You can access LTHT patient information video about post-surgery pain management, if applicable
Please read the following information booklet carefully as it will explain about how we will treat any pain you may experience during your stay in hospital.
Please feel free to ask your doctors and nurses about anything that is unclear, or if you have any unanswered questions about your care.
There is a pain management team within the hospital that visits most wards regularly. If you would like to discuss anything related to this booklet or feel you would like to speak to them before or after your operation, please ask the staff to arrange this for you and we will try and accommodate this.
The experience of pain is very different for everyone and only you know how much it hurts, so do not be afraid of being honest about the amount of pain you are feeling.
Tell your nurse as soon as you start to feel any pain so they can give you pain relieving medication as soon as possible. This will stop your pain getting worse and improve it, but be mindful that having your pain controlled is not the same as being pain free.
Pain is much easier to manage if you keep it under control by taking pain relieving medication regularly, rather than trying to cope and letting it build up. You need to think about what your pain is like while you are resting and when you move. You should be able to take a deep breath, cough and move without the pain being too much and preventing you from doing this.
If you usually take pain relieving medication at home to manage a chronic pain, please make sure you bring these medications into hospital with you to prevent any delay in you being given these whilst you are a patient in hospital.
Pain relieving medication may come in many forms such as tablets, liquids, patches and suppositories. If swallowing is a problem please discuss this with your nurse, doctor or pharmacist.
Please note that the pain team in this hospital is the Acute In-Patient Pain Team, and they are not the same as the Chronic Pain Team which is a service only accessed in the community setting via a GP. Chronic pain regimes should not be changed whilst you are an in-patient. If this is required, this is best done as an out-patient appointment with the initial prescribing practitioner.
Please note
(Please note this booklet does not include any pain relief information for patients under Obstetrics. Please speak to your Obstetrician should you have any queries about pain management throughout your antenatal or postnatal care.)
Content
Tick as appropriate
Sections 01 – 05 are relevant to all patients.
Sections 01 – 07b are relevant to all patients undergoing any operation (whether minor or major).
Sections 7c – 08 are relevant only to patients undergoing a major operation.
01: Pain Assessment Scale
02: Pain Relieving Medications
03: Alternative Routes of Pain Relief
04: Alternative Therapies
05: Pain Management after Discharge & Opioid Weaning Table
06: Patient Controlled Analgesia System (PCAS)
07: Spinal and Epidural Analgesia
08: Continuous Wound Infusion
09: Erector Spinae Plane Block (chest nerve block)
01 Pain Assessment Scale
You will be asked regularly by a member of the healthcare team to score your pain levels from 0 to 3.
0 = no pain at all,
1 = mild pain,
2 = moderate pain and
3 = severe pain.
Please keep in mind the Acute Pain Intensity Score below to help assist with this.
Acute pain intensity score
Assess pain intensity on movement
| 0 | No Pain |
| 1 | Mild Pain |
| 2 | Moderate Pain |
| 3 | Severe Pain |
02: Pain Relieving Medications
There are a variety of different medications available for managing your pain and your doctor or nurse can discuss with you the option that will suit you best.
Paracetamol
Paracetamol is used to relieve mild to moderate pain (Paracetamol is available over the counter from many retail outlets).
- Paracetamol is not always suitable if you have liver problems, or if you regularly drink more than the maximum recommended amount of alcohol (14 units a week).
Non-Steroidal Anti-Inflammatory Drug (NSAID)
An NSAID eases pain and reduces inflammation. There are many NSAIDs available such as Ibuprofen, Naproxen, Diclofenac and some which are less likely to cause indigestion such as Celecoxib and Parecoxib. However, in Leeds Teaching Hospitals we predominantly use Ibuprofen (Ibuprofen is available over the counter from many retail outlets).
NSAIDs are best taken with food to help protect the stomach from side-effects such as indigestion.
NSAIDs are not suitable for everyone and we may avoid them if you have:
- Severe asthma
- History of adverse reaction to NSAIDS
- Stomach or duodenal ulcer or any inflammatory bowel disorder
- A blood clotting disorder
- High blood pressure
- High cholesterol or blood sugar levels
- Reduced liver or kidney function
- Previous heart attack, angina, stroke or mini stroke (Parecoxib and celecoxib avoided in these conditions)
Opioids
Opioids provide pain relief by acting on areas in the spinal cord and brain to block pain signals. Opioids include some of the strongest painkillers available and are widely used to treat pain – for example after surgery, serious injury and cancer. Opioid drugs can help with some but not all types of pain.
