn means some reduction in the short-sightedness and astigmatism associated with keratoconus.
Risks of Cross-Linking
Potential complications of cross-linking are rare. They include corneal haze, corneal infection, corneal inflammation, corneal scarring, and the need for repeat surgery.
Is Cross-Linking suitable for all keratoconus patients?
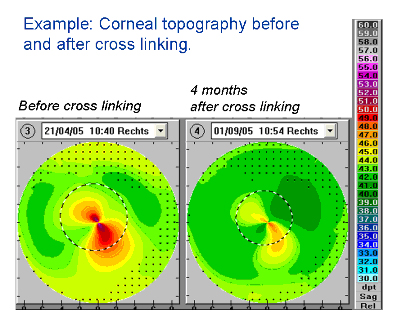
Cross-Linking is a relatively new treatment and its place in the treatment of keratoconus is still being defined. This will become more apparent as more people are treated around the world, and the results of these treatments are published. To date, the published literature suggests that cross-linking is most suitable for patients with progressive keratoconus. That means patients whose glasses or contact lens prescription is changing quite frequently, or whose vision is becoming worse despite using contact lenses, or whose corneal topography maps show clear progression of keratoconus.
Summary
Cross-linking strengthens the cornea and halts the progression of keratoconus and corneal ectasia. It may be used alone, or in conjunction with other treatments such as Keraring corneal implants or phakic intraocular lenses, to produce an improved outcome. When the cornea has stabilised, glasses or contact lenses are usually required to provide the best level of vision.
Back to top