Atopic Eczema
Atopic eczema (AE) is the commonest type of eczema. It is linked to the tendency to dry skin and a family (genetic) tendency to eczema, asthma or hay fever (atopy). It usually presents in the first year of life and rarely after the age of 5 years. Patients with AE are at higher risk of developing asthma, hay fever and/or an allergy.
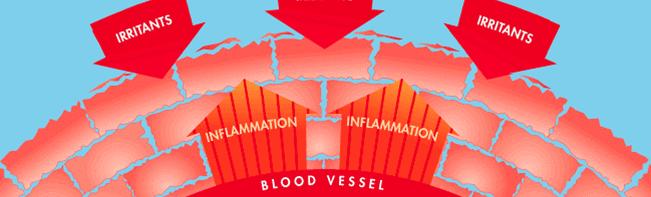
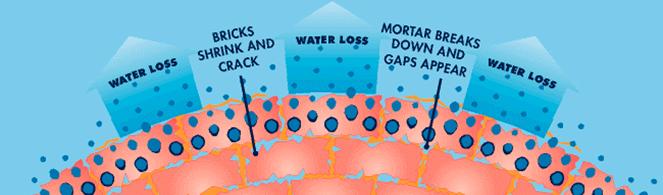
In patients with AE the skin is dry (like a brick wall where the mortar has dried out and weakened). This allows irritants, infections and allergens to penetrate the skin surface and trigger the body’s immune system. In AE the body’s immune system tends to over-react, forming increased levels of chemicals which trigger inflammation and a blood protein called Immunoglobulin type E (IgE). These result in inflammation (redness and weeping) and itching. Chronic scratching and rubbing leads to thickening of the skin with exaggerated skin creases, and raw/ broken areas.
Location of Eczema
AE can occur anywhere, however in babies it often involves the face and in children often the creases (elbows, wrists, backs of knees, and ankles) and in adults, the face, creases, and hands.
Things which trigger eczema to flare
There are five main factors that can trigger a flare of AE:
- Stresses
- Dry Skin
- Infection
- Irritants
- Allergies
1. Stress
Stressful triggers include tiredness, teething, illness and vaccination/immunisation, as well as day-to-day stresses at home and school. Even children and babies can be affected by stress and can also have worries of their own which you may not realise e.g. new baby in the home, new nursery etc.
2. Dry Skin
Most patients with eczema have an increased tendency to dry skin/water loss through the skin due to genetic changes which alter the skin surface layer. This varies from mild dryness (which may not be obvious) to severe dryness. The worse the dryness the more severe the tendency to eczema/inflammation (redness, weeping, swelling) tends to be.
Increased dryness increases skin itching and increases the risk of infection (made worse by scratching due to itching), reaction to irritants, and increases the risk for allergy development and reaction. Treatment and prevention of dryness is crucial in managing and preventing eczema (the equivalent to cleaning teeth to prevent tooth decay).
3. Infection
Any infection on the skin can trigger eczema to worsen however 3 infections are particularly common.
1. Impetigo-type bacteria – A bacterium called Staphylococcus (Staph) Aureus can be found on many people’s skin and sometimes in the nose. However, it can cause active infection, particularly in AE skin. If the skin is dry, flaky or cracked the bacteria can multiply and trigger inflammation in the skin making the eczema worse, producing a vicious cycle of flaring.
Signs of Staph infection (*see images: https://eczema.org)
- broken, weeping skin
- yellow crusts or / and pus-filled spots
- sore skin
- red and hot skin
Treatment & Prevention:
If the infected area is small antiseptics or antibiotics can be applied directly on to the skin (topically). Sometimes they may be added into other topical treatments e.g. steroids and moisturisers. Antibiotics may be required if the infection is spreading despite topical therapy or the child is unwell. A skin swab is often taken before treatment is started.
Staph Aureus can sometimes live in the skin lining the nose. In patients getting recurrent infection, a nasal swab is often taken and if found an antibiotic nasal ointment is prescribed.
Antiseptic bath or shower gels together with soap substitutes help to prevent the risk of infection by reducing the number of living bacteria on the skin. Antibacterial ointments can also be applied to broken/cracked skin to help prevent infection.