Weak opioids
Dihydrocodeine, Codeine and Tramadol are classed as a weak opioid medicine. Weak opioids are used to treat mild-to-moderate pain. These can be particularly useful to add in when pain relieving combinations such as Paracetamol and Ibuprofen have not been effective.
Codeine is available as a combination with paracetamol in two strengths both known as Co-codamol. It is important that you do not take any other medicines which contain paracetamol whilst you are taking Co-codamol. Moderate strength Co-codamol is available over the counter from many retail outlets – strong co-codamol is only available on prescription.
Strong Opioids
Morphine, Oxycodone, Fentanyl and Buprenorphine are classed as a strong opioid. Strong opioids are used to treat severe pain that is not relieved by simple painkillers alone, such as paracetamol and ibuprofen, and a weak opioid.
Both weak and strong opioids can have some unwanted side effects such as:
- constipation
- drowsiness
- nausea
- headaches
- dizziness
- poor concentration
- sedation and respiratory depression – particularly with strong opioids.
If you experience any other symptoms which you think may be due to the medicine, discuss them with your nurse or doctor for further advice.
There can be risks to your health and well-being if you continue taking opioids at high doses for a long period of time:
- reduced fertility
- low sex drive
- irregular periods
- inability to keep an erection
- reduced ability to fight infection
- increased levels of pain
- addiction
- reduced quality of life
Long term repeated use of prescription opioids can lead to drug dependency. The absence of these drugs can then cause several physiological reactions, all of which could negatively impact your life.
Can I drive if I am taking opioids?
UK law allows you to drive if you are taking opioid medicines as long as you are taking them as prescribed. You are responsible for making sure you are fit to drive. It is important that you do not drive or operate heavy machinery until you see how the opioids affect you as it is highly likely that your reactions and alertness will be affected. You should not drive if your dose has changed or if you feel unsafe. You do not have to inform the Driver & Vehicle Licensing Agency (DVLA) that you are starting an opioid. However, there may be other information about your illness that the DVLA needs to know.
Is it safe to drink alcohol when I am taking opioids?
Alcohol and opioids together cause sleepiness and poor concentration. You should avoid alcohol completely when you first start on opioids or when your dose has just been increased. If you are taking a regular steady dose of opioid, you may be able to drink modest amounts of alcohol without getting any extra unusual effects.
How do I store opioids?
You should store opioids safely in a cool, dark place. Make sure it is well out of reach of children, vulnerable adults and pets. It is important that only YOU take the opioids prescribed for your pain. Opioid medicines should be kept in their original containers and clearly labelled.
Dependency and addiction
As with all strong pain relieving medication, there is a risk that you may become addicted or reliant on these tablets. It is important that you aim to stop taking opioids within a time frame agreed with your GP. Opioids are very good for acute short term pain relief and pain control at the end of life but there is little evidence that opioids are helpful in long-term pain management.
Many people reduce their opioid dose and find that their pain is no worse and their enjoyment of life and physical fitness improves.
For more information please visit:
https://www.gov.uk/guidance/opioid-medicines-and-the-risk-of-addiction
Neuropathic agents
You may require medicine to treat nerve pain (neuropathic pain). Neuropathic pain is pain that is caused by damage to the nervous system. A doctor or nurse will assess for signs of neuropathic pain and start this medication if appropriate.
Unlike most other types of pain, neuropathic pain does not usually get better with common painkillers, such as paracetamol and ibuprofen, and other medicines are often used.
Neuropathic pain medication should usually be started at the minimum dose, with the dose gradually increased until you notice an effect, which can take several days. Higher doses may be better at managing the pain, but are also more likely to cause side-effects.
The most common side-effects are:
- tiredness
- dizziness
- feeling ‘drunk’
- twitching
If you experience any of the above side effects, it may be necessary to reduce your dose. However, the side effects often improve after a week or two as your body gets used to the nerve pain medication.
Many of these neuropathic pain medicines are also used for treating other health conditions, such as depression, epilepsy, anxiety or headaches. If you are given an antidepressant to treat your pain this does not mean your doctor suspects you are depressed.
