What is a mechanical thrombectomy?
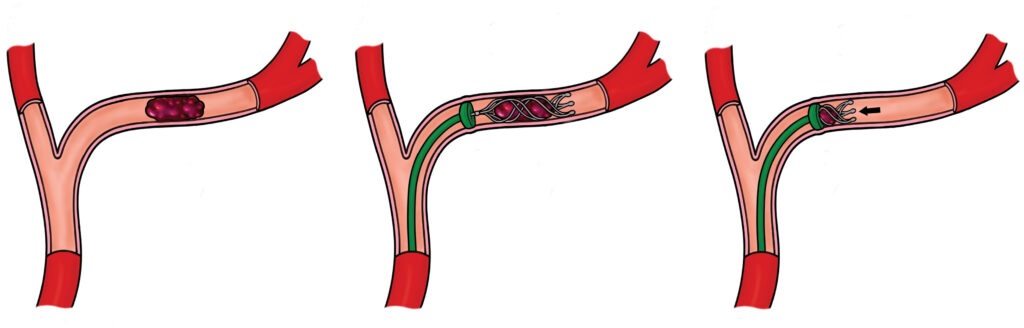
Illustration 1 (Image on the left): A cross-section of an artery showing a dark red blood clot lodged inside, blocking blood flow. The artery walls are intact, and the surrounding tissue is shaded to indicate restricted circulation.
Illustration 2 (Image in the centre): A catheter is inserted into the artery, reaching the site of the clot. A stent retriever is deployed through the catheter, expanding within the clot to capture it. The artery remains partially blocked, with the device in place.
Illustration 3 (Image on the right): The stent retriever is withdrawn along with the clot, clearing the artery. Blood flow is visibly restored, with the artery lumen open and unobstructed. The catheter is still partially visible, exiting the artery.
You or your relative has had a stroke and the medical team have decided the best treatment is to remove the clot directly from the blocked blood vessel. This is called a mechanical thrombectomy.
It is an operation used to remove a blood clot from the vessels in the brain using x-rays to navigate the tools needed to do this.
A stroke is a life-threatening medical condition that happens when either a blood vessel in the brain becomes blocked usually by a clot (ischaemic) or bursts (haemorrhagic).
You or your relative has had an ischaemic stroke. With this type of stroke if the blood flow is not restored quickly permeant brain damage will be caused which can lead to serious disability or in some cases death.
How do I prepare?
There is no specific preparation as this is an emergency procedure and is normally completed in your best interest. Mechanical thrombectomy has shown through studies the benefit in 1 of 2 patients, which is the highest than any intervention can offer. No other alternative matches it.
How is it performed?
Consent
This procedure is time critical where possible the Neuro-radiologist will meet you to discuss the procedure in more detail, the risks and answer any of your questions to your satisfaction before you provide your permission and sign your consent form.
If you are unable to consent, then the doctor will proceed in your best interest, often after discussion with your family.
Anaesthetic
A thrombectomy can be performed under both general or local anaesthetic. It is normal to be agitated during a stroke therefore the doctor may decide it is best to have a general anaesthetic during the operation to prevent any movement as this poses a risk of bursting a healthy blood vessel and causing a bleed in the brain.
If your doctor decides it is safe to do your thrombectomy under local anaesthetic you will be awake however an anaesthetist will remain present in case a general anaesthetic becomes necessary. Local anaesthetic will be injected into the groin area to numb it before access is gained.
Operation
The radiologist will gain access to the blood vessels through the artery in the groin (femoral). If the operation is done whilst you are awake, local anaesthetic will be injected in to the skin to numb it first. A small incision is then made in the skin followed by a needle into the blood vessel through which a wire is introduced to guide the sheath into place (small thin tube similar to a cannula).
The radiologist will then pass a thin catheter and wire into the blood vessels and navigate through the body and into the blood vessels in the brain.
X-rays will be used to help the radiologist guide the catheter and wire to the blocked blood vessel. A special x-ray die (contrast) will be used to make the blood vessels visible on x-ray. A micro catheter will be inserted up to the blocked part of the blood vessel through which a small stent will be pushed into the clot and opened up (this is called a stent retriever). The stent is left insitu for a few minutes to allow the clot to become embedded in the mesh. The stent is then pulled back into the catheter at the same time suction is used to prevent any small bits of clot travelling further down the blood vessel and causing another blockage.
