You have received this leaflet because you have been diagnosed or are undergoing tests for Polycystic Ovary Syndrome (PCOS).
This leaflet explains what PCOS is and how it may be affecting your health and fertility. It provides some options for lifestyle change that will help your overall health and should help to increase the possibility of having a baby if you choose to.
More information is available on our website: www.leedsth.nhs.uk/services/fertility/
Please ask your nurse specialist or doctor any questions. We are here to help.
What are polycystic ovaries and what is Polycystic Ovary Syndrome (PCOS)?
‘Polycystic ovaries’ (PCO) is a descriptive term for the appearance of ovaries on ultrasound examination when they have lots of small bubbles or cysts in them. These are egg-bearing sacs or ‘follicles’, that have stopped growing and do not reach the stage of egg-release or ovulation.
When you are born, you will have many more eggs than you can ever use or ovulate. You are born with about one million eggs yet the maximum number that could ever be ovulated is about 450, if you never get pregnant and never take contraceptives to stop ovulation. Every day, about 30-40 eggs leave the dormant store and begin the journey towards ovulation.
Most fall by the wayside and never mature fully. Only one egg reaches maturity each month for ovulation. Usually the rest disappear and are not detected by ultrasound scans. For reasons that we still do not completely understand, some of these get stuck in the natural process of turnover and form the cysts we see on modern ultrasound scanning. Each ovary needs to have 20 or more cysts to fall under the current definition of being polycystic, but this does fluctuate.
Normal Ovary
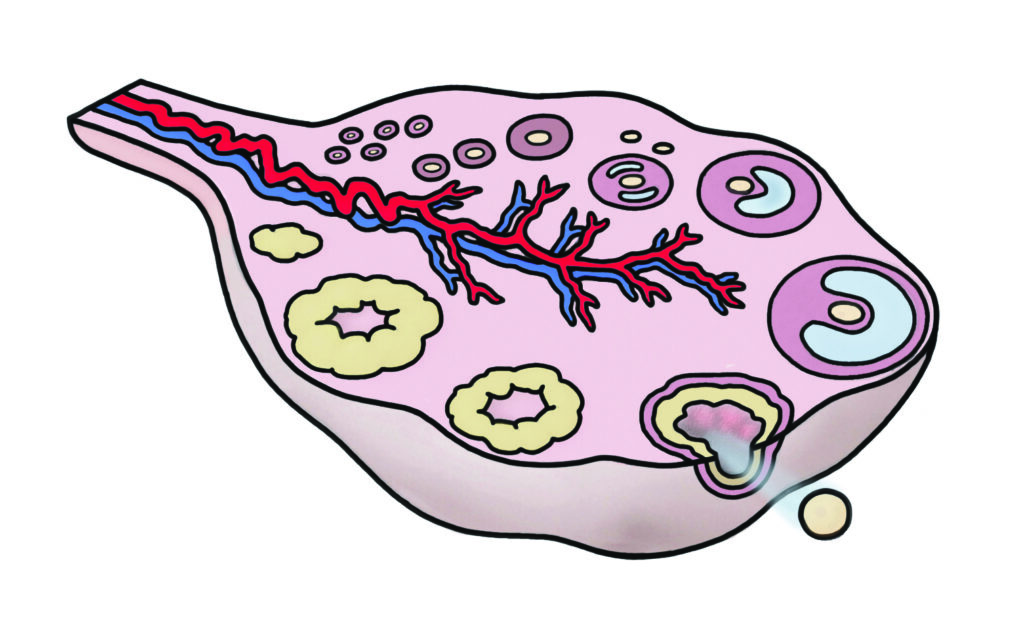
Polycystic Ovary

The ovaries contain eggs but they also produce hormones from puberty onwards, including after the eggs have all gone after the menopause. Hormone production changes during the menstrual cycle with the development of the ovulating egg. Other cells in the ovary produce hormones that affect the development of healthy eggs (e.g. oestrogen & testosterone). The ovary itself is controlled and influenced by other hormones. The pituitary gland (master gland) in the brain is crucial to the cyclical pattern of menstrual periods. It releases Follicle Stimulating Hormone (FSH) to kick start the development of the monthly egg-containing follicle and Luteinizing Hormone (LH) to trigger the release of the mature egg (ovulation). Other hormones can also affect hormone production by the ovary. Insulin and similar hormones are especially important here.

Polycystic ovary syndrome (PCOS) is the commonest hormonal problem found if you are trying to conceive. PCOS is not the same as having ‘polycystic ovaries’.
Polycystic ovaries (PCO) can affect 1 in 4 people, most are fit and well, have no problems or concerns and may conceive naturally. Around 1 in 10 have a mixture of other symptoms and the combination is often enough to make the diagnosis of PCOS. It is important to understand that symptoms of PCOS can vary enormously and can also change at different stages of life.