The main medicines recommended for neuropathic pain include:
- Amitriptyline – also used for treatment of headaches and depression.
- Duloxetine – also used for treatment of bladder problems and depression.
- Pregabalin and Gabapentin – also used to treat epilepsy, headaches or anxiety.
03: Alternative routes of pain relief
In certain circumstances it may be necessary for you to have pain relieving medication via an injection (either under the skin/into the muscle/into the vein) or via a suppository (a wax pellet into your back passage). This type of pain medication is often used if you are feeling sick or you are unable to eat and drink.
04: Alternative therapies
There are many other things that you can do to help keep yourself comfortable. Some of these are:
- Regularly change your position in bed as well as getting up and moving around as much as possible.
- Distraction therapies such as:
– reading a book or magazine
– listening to music
– completing a puzzle
– watching movies - If you have had an operation use a pillow to support your wound when you need to cough or move.
05: Pain management after discharge
Please make sure you have a supply of Paracetamol and/or Ibuprofen (if appropriate) at home, as these may not necessarily be supplied to you by the hospital before you go home.
You may be discharged home with some stronger pain relieving tables, for example: tramadol, codeine or very occasionally morphine tablets.
Please note that you will not necessarily need to continue taking these pain killers long-term. If your pain begins to settle over the following days/weeks, you can start to reduce the amount of pain killers you take. Please follow any guidance outlined in your discharge letter.
If you have pain relieving medication left over once your pain is managed it is important to dispose of the medicine safely. It is recommended to take the medication to your local pharmacy, whether or not they have expired. Pharmacies have the ability to dispose of medication in the safest way possible. Do NOT flush them down a toilet or throw in the rubbish bin.
Opioid Weaning Table
Please feel free to use the table below with assistance from a healthcare professional to help plan how to reduce your opioid medication once you are discharged home. The dose of the opioid should be reduced gradually by at least 10-20% per week, you can reduce it by more if you feel able.
Aim to reduce the dose as follows:
Please note
This table will be completed on your physical copy of the leaflet.
For more information related to this section please see the following websites:
Taking opioids for pain | Faculty of Pain Medicine
Drugs and driving: the law – GOV.UK
Relevant to all patients undergoing any operation
When you wake up from your operation you will be asked if you are comfortable. If you are experiencing discomfort the nurse will ask you to score your pain from 0 to 3. Keep in mind the pain assessment scale highlighted at the beginning of this booklet.
Following your operation you may have more than one means of pain relief. This will help you stay comfortable to be able to take deep breaths, cough and move about which reduces the chance of you suffering from any side-effects, such as a chest infection or blood clots in the legs.
Good pain relief will help you recover from an operation quicker and get you home sooner.
Keep in mind that it is normal and unavoidable to have some pain after surgery. The pain relief you are given should be sufficient to allow you to deep breathe and cough and move around.
You may have one or two of the following means of pain relief after your operation to keep you comfortable.
06: Patient Controlled Analgesia System (PCAS)

PCAS is a type of pain relief, which allows you to manage your own pain. This way you do not have to wait for a nurse to prepare and give you pain relieving injections.
When using a PCAS you are connected to a machine which contains a supply of pain relieving medication (an opioid) which will be given via a tube directly into a vein, usually on your arm. You are given a button to press, to tell the machine to give you a dose of the pain relieving medication. The PCA will be programmed by the doctor or nurse to deliver a dose of pain relieving medication when you press the button. Whilst this dose is working, even if you press the button, the machine will not give you another dose. After a pre-set time (usually five minutes) when this dose has worked you can give yourself another dose if you need it by pressing the button again. In this way you control the amount of pain relieving medication that you receive. The system is very safe to use – if you do become very drowsy (indicating you should not have any more doses) the drowsiness itself prevents you pressing the button so you will not give yourself any further doses until you are more awake.
It is important to remember that the chance of you becoming addicted to the pain relief or giving yourself too much is very small.
PCAS opioids are generally very effective however there are some possible side effects to be aware of:
- Constipation
- Nausea
- Headaches
- Dizziness
- Poor concentration
- Hallucinations
- Drowsiness and depression of breathing
You are closely monitored for the above side-effects whilst you are using a PCAS but if you experience any of the above between this monitoring please inform your doctor or nurse as most of these symptoms can be managed with other medicines.