2. Herpes Simplex (cold sore) viral infection (*see images: https://eczema.org)
A third of the population get recurrent cold sores. These are due to a viral infection called Herpes Simplex type I. If this virus gets onto skin prone to eczema (or worse where eczema is active), it tends to spread quickly, sometimes extensively to cause a much more severe infection than normal and can heal with scarring. It can even spread into the eye.
Contact with active/ healing cold sores should be avoided and if infection is suspected you should seek urgent medical attention. Once patients have had infection once, it has a tendency to recur at times of stress, illness, sun, and in those with low vitamin D or iron levels.
Signs of infection:
Painful small blisters often around the mouth, face, and neck (occasionally fingers or other sites) spreading to other areas of the body. Blisters may be oozy and quickly crust.
Treatment: Antiviral medicine or tablets. If infection is widespread, patients are often admitted to hospital for treatment. Infections around or involving the eye should be seen by an Eye Specialist.
3. Candida (Thrush) fungal infection
Candida is a yeast that tends to live on the skin in the moist skin folds e.g., groins, nappy area, around the mouth in children who dribble or suck dummies etc. The infection can trigger / worsen eczema.
Signs of infection:
Infection tends to make the skin very red, shiny and sore and occasionally little pussy spots are seen. Occasionally infants may also have mouth soreness due to Candida.
Treatment: Antifungal cream or drops for the mouth.
4. Irritants
Common irritants include:
- Any factor which dries the skin e.g. over washing, detergents, sustained central heating, cold weather etc.
- Heat – hot weather, hot bath/shower etc.
- Body secretions – nasal (e.g. with colds/coughs), sweat, urine, stool/poo (wet / dirty nappies).
- Contact irritants – include preservative chemicals added to all cream products including moisturisers, steroids, and sun-creams (which can cause stinging when applied to more active eczema), wool/rough materials, detergents, sand.
5. Allergies
Not all patients with AE have an allergy. However allergies are more common in atopic patients and can cause eczema to flare. Allergies can be due to proteins reaching the skin via the air, by direct contact, or in the diet.
There are three groups of allergens
Dietary / Food
Most Common food allergens:
Milk (dairy products), Eggs, Fish, Wheat, Soya, Nuts.
Also – Pulses (peas, lentils), sesame, kiwi.
Many children with AE do not have a food allergy, however food allergy can be a factor in some children and is more common in children with more severe eczema and in families with allergies.
Food allergy is suspected if:
- There is a history of reacting on the skin to a food (urticarial/red blotchy, itchy or swollen rash or swelling).
- Other symptoms such as recurrent vomiting, tummy upset or diarrhoea, wheezing or breathing change after a food.
- Eczema is very severe, widespread, red and itchy and not responding to treatment.
If food allergy is suspected further tests can be carried out under the supervision of a Paediatric Allergist and dietary advice from a paediatric dietician.
2. Airborne allergies
- Animals – House dust mite, cat, dog, horse etc.
- Plants – Grass and tree pollen – this can cause eczema to flare over the hay fever season.
- Moulds.
Airborne allergy is suspected if:
- There is a history of reacting on the skin to the allergen e.g. if licked or touched by an animal or skin flare with dust exposure.
- Eczema involves exposed areas of skin (face particularly around the eyes/neck/forearms).
- Eczema is seasonal (e.g. summer months with pollen allergy).
3. Contact allergies
Everyday products (even hypoallergenic) that come in contact with the skin can sometimes trigger allergy e.g. metals in jewellery, fragrances, dyes, preservative chemicals in skin products and baby wipes etc. Be aware that some contact allergy is due to aerosolized allergen e.g., paint fumes/fragrance sprays.
If contact allergy is suspected then contact allergy (patch tests) can be arranged in the hospital dermatology department.
Contact allergy is suspected if:
- There is a history of reacting on the skin to the allergen e.g. fragrance product, footwear or clothing, dyes, under metal objects e.g. jewellery/buckle.
- The pattern of eczema is unusual.
- Eczema is not responding as expected to standard treatments.