If the clot is successfully removed the first time this is the end of the procedure. If the clot has not been removed the same steps will be repeated these are known as passes.
The doctor will repeat this process until either the clot is removed or it becomes unsafe to continue, unfortunately it is not always possible to remove the clot in some people.
Staff involved
Interventional Radiology (IR) procedures are performed by a multidisciplinary team. The team includes the following key staff:
- Interventional Radiologist (Consultant/Fellow): A doctor specially trained in minimally invasive, image-guided techniques who performs the procedure.
- Radiology Nurses: Highly trained nurses who care for the patient before, during, and after the procedure. They assist with sedation, monitor vital signs (heart rate, breathing, oxygen levels), and may “scrub in” to assist the radiologist directly.
- Radiographers: Experts in imaging equipment who operate the machines to provide real-time guidance for the doctor.
- Senior Clinical Support Workers (SCSWs): Assist with the setup of the room, patient positioning, and maintenance of sterile conditions.
What are the risks?
This is overall a safe procedure, although with any procedures, this carries the following risks:
- Complications as a result of the anaesthetic.
- Injection of air into the blood vessels.
- Bleeding from or damage to the artery in the groin which may result in a surgical operation to be repaired.
- The brain may swell as a result of the restored blood flow which could lead to a surgical operation to relieve pressure on the brain.
- Bleeding into the brain as a result of the restored blood flow through vessels which have been damaged; complications can vary from no symptoms to worsening of stroke symptoms or even death.
- Allergic reaction to contrast dye (mild symptoms like nausea, itchiness and rashes occur in 3%; moderate to severe symptoms such as severe vomiting, bronchospasm occur in less than 1%; risk of death is rare, estimated at 1:170,000).
- X-rays will be used to make images of your body and guide your doctor during the procedure. X-rays are a type of radiation. We are all exposed to low levels of natural radiation as part of our everyday lives and medical x-rays give an extra dose of radiation. Radiation can increase your chances of developing cancer many years or decades after the exposure. The chances of this happening to you as a result of this procedure are considered to be very low.
- In some very rare situations, you might experience some hair loss or some reddening of the skin in the area that was treated. If this happens, you should contact your clinical team who will be able to give some advice on the simple steps you can take to look after your skin.
- It is important to remember that your doctor thinks that the benefits of this procedure outweigh any risks from the radiation. We will make sure that the amount of radiation used in your procedure is as low as possible.
What else to expect from this operation?
Admission
If you experience a stroke, you will usually arrive at the hospital by ambulance or by attending A&E.
If you come directly to Leeds General Infirmary (LGI), you will be admitted to the hyper acute stroke ward (L21/L21S), where your rehabilitation will begin. If you were transferred to LGI from another hospital for a thrombectomy, you may return to that hospital afterwards to continue your rehabilitation, or you may remain at LGI and be admitted to the stroke ward here.
Recovery
Once the procedure is completed, the anaesthetist will wake you up whilst you are still in Radiology Theatres. You will be transferred to the recovery area in main theatres once it is safe to do so. Regular neurological examinations will be carried out to ensure you have not experienced any complications. This will involve asking you simple questions, testing the strength of your arms and legs and shining a light into your eyes.
Your blood pressure, heart rate and oxygen levels will also be monitored. The nurse will check the small wound in your groin for any bleeding.
If you have your thrombectomy under local anaesthetic you may still be transferred to the main recovery area for close monitoring and wait there until a bed becomes available on the stroke ward or while transport is arranged to transfer you back to your local hospital. Alternatively, you may be transferred immediately to the stroke ward or back to your local hospital following your operation.
Aftercare
Immediately after your operation, you will be required to have a period of bed rest to prevent the artery in your groin from bleeding. Your doctor may use a small plug to close the hole in the artery this is called a closure device, if this is used you will be able to sit up straight away.
Your doctor may request that you have bed rest for at least one night following your stroke. Depending on the severity of disability your stroke has caused it may not be possible for you to get out of bed the following day.
You will be assessed by the stroke doctor and multidisciplinary team as part of your rehabilitation.
Contact information
We hope some of your questions have been answered by this leaflet. If there are any questions you would like to ask before you come for your operation, please get in touch.