Key-hole approach to repair the mitral heart valve (without open heart surgery)
What is mitral valve disease?
You have been diagnosed with mitral valve disease by your doctor.
This information will help you to understand your condition, and the treatment options available, in particular a keyhole heart valve repair procedure known as TEER (transcatheter edge-to-edge repair).
We also hope that this information is useful for your family and/or carers to understand your condition so that they can support you before and after any procedures that take place. It will also explain some of the aims, benefits, risks and alternatives to this procedure and your choices so that you can be involved in making any decisions.
Mitral valve problems can either involve narrowing of the valve (mitral stenosis) or leaking of the valve (mitral regurgitation). You have been diagnosed with mitral regurgitation.
Mitral regurgitation can either be due to degeneration of the valve itself, secondary to infection of the valve, or due to enlargement of the heart chambers.
The mitral valve is a complicated structure and often combinations of problems contribute to the leak.
If a valve leaks, the heart must work harder to accommodate, so the work for the ventricle (pumping chamber) increases. As a result, the chambers of the heart enlarge and over time the heart muscle weakens. This affects your overall health and may stop you from taking part in your normal daily activities. Without treatment, mitral regurgitation can be a very serious, even life-threatening condition, leading to heart failure and risk of sudden cardiac death.
Signs and symptoms of mitral valve problems
Back to topHow the heart works
A normal heart has four chambers. The upper two chambers are the right and left atria. The lower two chambers are the right and left ventricles. The heart’s job is to supply the body with oxygen-rich blood. Blood is pumped through the four chambers with the help of four heart valves; the tricuspid, pulmonary, mitral and aortic valves.
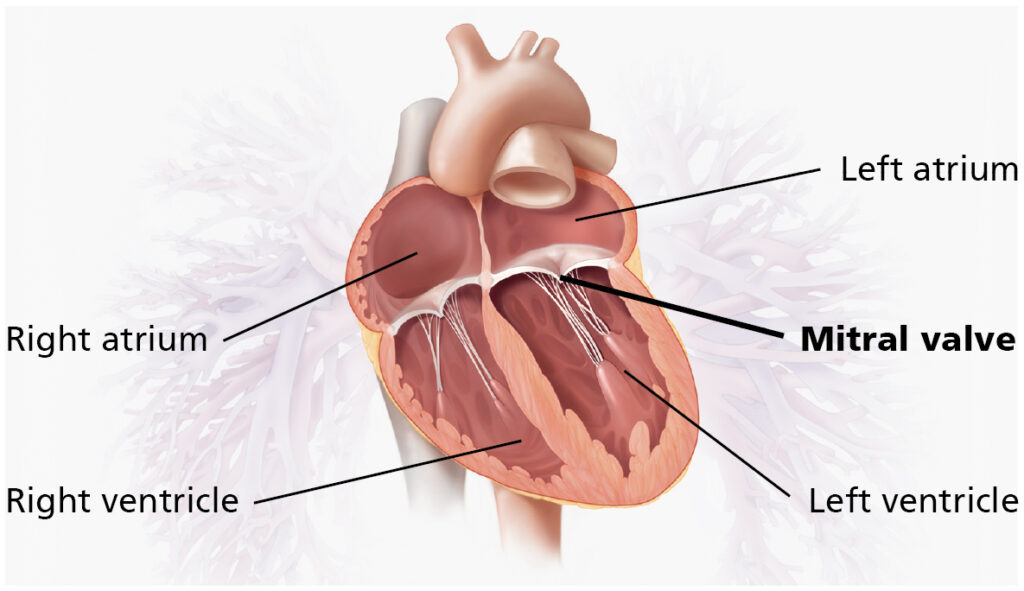
The mitral valve separates the upper left heart chamber (left atrium) from the lower left heart chamber (left ventricle). The mitral valve has two flaps, called leaflets. The leaflets open to let the blood flow into the left ventricle, and close to stop blood flowing backwards to the left atrium.