Treatment
1. Moisturisers / Emollients
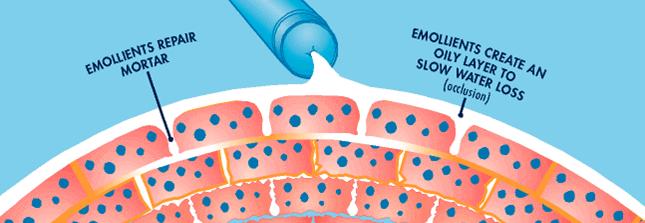
Moisturisers are the first-line treatment for eczema and also help to prevent eczema from flaring. They act as a protective barrier against infection, irritants and allergens. It is essential to apply regular moisturiser often enough and in sufficient amount to clear all dryness. For most patients this is at least twice daily, more often if the skin is still dry. Regular moisturising for skin prone to dryness/eczema is the equivalent of cleaning teeth and should be continued even when eczema is clear.
Emollients can be ointments, creams or preparations to wash with. Frequent bathing, detergents and shampoos can worsen dryness and eczema and should be avoided where possible.
Quantity of Emollient to be used per week
| Amount (g) | |
|---|---|
| Infant | 125-250 |
| Small Child | 250-500 |
| Large Child | 500+ |
Ointments
Ointments are the best for moisturising dry skin and less likely to sting/irritate eczematous skin. Ointments are preferred for very dry or cracked skin and during a significant flare.
During hot weather, or if used excessively, ointments can block pores and lead to blocked and irritated hair follicles (folliculitis) and especially in hot or humid conditions increased itching and skin heat. If this occurs stop greasy preparations temporarily and consider switching to creams and seek advice if necessary.
Note:
There is a fire risk with all emollients (paraffin and non-paraffin based). Emollients on clothing, soft furnishings, bedding etc. makes them all more flammable. Avoid exposure of any of these with naked flames such as cigarettes, vaping devices, candles, open fires, gas cookers, matches etc due to increased fisk of fire or burns!
Creams
Creams are white, water based and lighter than ointments. They tend to be less moisturising than ointments. Due to their water content preservative chemicals are added to stop them growing bacteria/moulds and prolong the shelf-life. Preservatives may sting and aggravate when applied especially to more active eczema, and occasionally cause contact allergy. We therefore tend to avoid creams when skin is very dry/cracked and if eczema is moderate or severe.
However, creams are less likely to block pores and cause folliculitis or in acne prone sites/ages acne. These are therefore preferable for eczema skin that is well moisturised, clear or with mild eczema, in acne prone areas or in hot or humid weather. They are also cosmetically nicer to use so are good for daytime moisturisation provided dryness or eczema is not as severe.
How to apply emollient
- If the emollient is in a tub rather than a pump dispenser, use a clean spoon to scoop out (rather than your fingers), to reduce the risk of transferring skin bacteria into the emollient.
- Apply directly onto the skin and smooth gently into the skin in the same direction that the hair grows (avoid rubbing). This helps reduce hair follicles becoming blocked. If the bottle/ tub doesn’t have a pump dispenser, use a spoon to decant out (avoid putting fingers into pots as this can increase the risk of contamination with microorganisms and act as a source of infection). Obtain new supplies of open pots of topical medications after treatment for infected atopic eczema.
- Use emollients with other topical treatments as advised. We tend to recommend using any steroid/anti-inflammatory topical first and wait a few minutes before applying the emollient.
- Consider providing your child’s nursery or school with a supply.
- It may be preferable to have more than one type to use on different areas (e.g., one for face, another for body) or at different times depending on the severity of eczema (e.g., lighter product when clear/no dryness and thicker greasier preparation when skin very dry/ inflamed). Non-prescribed emollients should be fragrance-free.
Emollients for washing
- Use an emollient as a soap substitute for hand washing, showering or added to bath water as standard soaps and shower gels can be irritating to the skin.
- To apply as a soap, mix a teaspoonful in the palm of your hand with a little warm water and spread over damp or dry skin. They do not foam like a conventional soap but are just as effective at cleaning the skin. Rinse and pat the skin dry, being careful not to rub. An emollient with antiseptic may be given for those prone to recurrent skin infection.