In most cases you will be given Paracetamol and sometimes an anti-inflammatory drug (NSAID) as well as the PCAS.
07: Spinal and Epidural Analgesia
07a Spinal single injection (please also read 7d)
A spinal anaesthetic is sometimes used for surgery below the waistline which consists of a single injection of local anaesthetic into the fluid around the nerves in your spine.

The local anaesthetic is injected in the middle of your lower back using a needle (having numbed the skin area first). This numbs your lower body and legs, makes your legs feel very heavy and allows painless surgery with you awake. Sometimes a dose of long acting strong pain medication is added to the local anaesthetic injection, which provides some additional pain relief in the post-operative period. Spinal anaesthesia using a long acting pain killer may be used along with a general anaesthetic for abdominal surgery to provide pain relief for a variable period after surgery.
07b Epidural Single Injection (please also read 7d)
An epidural anaesthetic is sometimes used for surgery below the waistline. The nerves to your lower body leave the spine and pass through an area in your back close to the spine called the epidural space. When you have a single injection epidural an anaesthetist will perform an injection in the middle of your lower back to introduce local anaesthetic into the epidural space (having numbed the skin area first). This numbs the nerves in this area giving you a band of numbness around your body.
This technique can be used alone to allow painless surgery to occur while you are awake. Sometimes a dose of long acting strong pain killer drug is added to the local anaesthetic injection, which provides some additional pain relief in the post-operative period. Epidural single injection anaesthesia using a long acting pain killer can also be used with a general anaesthetic for abdominal surgery to provide pain relief for a variable period after surgery.
07c Continuous Epidural Analgesia (please also read 7d)
For major surgery, particularly major abdominal or chest operations, an epidural can be used to supplement a general anaesthetic, and then continued after the operation for several days for pain control.
The nerves to your chest and abdomen leave the spine and pass through an area in your back close to your spine, called the ‘epidural space’. When you have an epidural, an anaesthetist uses a needle (numbing the skin if you are awake) to place a fine plastic tube (an epidural catheter) into the epidural space.
Local anaesthetic and sometimes other pain relieving medications are put through the epidural catheter.
This aims to give you a band of pain relief around your body at the site of your surgery. The local anaesthetic will cause some numbness as well as pain relief.
An epidural pump is used to give pain relief drugs continuously through the epidural catheter after your operation. The pain relief lasts as long as the pump is running which is usually stopped on day three (day zero being the day of your operation). When this is stopped, full feeling will return within a few hours therefore other pain relieving medication will be given to you before the epidural is stopped.
While both spinals and epidurals are effective methods of pain relief you will be closely monitored during and after your operation as they are not without a small risk of side effects and complications.
7d Common side-effects of spinals and epidurals
The following may be unpleasant, however can be treated and do not usually last long:
- Discomfort – during insertion of the spinal/epidural you may feel tingling or a sharp sensation running down your legs or bottom or around your side. This could be due to the needle brushing against the nerve. Try to stay still and inform your anaesthetist.
- Low blood pressure – this can make you feel sick or faint. Your anaesthetist or ward nurse will give you fluids through a drip and other medications to help improve your blood pressure and any sickness or dizziness.
- Feeling sick – this is less common with epidurals than other methods of pain relief, and can usually be treated effectively.
- Difficulty passing urine – whilst the spinal/epidural is working you may find it more difficult than usual to empty your bladder. Your bladder function usually returns to normal when the spinal/epidural wears off. You may require a temporary catheter to help you pass urine which are often necessary after major surgery anyway.
- Inadequate pain relief – if you are having an epidural, occasionally like with other methods of pain relief, it may not relieve all of your pain.
An anaesthetist or specialist pain nurse will decide if it can be improved or if you need to switch to another method of pain relief. If long acting pain relief via a single spinal injection was used and is not adequate then other strong pain killers will be given.
Rare complications
- Severe persistent headaches – A mild headache is not uncommon after surgery and can be due to a number of different factors.
- On-going backache – is thought occasionally to result from epidural insertion.
- Catheter infection – infection can occasionally occur around the tube of the epidural. If this happens it will be removed. Alert a member of staff if you experience any headaches, a stiff neck, fevers or vomiting.
It is much rarer for a deeper infection to develop, which may require antibiotics or (rarely) emergency back surgery. Disabling nerve damage due to an epidural abscess is very rare indeed (see next page).