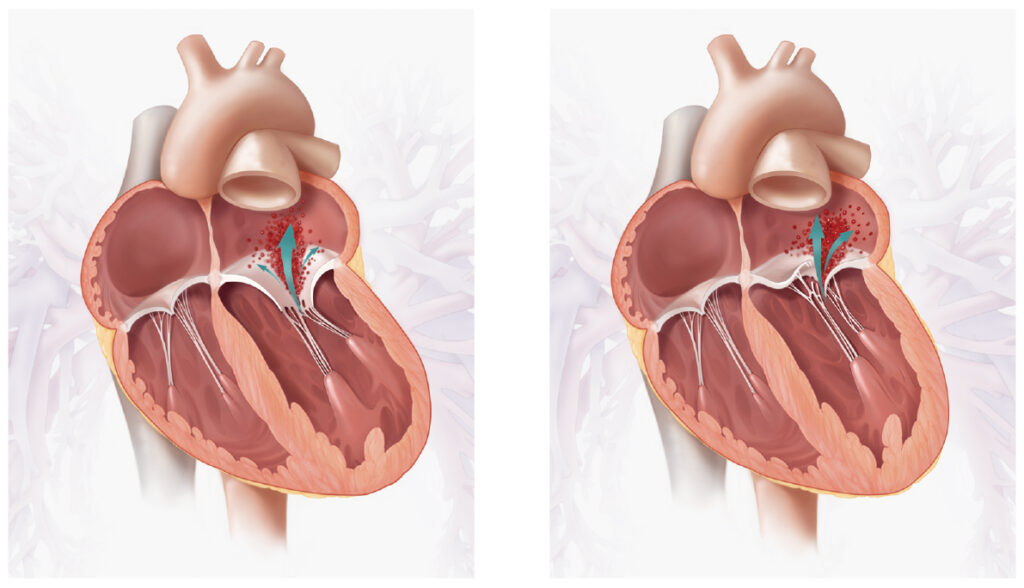
Mitral regurgitation: when the leaflets do not close properly, with every heartbeat blood may leak in reverse direction towards left atrium.
What are the possible treatment options for mitral regurgitation?
It is important to talk to your doctor about the effects of not having the procedure
Depending on your individual health needs, some centres across United Kingdom can now offer patients with mitral regurgitation who are not suitable for open-heart surgery an alternative, much less invasive keyhole valve procedure called:
Mitral Valve Transcatheter Edge-to-Edge Repair (TEER)
Back to topMitral Valve Transcatheter Edge-to-Edge Repair (TEER)
What is TEER?
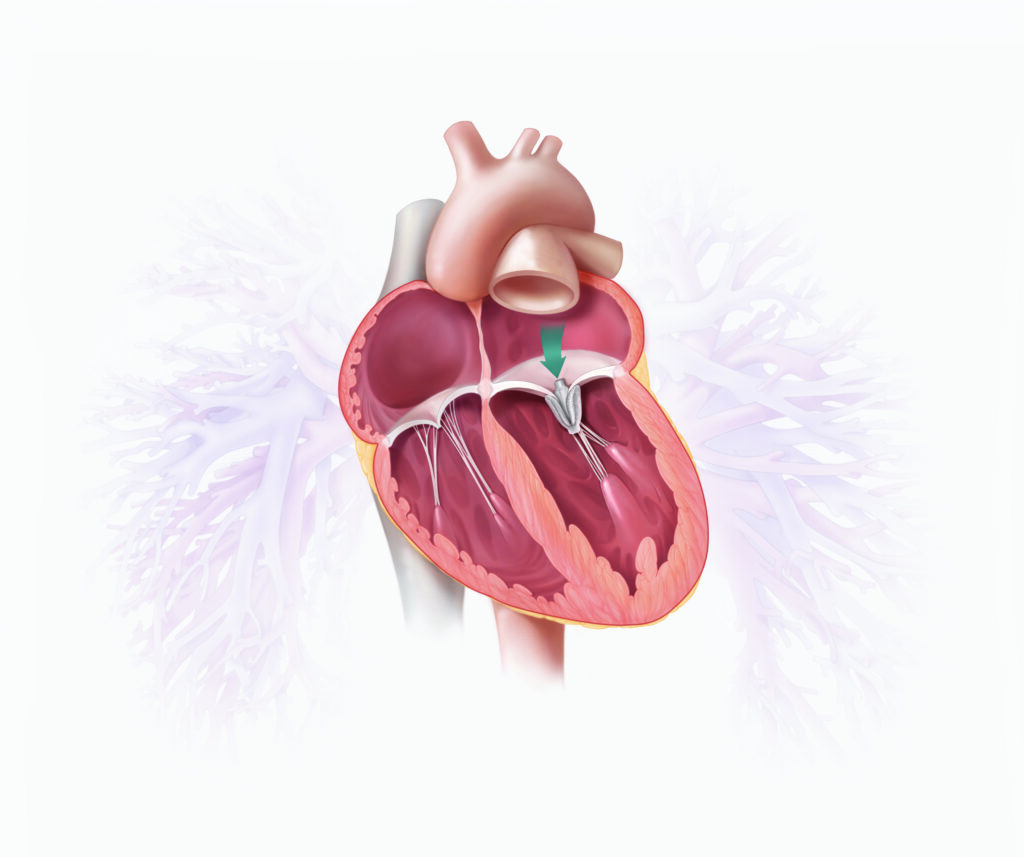
You may be suitable for another form of valve repair, one which does not require open heart surgery, this is TEER. The valve is repaired percutaneously (“through the skin”) via a vein in the groin using a catheter (thin flexible tube). On the top end of this tube, a clip is attached which holds the leaflets together in the abnormal area of the valve and holds it to together to reduce the leak (or regurgitation). This method does not require the breastbone to be cut or open heart surgery to be performed.
However not all leaking mitral valves are suitable for TEER. The decision if the leaking mitral valve is suitable or not will be made after review of all the imaging.
What will happen before the procedure?
Preparing for any mitral valve procedure requires a series of hospital tests that are essential to make sure that you will benefit from having it done. The tests also check that it would be a safe procedure for you.
What can I do to improve my health before TEER procedure?
The Heart Team Meeting
All cases are discussed in a multi-disciplinary team (MDT), or heart team meeting, made up of relevant valve specialists, including consultant cardiologists, consultant cardiac surgeons, imaging specialists, heart valve nurse specialists, and sometimes anaesthetists.
We will analyse all the data and information to make an informed decision about the best management and treatment option for your condition.
Pre-assessment Visit
Once accepted by the team for your mitral valve procedure, you will be invited to attend a pre-admission clinic. You will be provided with the details of your procedure preparation and admission process. We will also discuss the care before, during and after your TEER.
Usually, you will see the nurse during this visit. Occasionally, they find something about your general health if for example, have a cold, rash or infection that could increase the risks associated with anaesthetic or operation. It might then be better to delay your operation until the problem has been resolved and reviewed.
You may wish to bring a friend or family member with you during this visit.
While you are waiting for your hospital admission, it is important to contact the valve nurse specialist should your symptoms worsen or your health start to deteriorate. We will also need to be informed of any unplanned admissions to hospital.
The contact number is 0113 392 5298.
What will happen during the procedure?
In the cardiac catheterisation lab
The anaesthetist may prescribe a sedative, usually a tablet, to help you relax This will be given by the nurses before you go for your procedure. You will then be taken to the cardiac catheterisation lab (“cath lab”). One of the nurses from the ward will come with you and stay with you until you are transferred into the care of the anaesthetist. When you arrive in the catheterisation lab, the anaesthetic assistant will check your details, and you will be transferred onto the operating table and moved into the anaesthetic room. Here, the anaesthetic assistant will attach you to a heart monitor and place a pulse and oxygen monitor on your finger.
The anaesthetist will then put a drip into a vein in your hand or arm, through which the anaesthetic can be given to send you to sleep and.
After this, you will receive some oxygen through a mask and the anaesthetist will start to give you the anaesthetic medication. Once you are anaesthetised, a tube will be placed in your windpipe so that the anaesthetist can support your breathing during the procedure and further drips will be put in place: some into veins in your arms, and some into veins in your neck. A catheter will be put into your bladder to drain urine during the procedure. All of this allows us to monitor you closely during the operation and to give you drugs and fluids.
Once you are asleep, a trans-oesophageal echo (TOE) probe will be passed into your oesophagus (also known as your gullet or “food pipe”). A TOE is a special type of ultrasound that uses sound waves to take very clear pictures of the heart. This allows your cardiologist to use TOE to guide the catheters carefully into your heart.
First, a small incision (cut) in your groin is made and then, through the incision, a tube is inserted into the large vein in your groin. Through this tube a catheter is inserted. Using x-ray pictures, the catheter is guided into your heart. To access your mitral valve a small puncture is made in the inter-atrial septum (the thin wall between the two upper chambers (the atria) in the heart). Once the catheter is in place, the clip device is delivered into position to repair the leak of the mitral valve. Some patients may require more than one clip to adequately repair the valve.
Occassionally patients need a blood transfusion during the procedure. You will need to inform the team if you have any objections to having a transfusion.
Because this is not open-heart surgery the nature of the repair is less precise and TEER does not always result in a perfect repair. However, the clip, or clips, will hold the 2 edges of the mitral valve leaflets in position and reduces the extent of the leak. The result of the clip is a mitral valve with two openings instead of one with blood able to flow through both openings. The clip procedure will reduce the leak in around 90% of patients. In most patients the leak is reduced a lot. In some patients the leak is only reduced a little, but still enough to improve your symptoms.