- For shampooing hair, in children under 1 year use an emollient instead of shampoo. Older children can use a non-perfumed brand of shampoo, ideally labelled as suitable for eczema, and avoid washing hair in bath water.
- Bath emollients are no longer routinely prescribed / given on prescription.
Remember – Children with emollients are very slippery when wet!
2. Topical Cortico-Steroids (TCS)
Although moisturisers are the first-line treatment for eczema, TCS are necessary to treat acutely inflamed or highly itchy areas of skin. They should always be used with moisturisers and not instead of. When used correctly and monitored by a medical or nursing professional, TCS are safe to use and usually very effective.
When and where to use steroids
TCS should ideally be used where eczema is active, even if the skin is broken or cracked, however they should be avoided where there is no eczema or if there is untreated infection (e.g., see impetigo or cold sore infection previously).
How to use steroids
See the Finger Tip Unit guide for quantity use. TCS should be applied before a moisturiser to avoid the moisturiser acting as a barrier preventing the steroid being absorbed into the skin. When applying moisturiser avoid spreading steroid onto healthy areas of skin. TCS should be measured to a ‘Finger-tip unit’ and into the skin in the direction of hair to reduce the risk of folliculitis.
Finger-Tip Unit Guide for steroids
For one finger-tip unit (FTU) – Squeeze the steroid from the end of your index finger to the first crease of your (adult) hand. This amount should be used to treat an area of eczema 2x the size of the same (adult) hand.

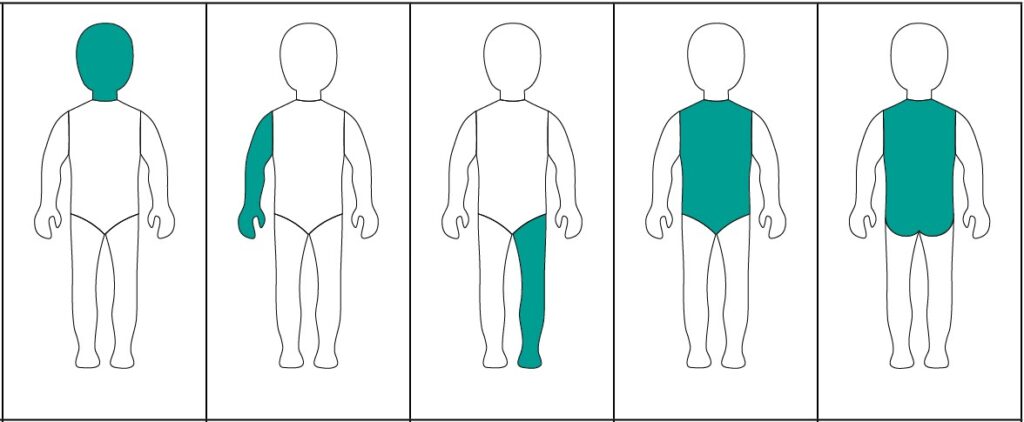
Face & Neck | Arm & Hand | Leg & Foot | Trunk (Front) | Trunk (Back) inc Buttocks |
|---|
| AGE | NUMBER OF FTUs | ||||
|---|---|---|---|---|---|
| 3-6 mth | 1 | 1 | 1½ | 1 | 1½ |
| 1-2 yr | 1½ | 1½ | 2 | 2 | 3 |
| 3-5 yr | 1½ | 2 | 3 | 3 | 3½ |
| 6-10 yr | 2 | 2½ | 4½ | 3½ | 5 |
The diagrams show how many adult FTUs of steroid (cream or ointment) are required to cover each area of the child’s body.
Which steroid to use: You will be advised of a care plan for using steroids. When eczema is active steroids are often recommended 1-2 times daily for 1 to 2 weeks, however they may be recommended for longer if eczema is more severe, although we often recommended tailing off how often they should be applied or tailing off from a stronger to a weaker steroid. Use of dressings or garments over the top of strong steroids should only be done following specific dermatology advice as they increase the amount being absorbed in to the skin.