Very rare complications
- Nerve Damage
Temporary – Uncommonly, loss of sensation, pins and needles and sometimes muscle weakness lasting a few days, weeks or months can occur. In most people this gets completely better in time.
Permanent nerve damage causing permanent leg weakness and numbness after spinal or epidural is very rare. A study has shown it happens in between 1 in 6,000 and 1 in 12,000 epidurals used for surgery and 1 in 50,000 spinals. Also nerve damage can happen for other reasons during surgery, related to the surgery itself or for other medical reasons unrelated to the epidural or spinal.
These very rare complications of spinal or epidural can be caused by:
- Haematoma (collection of clotted blood) in the spinal canal or epidural space is very rare but can require emergency back surgery to attempt to prevent disabling nerve damage.
- Spinal epidural abscess is an accumulation of pus in the epidural space that can mechanically compress the spinal cord. Diagnosis is by MRI or CT scan. Treatment involves antibiotics and sometimes drainage of the abscess.
Both haematomas and abscesses benefit from early detection. Your epidural will be examined daily for signs of infection and you will be closely monitored for any leg weakness or numbness. Once you are discharged home, please note that, in the very unlikely event that you were to experience new numbness/loss of sensation to your legs and/or leg weakness and/or severe sudden back pain occurs, please seek urgent medical advice.
- Direct damage to nerves on epidural or spinal injection is possible but is very rare.
- Slow breathing – some drugs used in a spinal or epidurals can cause slow breathing or drowsiness, which requires treatment.
- Convulsions (fits), severe breathing difficulty and death are all extremely rare complications of an epidural.
For more information related to this section please see the following websites:
Page not found – 404 | The Royal College of Anaesthetists
Page not found – 404 | The Royal College of Anaesthetists
Page not found – 404 | The Royal College of Anaesthetists
Please access the following video link introducing you to the In-Patient Pain Management Team who talk around what to expect after your surgery and how we may manage any pain you may experience:
Inpatient Pain Management LTHT
(Only relevant to patients undergoing a major operation – Sections 7c and 7d above also relevant to major surgery)
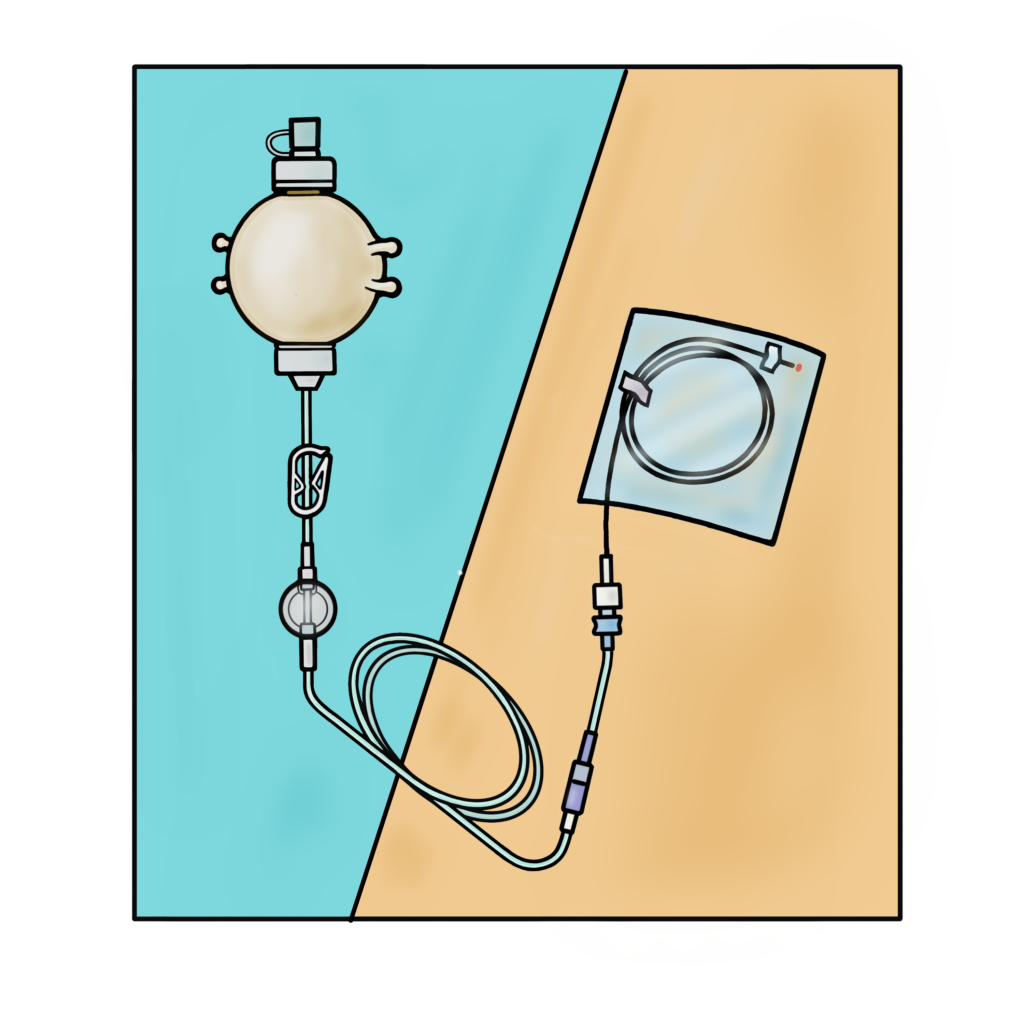
08: Wound Catheters
A Continuous Wound Infusion is a system which administers local anaesthetic, through a pump, directly into your surgical wound via one or more small plastic tubes which is placed during the operation by the surgeon. They can stay in for several days after your operation.
Local anaesthetic generally works well, you probably will still be able to feel touch and movement, but you should not be able to feel pain.
Wound catheters are almost always used alongside another strong pain killer. Either tablets or a patient controlled analgesia system (PCAS).
