This leaflet provides information for parents and carers about partial atrio-ventricular septal defect in children and the management and treatment of this condition.
Partial Atrio-Ventricular Septal Defect
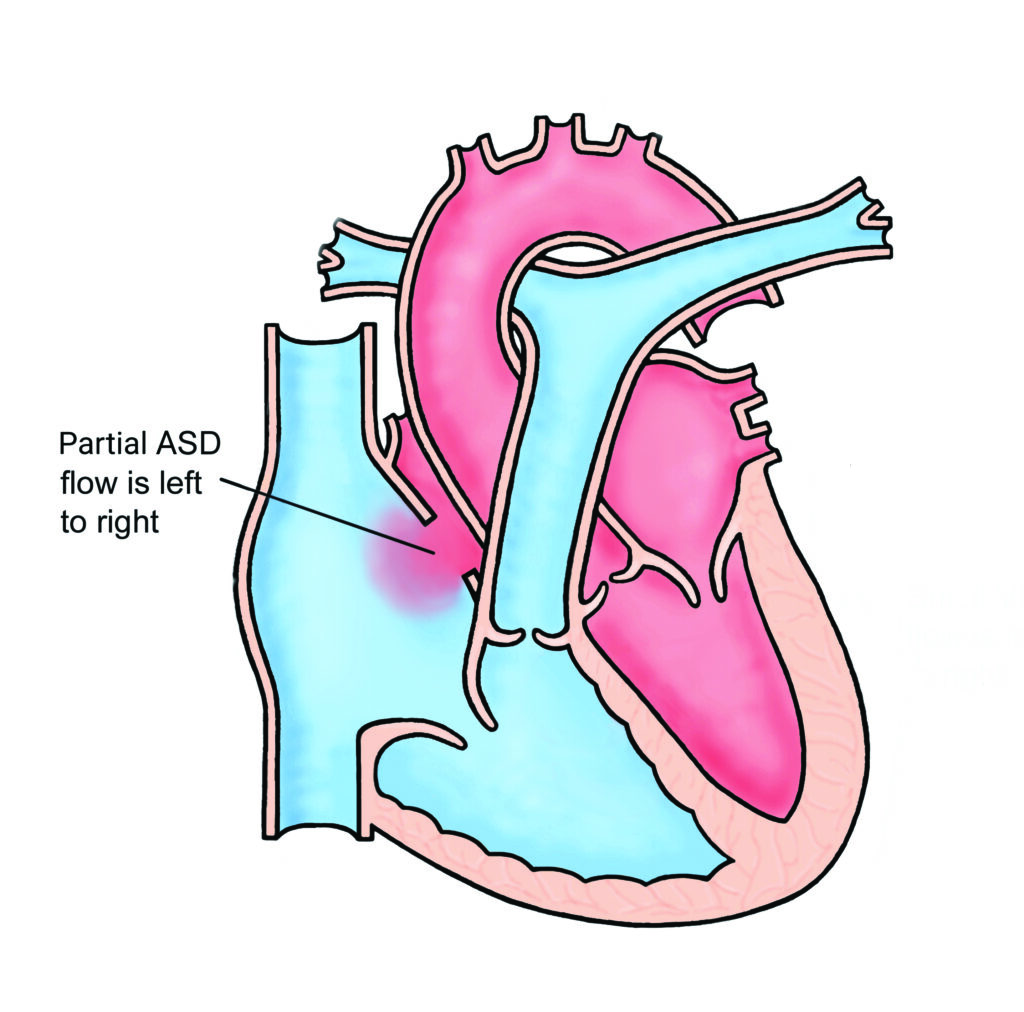
This is a serious heart abnormality which consists of a hole between the two small pumping chambers (atria). The hole also affects the inlet valves of the heart.