Typical symptoms include:
- Irregular or absent periods.
- A tendency to put on weight and have difficulty losing it.
- Greasy skin with a tendency to breakouts like acne.
- Unwanted thick hair growth (especially on the face and elsewhere on the body) and sometimes thinning of the hair on the scalp.

You may find you have quite mild symptoms or quite troublesome symptoms.
The currently accepted definition for PCOS is the presence of two out of the following three features (when other reasons have been ruled out):
- Symptoms of high testosterone (unwanted hair, acne) or high testosterone on a blood test.
- Irregular or absent periods.
- Polycystic ovaries on scan.
What causes PCOS?
We don’t know exactly what causes PCOS but we believe that people with PCOS are born with the likelihood of developing the syndrome. It seems to run in families and is more common in some ethnic groups e.g. south Asians. However a single faulty gene has not been identified and there appear to be a number of genes involved. For some the condition is associated with a tendency to produce too much LH from the pituitary gland, whilst for others, particularly those who are overweight, the condition is associated with faulty insulin hormone function and a diabetic tendency. The different features of PCOS may vary and can change over time. Gaining weight is very often associated with worsening symptoms. Insulin hormone is needed to convert sugar (carbohydrate) into energy. When we gain weight, insulin works less well but is produced in larger amounts. More sugar ends up being stored in the body (as fat) rather than being burned up to make fuel.
This sets up a vicious cycle which is hard to break, unless sugar and carbohydrate consumption are reduced (low carb diet) and the energy stores are called upon more often (by increased physical exercise).
Insulin levels that are higher than normal also have other side-effects, including on the ovary which responds by producing more testosterone. The skin and hair follicles react to these signals producing the unwanted visible signs of PCOS. Other hormonal imbalances prevent the ovary from releasing eggs normally and this is what causes irregular or absent periods and delays pregnancy.
What tests do I need?
The diagnosis is often suspected from listening to the story of symptoms and the tests will confirm it. It is important to rule some things out that can rarely cause some of the symptoms. Other treatments would be needed in these cases.
Blood tests

- FSH / LH / Oestradiol
- Thyroid function tests
- Prolactin
- Testosterone
- HbA1C diabetes test or Glucose Tolerance Test
- Cholesterol / lipid profile
- Vitamin D
Ultrasound scan
What is the treatment of PCOS?
Polycystic ovaries by themselves do not require any treatment. The cysts (‘follicles’) are not dangerous or painful and do not progress into anything serious. General advice aiming for a healthy lifestyle is important to prevent the slippery slope of the consequences of high insulin levels and weight gain (diabetes, heart disease, blood pressure problems).
The treatment options are dependent on the main symptoms of concern:
Irregular periods
If you have infrequent or absent periods you are at risk of overgrowth of the lining of the womb (endometrium). It is important that the endometrium is shed on a regular basis (period) to prevent this from happening because if the endometrium becomes too thick it may sometimes develop into cancer of the womb (endometrial carcinoma).
The endometrium can be seen on an ultrasound scan and if it appears too thick, or irregular, a dilatation and curretage (D & C) operation is advised in order to take a sample (biopsy) and examine the endometrium under a microscope.
Irregular and unpredictable periods can be unpleasant and a nuisance as well as suggesting irregular ovulation and the risk of endometrial thickening. If pregnancy is not desired the easiest approach is the use of a low dose combined oral contraceptive (that is a contraceptive pill).
This will result in an artificial cycle and regular shedding of the endometrium.
If you cannot take the pill you may require alternative hormonal therapy to induce regular periods, such as a progestogen for 5-10 days every 1-3 months, depending upon your individual requirements. It is important to have a period at least once every 3 – 4 months to prevent abnormal thickening of the womb lining.
An alternative way of protecting the womb lining from getting too thick is to use a progesterone-secreting coil (Intrauterine System) which releases the hormone progesterone continuously in a very low dose into the womb. This prevents the lining from thickening up and often results in reduced or absent menstrual bleeding. You may find this a convenient and easy choice as you do not have to remember to take a daily pill or a course of pills. The coil needs to be replaced after five years. It can be removed easily by a doctor or trained nurse. Whilst it is contraceptive when it is in place, once it is removed your hormones will come back to what is normal for you.
You will need to keep a record of your periods to make sure they are coming often enough (at least every 3-4 months). If they are not, you should seek medical help to make sure the lining is not abnormally thick, and for treatment to protect the womb lining or fertility advice.
Infertility
If your menstrual cycle is irregular, ovulation is also irregular or absent and it will take longer to get pregnant. Fertility treatment can help achieve a regular ovulatory cycle and hence a better chance to conceive.