Wound catheters are generally very effective, and complications are extremely rare, however there are some risks to be aware of.
Rare complications
These are mostly catheter-related complications. Your wound catheters will be monitored by nursing and medical staff to assess for this.
- Ineffective pain relief – the correct placing of wound catheters is important for them to be effective. Incorrect placing or catheter dislodgement or disconnection could lead to more pain after surgery than expected. Please let a member of staff know if you are experiencing pain.
- Delayed wound healing due to the catheter tubes being in place.
- Infection of the wound, or the surrounding skin.
- Haematoma formation (a swelling of clotted blood).
- Difficulty removing the wound catheters including retention of a section of wound catheter in the wound.
Although extremely rare and unlikely, local anaesthetic toxicity could be possible due to the misplacement of a wound catheter into a blood vessel. You will be monitored for this.
09: Erector Spinae Plane Block (chest nerve block)
An Erector Spinae Plane Block is an injection of local anaesthetic at the upper part of your back which targets the nerves responsible for pain sensation in your chest. This injection is carried out by an anaesthetist and involves placing a local anaesthetic drug around the nerve to block the pain signals and make the chest wall feel numb.
Using this block together with other painkillers will help with pain relief after chest trauma or injury.
What are the benefits of the ESP Block?
- Less need for strong painkillers, which can make you feel sick or drowsy.
- Being able to take deep breaths and cough, reducing your risk of a chest infection.
- Being able to move around earlier and get home sooner.
What are the possible complications of the ESP Block?
Nerve blocks are generally very safe, however, as with most procedures in hospital, there are some risks to be aware of:
- Partial or no effect from the block – other pain relief options are available if this occurs.
- Bruising or bleeding at injection site.
- Infection at injection site.
- Damage to nearby blood vessels, nerves or lung lining (rare).
- Local anaesthetic allergy or toxicity (very rare).
Local Anaesthetic Toxicity
There are risks of local anaesthetic toxicity with both an erector spinae plane block and wound infusers as follows.
Uncommon side-effects:
- Feelings of anxiety or paranoia
- Light-headedness
- Visual Disturbances (sometimes ‘tunnel vision’)
- Tinnitus (ringing inside of the ear)
- Metallic taste in the mouth
- Numbness of the tongue and around the mouth
Rare side-effects:
- Arrhythmias (abnormal heart rate)
- Lower blood pressure
- Unconsciousness and coma
Very rare side-effects:
- Death

Understanding risk
People vary in how they interpret words and numbers. This scale is provided to help.
You can access the internet link below to view Leeds Teaching Hospital Trusts patient information video regarding pain management after your surgery if appropriate:
Inpatient Pain Management LTHT
Back to top