For the face and other delicate sites: Usually only mild steroids are recommended. Occasionally if eczema is more severe, a moderate strength steroid is recommended for a short period of time, reducing to a mild steroid as the eczema improves. It is very rare for strong (potent) steroids to be recommended for the face even for short periods. They should usually be avoided due to the risk of skin thinning and also of cataract if used near to the eye. In general avoid using anything other than very mild steroids near the eye or on the eyelids.
For the body: The steroid strength used will depend on eczema severity. Your doctor/nurse will recommend which should be used. In general ointments are preferable to creams (for the same reason that ointment moisturisers are usually preferable to creams). Some steroids have extra ingredients added, e.g. antiseptics, antibiotics or antifungal treatments which may be recommended if infection is suspected along with eczema. Continue treatment until eczema clears to reduce the risk of the eczema returning quickly and to ensure that symptoms like itching or soreness settle adequately. There are some tape/dressing preparations which contain steroids that can be prescribed to local areas of persistent eczema.
Topical Steroid Withdrawal (TSW)
When used correctly, TCS are safe and effective. TWS has been reported very infrequently with prolonged use of strong TCS (particularly if used to the face or genital areas) and most people using TCS do not get TSW. Concern regarding the potential risk of TSW may lead to under treatment of AE. If eczema comes back weeks after stopping TCS it is not TSW.
In TSW eczema never clears up with appropriate amounts of strong steroid, the skin is redder/darker, more ‘burning’/sore than the original eczema often with severe itch, weepy/oozing areas, affects different areas of skin, may be associated with swelling (eyelids, hands, ankles) and the child may feel physically ill.
Available Topical Steroids
3. Topical Calcineurin Inhibitors (TCI)
TCIs are topical treatments applied to the skin, which work like steroids to reduce inflammation (redness/soreness/itching).
They are used similarly to steroids, once or twice a day where eczema is active which may include broken skin. However, unlike steroids there is no risk of skin thinning (atrophy) or if used in the eye area of cataract, therefore they are often recommended for delicate sites like the face and creases, particularly in children requiring long-term or frequent use of even mild topical corticosteroids.
Like TCS, TCI should be avoided on infected skin and should also be avoided under garments/bandages without specialist advice. It is also important to avoid sunburn/damage when using these treatments.
It is quite common to get some contact stinging or sometimes a burning sensation when used on eczema skin particularly when more inflamed or cracked/broken. As eczema improves this often reduces. Therefore we usually recommend calming the eczema initially with TCS before adding in a TCI which reduces this risk. If stinging/irritation is significant seek advice from your Health Care Professional (HCP).
Two TCIs are currently licensed for use in children: Pimecrolimus (Elidel®) 1% cream, licensed from 3 months of age, and Tacrolimus (Protopic®) ointment, 0.03% licensed from 2-16 years and 0.1% above 16 years.
For anyone prescribed TCI we advise reading the more detailed British Association of Dermatologists (B.A.D.) information sheet available on their website.
https://www.bad.org.uk
4. Topical Anti-Microbials (no steroid)
- Topical antibiotics – Bacitracin, Neomycin, Metronidazole
- Topical antifungals – Clotrimazole, Nystatin, Terbinafine
- Topical antiseptics – Clioquinol, Zinc
5. Scalp preparations
- Shampoos
Descaling: Capasal, Alphosyl 2in1, Polytar, T Gel
Antifungal/Antidandruff: Nizoral / Ketoconazole - Steroid preparations – see steroid table
- Non-steroid Scalp Preparations
Descaling: Sebco, Cocois, Tar Pomade, SCC ointment
6. Dressings and Bandages
Whole-body (limbs and trunk) occlusive dressings (including wet wraps) with TCS should only be used to treat eczema in children for 7-14 days (or for longer with specialist dermatological advice), but can be continued with emollients alone until eczema is clear.
A trained nurse will usually advise and/or demonstrate how these should be used.
Dressings: Duoderm® or similar dressings can be helpful to use over persistent small areas of eczema (provided there is no reaction to the sticky adhesive on the back of the dressing). TCS may be recommended beneath but only on advice from an appropriate HCP.