It is important that you are a healthy weight. If you are overweight (or underweight) you will have a reduced chance of pregnancy either naturally or with fertility assistance. In addition, the risks of pregnancy, including miscarriage are higher. Getting to a healthy weight, through diet and exercise, before starting treatment is required.
It will be necessary to check that your fallopian tubes are open (‘patent’) and that there is enough sperm available to achieve a pregnancy.

Ovulation induction
Two drugs ( Letrozole and Clomifene / clomid) in tablet form are available to regulate your cycle and kickstart ovulation. Approximately 75% will ovulate on these drugs.
In 6 out of 10 cases, you will become pregnant within 6 months of treatment.
If one of these tablets does not work, alternatives include daily hormone injections of a drug that contains FSH or a surgical treatment known as laparoscopic (‘key hole’) ovarian drilling (burning small holes in the ovary).
If ovulation induction is not successful you can move forward to IVF (‘test tube baby’) treatment.
As insulin problems are a key feature of PCOS, drugs that improve insulin resistance have been used to try to improve the way the ovaries work e.g. metformin. Although large studies have suggested improvement in the menstrual cycle and ovulation, there is no good evidence that taking these drugs improve the chance of having a baby. We tend to recommend metformin if there is a proven problem with high glucose levels (pre-diabetes).
If you want to read more detail about ovulation induction we have a separate booklet on our website on this subject.
Skin and hair problems
Having high androgen (testosterone) levels in your blood can lead to acne (spots) and unwanted hair growth. This may be more obvious in darker-haired people. Thinning of the hair on the head can also happen but is less common. Being overweight will make the problems worse as excess fat worsens the hormonal imbalance.
The combined oral contraceptive pill can be very useful for regulating the menstrual cycle and can help testosterone – driven symptoms. Those with levonogestrel, norethisterone or norgestimate are preferred.
The Dianette pill contains cyproterone acetate which can help with severe unwanted hair growth but it needs to be medically supervised and used for a limited time as there are other risks associated with it (blood clots in the legs / deep vein thrombosis). All OCPs provide reliable contraception. Because hair growth is slow and each hair is at a different stage of growth, it may take 6-9 months before you notice an improvement.
Cosmetic treatments such as shaving, electrolysis, waxing and laser therapy are often used for unwanted hair symptoms. All except shaving should be carried out by trained therapists.
Vaniqa (Eflornithine) is a cream which is only available on prescription which can be helpful for small areas of hair growth. It may cause thinning of the skin and a high factor sun cream is recommended if there is sun exposure.
Weight gain
Being overweight worsens the symptoms of PCOS. The condition does not make you gain weight but it can make it harder to lose weight as the body’s metabolism (rate that calories are burned compared with the rate of calorie consumption) is inefficient. Regular exercise (at least 30 minutes a day of exercise that makes you short of breath and sweaty, five times a week) will help to improve your metabolism and help weight loss.
Your eating plan should be sustainable and compatible with your lifestyle. It is sensible and advisable to eat a low carbohydrate diet with limited processed foods. Cooking fresh food from scratch with plenty of vegetables will help weight loss and reduce the risk of eating hidden calories and chemicals. When trying to lose weight and conceive we recommend cutting out alcohol altogether.
Alcohol contains a high calorie count and does not contribute anything useful to the diet.
You may find a group environment is helpful such as face to face weight loss clubs or online providers.
If you are struggling with weight loss, an appointment with a dietician or nutritionist can help identify further ways to improve your diet and focus on a natural and wholistic approach.
Weight loss drugs such as Orlistat and the injections Ozempic / Wegovy) may be offered in in General Practice to use alongside a low-fat diet and with supervision by your GP. It does not make you lose weight without other lifestyle changes at the same time.
Sometimes surgery to reduce the size of your stomach or place a band around it to make you feel fuller quickly may be helpful for those who have a larger amount of weight to lose. Surgery is very effective in the short-term but has risks and is not always available on the NHS. Many people regain weight in the longer term if they do not keep up a healthy lifestyle with regular exercise and good food choices.
What can happen in the longer term with PCOS?
If you have PCOS you have an increased risk of developing diabetes in later life. The chance of this can be very significantly reduced by leading a healthy lifestyle and maintaining a healthy weight. Long-term effects on the circulation can lead to high blood pressure, an increased risk of a heart attack or a stroke, kidney disease and blindness. Smoking will make the chance of these problems much worse.
It is important that you make sure that you have a period at least 3-4 times a year to minimise the risk of endometrial cancer. You should see your GP for advice and treatment if this is not happening. Developing endometrial cancer is still rare and can be very successfully treated when it is picked up early. This type of cancer is closely linked to being overweight and the combination of irregular periods and obesity is more dangerous.
Glossary
- Androgen: A term to include steroid hormones that promote features often related to the male.