Occasionally we have to use an extra device to close the hole in the inter-atrial septum. We are usually able to predict this before the procedure so you will be told. This does not significantly add to the risks and is performed as part of the same procedure.
After your procedure
- You will go from the catheter suite to the coronary care unit (CCU) where you will be closely monitored.
- Normally you are woken up early after the operation.
- Whilst there are tubes in your groin, you will have to be on bed rest.
- Over the next 24 hours you will have your drips and sheath’s (tubes) removed.
- When these tubes are removed you can sit out and start to walk about.
- You will be in hospital for one to three days depending on how quickly you recover.
Recovery at home
You should have someone to care for you for the first week after you leave hospital. Please speak to your nurse or doctor as soon as possible if you think this will be a problem.
The following are general guidelines as everyone’s recovery is different.
Activity
You should avoid strenuous activity for four weeks. This includes heavy lifting (such as shopping, suitcases) or pushing and pulling (such as cutting grass, vacuum cleaning).
It is important for your recovery that you have a short walk every day. This can be gradually increased. You may feel tired and need to rest in the afternoon.
You do not have to avoid climbing stairs or walking up hill. You may have to start off at a slower pace and you may feel slightly out of breath when walking. This should improve as your fitness level increases.
You may notice that your ankles are swollen after the procedure. This is due to fluid retention. Please contact your GP if this swelling travels further than your ankles.
Wounds
Your wounds should be healed by the time you leave hospital. If they still require a dressing, we will organise a district or practice nurse to continue this.
Normally you will have stitches that need to be removed by the practice nurse in one week. We will advise you about this before you leave hospital. Please get your GP or practice nurse to check your wound if it becomes red or inflamed.
You may have bruising to your groin for a few weeks.
You may have a hard lump under the skin due to a collection of blood (haematoma). Please talk to your GP if this becomes painful or grows bigger.
Please continue to shower every day. You can use liquid soap. It is safe to get your wound wet but avoid putting soap directly onto your wound or rubbing your wound before it has healed completely. It is important to keep this area dry between showers.
Medication
You will need to continue most of your medications, including anticoagulation. If not anticoagulated, you may need to take a blood thinning tablet such as Aspirin or Clopidogrel.
You may be discharged with some painkillers and ideally you take regularly until you are no longer getting discomfort from your wound(s).
You can contact your GP or the valve nurses if you are confused regarding your medications.
Driving
The DVLA (Driving and vehicle Licensing Agency) guideline recommends that you do not drive for four weeks following your procedure. You will need to inform your insurance company that you have had your mitral valve repaired. If you have a LGV or PCV licence, you will need to have an exercise test before getting your licence back.
Air travel
Please check this with your consultant, nurse, or cardiac rehabilitation nurse. In most cases, you can travel by plane seven days after your procedure. The clip device will not set off metal detectors at airports.
Work
If you were working before your procedure, you should be able to return to work after about four weeks.
Cardiac rehabilitation
Cardiac rehabilitation is a programme of graduated exercise and general health discussions. You will be referred to this service and will depend on whether your local community cardiac team offers this.
Follow-up care
You will have a follow up appointment after your TEER and the valve team will advise you on this before discharge. The team will also decide on future follow ups.
Back to topContact details
Valve Nurse Specialists
Telephone: 0113 392 5298
Email: [email protected]
Ward L20
Telephone: 0113 392 7420
Ward L14
Telephone: 0113 392 7414
Cardiology bed manager
Telephone: 0782 502 8321
Additional information and support
British Heart Foundation
The website contains a wealth of helpful information on all aspects of heart disease including the conditions, tests, treatments, and rehabilitation.
Telephone: 0207 935 0185
Helpline: 0300 300 3311
Email: [email protected]
Website: www.bhf.org.uk
Heart Valve Voice
This charity provides information and support for people with heart valve disease.
Telephone: 0739 960 6386
Email: [email protected]
Website: www.heartvalvevoice.com
Valve for life UK
This website provides a range of information to help patients who may have been diagnosed with Mitral valve disease and are looking to understand the condition and transcatheter treatment options.
You can also access our information video via their website.
Explain my procedure
Transcatheter Mitral Valve Edge-to-Edge Repair
Website: www.explainmyprocedure.com/leeds/qr/teer/
Password: takeheart11221