Bandages: Can be useful and prescribed for persistent eczema on arms/legs. Examples include zinc containing bandages such as Zipzoc stocking and Zincoband or another anti-inflammatory called icthammol (Icthopaste). Some will need to be held in place with a secondary bandage to stop them falling down/off.
7. Complimentary Therapies for Eczema
The effectiveness and safety of complementary therapies such as homeopathy, herbal medicine, food supplements for the management of atopic eczema have not yet been adequately assessed in studies.
If you are using or intend to use this type of treatment for your child’s eczema inform their healthcare professional.
- Caution is recommended with use of herbal medicines. Be wary of herbal products not labelled in English or that do not come with information on safe usage (see the Medicines Health Regulation Authority (MHRA) using herbal medicines: advice to consumers).
- Topical corticosteroids are deliberately added to some herbal products intended for use in eczema.
- Liver toxicity has been associated with the use of some Chinese herbal medicines used to treat eczema.
If you are using or intend to use this type of treatment for your child’s eczema inform their healthcare professional. If you do plan to use complimentary therapies, keep using emollients as well.
8. Treatment for very severe or chronic eczema
Photo (light) therapy or systemic treatments are used to treatment severe atopic eczema in children when other management options have failed or are inappropriate and where there is a significant negative impact on quality of life. Treatment should be undertaken only under specialist dermatological supervision.
Phototherapy
Phototherapy involves the use of artificial light treatment, usually UVB.
Treatment can usually only be given in hospital dermatology departments and is usually given 3 x per week on separated days. It is usually avoided in young (pre-school) children and those with very fair skin, but can be very effective in improving eczema, particularly for children who have naturally darker skin types.
Separate specific information is available on this and should be given and read through for any patient in whom this is considered /recommended.
Systemic Treatments for Eczema
There are a number of treatments recommended or licensed for use in eczema which is more severe/widespread and resistant to standard treatments.
These include:
- Oral Steroids – short course (syrup/tablet)
- Immune suppressant oral treatment (syrup/tablet) which broadly suppresses / reduces the immune system and therefore inflammation in eczema e.g., Methotrexate (also available as injections), Ciclosporin, Azathioprine and others.
- Biologic treatments targeted immune suppression. These target and block specific inflammatory pathways known to be significantly increased in eczema and are more specific and less generally immune suppressive. Several different treatments both injections under the skin / sub-cutaneous or in tablet form are now licensed some from the age of 6 months up e.g., Dupilumab, others in adolescents e.g., Upadacitinib, Abrocitinib, Tralokinumab, Lebrikizumab.
Separate specific information is available on these and should be given and read through for any patient in whom this is considered / recommended. Most require monitoring blood or other tests.
Live vaccines should be avoided in children on immune suppressive treatments. Further information on vaccines in this situation is available from the British Association of Dermatology website.
Handy Hints
Clothing
- Try to wear cotton clothes if possible. Nylon and man-made fabrics can increase sweating and wool itching.
- Use non-biological washing powders without conditioners.
- Occasionally use biological washing powder on a hot rinse when empty to remove grease from your washing machine.
Environment
- Avoid heat as this increases itching. Central heating can increase skin dryness due to the lack of humidity.
- Use a high factor sunscreen for sensitive skin.
- Keep the bedroom cool to minimise itch. Use cotton sheets and blankets rather than quilts.
Scratching
- File/cut nails regularly to keep short and cover hands with gloves/mittens overnight to reduce damage done by scratching.
- Gently squeeze or pinch to relieve itchy skin.
Avoid fragranced products
- Try new products first with a small patch on the arm, wait for 2-3 days to ensure no reaction.
Swimming
- Avoid if eczema is very active or if the skin shows signs of infection. Afterwards, shower to remove chlorine, pat dry and apply moisturiser
Other useful websites:
British Association of Dermatologists Patient Information Leaflets (multiple different leaflets relating to eczema, treatments, vaccination advice etc.)
British Association of Dermatologists Eczema Care Online Organization UK National Eczema Society The Primary Care Dermatology SocietyThe last section of this information can be filled out in the physical copy of the leaflet (pages 26-30) by a consultant, to view what this section looks like please use the PDF link at the top of this page.
Back to top