- Biopsy: To take a medical sample of a tissue (e.g. endometrium / womb lining) for examination of the cells under a microscope to check for abnormal changes
- Cholesterol: The healthy building block for many hormones but also a risk factor for heart disease if higher than normal in the bloodstream.
- Clomiphene Citrate: An anti-oestrogen oral medication used to help ovulation.
- Combined Oral Contraceptive Pill (COCP): A combination of oestrogen and progesterone often used for contraception.
- Diabetes: A condition of abnormally high blood sugar levels related to ineffective insulin.
- Dianette: An oral combined contraceptive pill with anti-androgenic actions.
- Eggs: A lifetime supply of eggs is present in the ovary at birth. They reduce in number and quality with time. They pass on the half of the genetic instructions to the embryo/baby.
- Endometrium: The lining of the womb.
- Fertilisation: Fertilisation is when the genetic material from the egg and sperm combine to create a new and unique cell which may go on to develop into an embryo and then a baby.
- Follicle: An egg-bearing sac in the ovary.
- FSH: Follicle Stimulating Hormone causes the eggs to mature in the ovary.
- Gonadotrophins: Hormones produced naturally by the pituitary gland to stimulate the ovary to produce and release eggs e.g. FSH, LH. These drugs are produced as medicines to over-stimulate the ovary during IVF / egg freezing to get lots of eggs ready at once e.g. Meriofert, Menopur, Gonal F.
- HbA1C: A test of blood sugar levels over several weeks (high in diabetes / pre-diabetes).
- Hirsutism: The medical description of excessive hair growth.
- Insulin: A hormone produced by the pancreas to help the body to use the sugar in food to make energy.
- Letrozole: A medication used to help ovulation.
- Metformin: A medication used to improve the function of insulin in Type 2 Diabetics (those with insulin-resistance rather than those with no insulin at all which are Type 1)
- Mirena: Progestogen-containing intrauterine coil device (IUCD or IUS- intrauterine system).
- Oestrogen: This hormone is naturally produced by the follicle in the ovary as the egg is growing. Its main job is to thicken the lining of the womb for a pregnancy to implant.
- Orlistat: A prescription-only weight-loss medication which reduces fat absorption from the digestion to reduce calorie intake. It can have side-effects including fatty diarrhoea and vitamin-deficiency as some vitamins need fat to be absorbed and used by the body.
- Ovary: Stores all the eggs for your whole life and produces hormones.
- Ovulation: When an egg is released from the surface of the ovary and pregnancy is possible; without pregnancy a period follows in 2 weeks; the absence of a period signals pregnancy has occurred or ovulation did not occur.
- Ozempic / Wegovy: These are prescription – only versions of semiglutide which have been introduced to medically assist weight loss. They suppress appetite and can be effective whilst they are being used but weight may be regained after finishing a course. They are subject to strict criteria to access on NHS.
- Pituitary gland: In the head, behind the nose, the master gland which produces many hormones including those that control the ovary and testis.
- Polycystic Ovary: An ovary that has at least 20 small ‘cysts’ (follicles) on ultrasound scan.
- Polycystic Ovary Syndrome: A combination of symptoms that may include irregular periods, androgenic symptoms (acne or unwanted hair growth) and ultrasound features of a polycystic ovary)
- Progesterone: The hormone produced by the ovary after ovulation to prepare the womb lining for implantation of a fertilised egg and the start of pregnancy.
- Progestogen: A synthetic form of progesterone found in all hormonal contraceptives (pills, injections, implant, coil).
- Prolactin: A hormone produced by the pituitary gland which helps with breast milk production. Sometimes it can be made in large amounts by too many active cells and one side effect is to make the periods disappear.
- Sperm: The sperm develop in testes and continue to do so throughout adult life. They do not suffer the same deterioration with age as eggs, as they are constantly being replaced. They pass on half of the genetic instructions to the embryo / baby.
- Testosterone: The hormone mainly produced from the ovaries that may give unwanted symptoms e.g. facial hair, acne and hair thinning.
- Vaniqa: A prescription-only skin cream to treat excessive hair growth in small areas such as the face.
Informed Consent
This leaflet is provided to supplement verbal information that will be given to you by your healthcare provider (Doctor/ Surgeon/Nurse) as part of the consent process prior to your procedure. Information sharing between you and the clinician is essential to ensure that your decision to consent is fully informed. Please ask questions if you don’t fully understand or have any concerns about what is proposed. You have a right to be involved in these decisions and should feel supported to do so. Please take the time to consider what is important to you to ensure the information you receive is specific and individualised.
Other resources
Leeds Centre for Reproductive Medicine
Weight management resources online
Contact us
For all NHS appointments
Monday – Friday 08.00-17.00