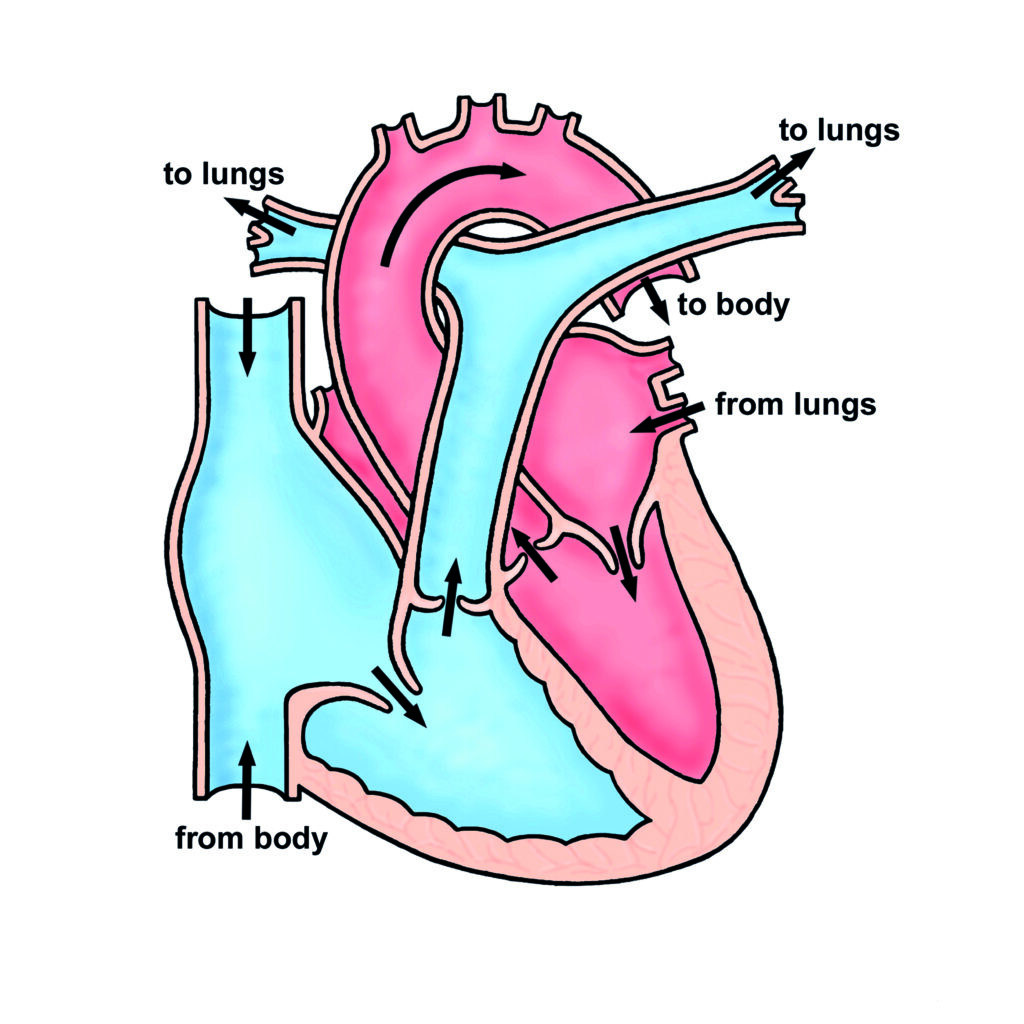
Normally there is a separate inlet valve in the right side of the heart (tricuspid valve) and a separate inlet valve in the left side (mitral valve). With atrioventricular septal defect (AVSD) there is a single valve known as a common valve.
This abnormality of the inlet valves in AVSD often stops the valves (particularly the mitral valve, on the left side of the heart) closing properly, so it is not watertight when it closes.
Tests
An ultrasound scan of the heart (an “echocardiogram”) is required to make the diagnosis, and to watch for any new problems developing as the child grows.
Treatment
Children with partial AVSD usually look perfectly well when they are young, but if the defect is not repaired it can eventually (after many years) cause permanent damage to the heart and the lungs. Surgery is usually recommended before school and sometimes before the age of 1 year. The surgery is complicated because the surgeon has to close the hole at the same time as dividing the common inlet valve into separate right and left parts.
The main problem with surgery is that the left sided inlet valve (mitral valve) always leaks to some extent after the hole is closed (this is called mitral regurgitation). If the mitral valve only leaks a little this may not matter and further treatment may never be necessary. However, if the mitral valve leaks badly further major surgery may be required to repair or replace the mitral valve.
Replacing the mitral valve (a metal valve is normally used) in young children is a difficult procedure and carries a further risk to the child’s life. Further major surgery is always necessary after valve replacement in young children because they outgrow the valve. You will meet the surgeon prior to surgery who will explain the operation in detail including the risks and potential complications.
Follow up
It is important for all patients with a repaired AVSD to be seen in the cardiology outpatient department to make sure that mitral regurgitation does not become worse as time goes by. In addition, a small proportion of children can develop narrowing of the outflow of the left ventricle (subaortic stenosis) after repair of the AVSD. This may need surgical treatment.
General advice for the future
Patients with repaired AVSD generally live normal active lives, including all kinds of sport. Most have a normal exercise tolerance but if there is significant mitral regurgitation it is usual to be more breathless than normal with exercise.
All patients with a repaired partial AVSD will be at risk of infection in the heart (called endocarditis). Such infections may be caused by infections of the teeth or gums, so it is very important to look after your child’s teeth and gums carefully and visit the dentist regularly (every 6-12 months). Ear or body piercing and tattooing are best avoided as they carry a small risk of infection which may spread to the heart. For more information about endocarditis please see the link below: