What and where are parathyroid glands?
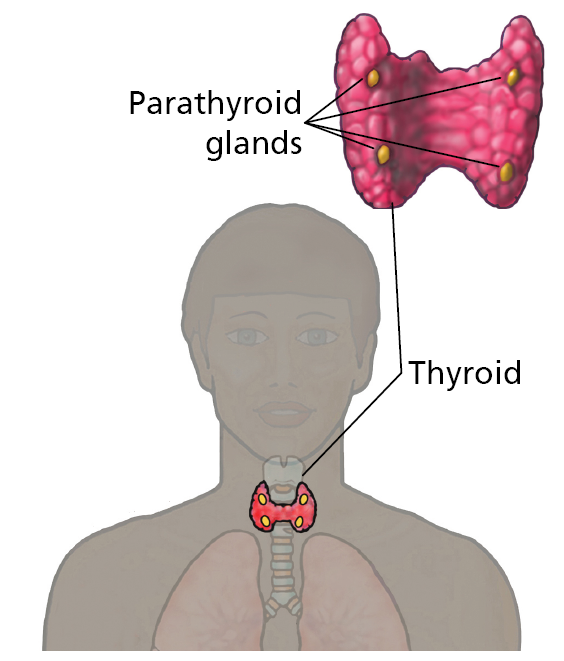
The parathyroid glands are four small glands, each normally the size of a grain of rice, found in your neck.
They lie near the thyroid gland.
The parathyroids control calcium levels in your bloodstream. If they detect low calcium levels, a hormone called PTH (parathyroid hormone) is released from the glands.
This hormone increases calcium levels in the blood by releasing it from your bones. In primary hyperparathyroidism (PHPT), one or more of the parathyroids produces excess PTH resulting in high calcium levels.
This can cause thinning of the bones (osteoporosis), kidney stones and other symptoms such as memory loss, depression, anxiety, bony pain, and tiredness.
Why do I need a parathyroidectomy?
Your surgeon has recommended removal of one or more of your parathyroid glands: this is called a parathyroidectomy. Surgery cures more than 95% of patients with primary hyperparathyroidism.
Parathyroid surgery is a common operation performed regularly with excellent success rates and relatively few risks.
What are the alternatives to surgery?
If you decide to not have parathyroid surgery, your endocrinologist doctor will monitor your calcium levels and bone density regularly.
They may try medical treatment to reduce the effect of the high PTH levels with a drug called cinacalcet. This drug will not reverse your osteoporosis or kidney stones and can have side effects such as nausea and vomiting.
What operation will I have?
If you decide to have an operation, we will request scans of your neck to try to locate if one or more than one of your parathyroids are producing too much PTH hormone. In 80% patients it is one enlarged parathyroid gland that is making excess hormone, however in 20% patients more than one (usually all the glands) are enlarged to varying degrees.
The most common types of scans are:
1. Ultrasound
Used to try to identify enlarged parathyroids within your neck as well as examining your thyroid gland.
2. Nuclear medicine scan
Also known as a sestamibi/SPECT-CT. This uses a tiny dose of radioactive isotope in combination with a CT scan to try to locate which parathyroids are overactive.
This can locate the enlarged parathyroid in approximately 60-70% of cases. The most common reason for not locating the enlarged gland in this scan is because more than one parathyroid is overactive.
The results of these scans will help the surgeon decide which operation to perform for your parathyroidectomy. The choices are:
- Focused parathyroidectomy – if the scans have localised an enlarged gland the surgery will initially concentrate on this gland and only explore this side of the neck. However, if the gland is not obviously found or there is a suggestion that more than one gland is enlarged during the operation then both sides of the neck will be explored.
- Bilateral neck exploration – if the scans are not clear on the location of the enlarged parathyroid or are suggestive of multiple enlarged glands, your surgeon will recommend a bilateral neck exploration. Using a central horizontal cut in your neck they will explore both sides to look for the enlarged parathyroid/s.
In addition, during the surgery, you may have blood tests taken during the procedure to monitor your PTH levels (intra-operative PTH monitoring). Sometimes tissue is sent to the laboratory during the procedure to confirm that the correct parathyroid has been removed.
This will help guide the surgeon on the success and extent of the surgery.
How is surgery performed?
Parathyroidectomy surgery is performed under a general anaesthetic which means you will be asleep for the procedure.
Your wounds will be closed with stitches (normally dissolvable) before you wake up.
What are the potential risks?
All surgery carries potential risks, but these are generally low in parathyroid surgery.
1. General risks
- Bleeding – there is a small risk of bleeding with any surgery. Occasionally people bleed in their neck after surgery causing swelling (haematoma). Although this is rare, if it occurs patients may need to go back to theatre to stop the bleeding.
- Infection – any surgery carries a risk of wound infection or chest infection, but these are both uncommon after parathyroid surgery.
- Deep Vein Thrombosis (DVT) / Pulmonary embolism (PE) – patients having a general anaesthetic are at risk of developing blood clots in their legs (DVT) or lungs (PE). To reduce this risk, you will be given special stockings to wear whilst in hospital and are advised to wear them at home for the first two weeks and keep active.
- Scarring – most scars in the neck heal well and are barely visible after a few months. However, some people are prone to developing thickened and bumpy scarring called keloid. If you have had problems with keloid scarring in the past, it is important to let your surgeon know before surgery.
2. Specific risks
- Damage to recurrent laryngeal nerve – the nerves that control your vocal cords are found on each side of the neck close to your parathyroid glands. During parathyroid surgery there is a risk that these nerves could be damaged which could affect your voice, swallowing and breathing. The chance of permanent damage to either nerve is very low (less than one in 100 patients). Approximately five in 100 patients will notice a temporary change to their voice that lasts a few weeks or months due to bruising or stretching of the nerve. Occasionally patients notice subtle voice changes even without evidence of nerve damage.
- Swallowing problems – following parathyroid surgery some patients may experience temporary trouble with swallowing. This usually improves with time.
- Failure to cure – there is a small risk that surgery does not cure your high calcium problem because the enlarged parathyroid cannot be found or not all the overactive glands have been removed. This happens in less than five in 100 patients.
- Low calcium – After the enlarged parathyroid/s are removed it can take a while for the remaining parathyroid/s to start working again. This can result in low calcium levels causing tingling sensations. You may have to take calcium and Vitamin D tablets after surgery for a few days or weeks until the other glands start working again. You may get tingling sensations even if your calcium levels are normal. This occurs because your body was used to higher calcium levels and will typically improve over a number of days. Rarely, you can develop long term low calcium levels that may require prolonged or life-long calcium and Vitamin D supplements.
- Recurrence – In the future there is a chance that one of the remaining glands may also become overactive and cause your calcium to rise again. You should therefore have yearly calcium checks after surgery.
What happens on the day of surgery?
Patients having parathyroid surgery are usually admitted on the day of their operation.
Before your surgery you will be contacted by the hospital to confirm the instructions for the day of admission including the time of arrival to hospital, where you need to go and when you must stop eating and drinking.
On the day of the operation, you will be seen by the surgeon who will re-discuss the surgery. If you haven’t signed a consent form before, you will be asked to complete it on the day. You will also be seen by the anaesthetist who will discuss the anaesthetic with you.
Your operation will take between 1-3 hours. After the procedure you will wake up in the recovery area, also known as PACU (Post Anaesthetic Care Unit). Here, specially trained nurses will monitor your recovery from surgery with regular checks on your breathing, heart rate and blood pressure as well as your wound. When they are happy you are well enough, you will be moved to the ward area.
You will normally be able to eat and drink once you are awake enough unless the surgeon has given specific instructions.
What happens after surgery?
Following surgery, some patients maybe discharged on the same day, if day case surgery has been discussed with you in clinic. Many patients will remain on the ward overnight for on-going monitoring. You will have blood tests that evening and the following morning to check your calcium levels. If these levels are low, you will be started on calcium and Vitamin D tablets.
The morning after surgery you will be reviewed on the ward round by the medical team.
If you were taking cinacalcet prior to surgery this will be stopped if the operation has been successful.
Wound care after discharge
Your wound is closed with a dissolvable stitch and protected with skin glue and Steri-Strips. You can have a shower after the operation and pat the wound dry. You should avoid soaking your dressings and swimming is not advised until you have been reviewed back in clinic.
The Steri-strips can be removed from your wound after a week. You may notice the ends of the stitches sticking out from either end of your wound. After two days these can be trimmed by yourself or left until review in clinic by your surgeon.
If you are concerned about any swelling or redness to the wound after discharge from hospital you can call Ward J23 (0113 206 9123) or J84 (0113 206 9184) day or night for advice. Alternatively, you can see your GP.
Blood tests after surgery
Some patients may be asked to attend Ward J23 (Level 1 Chancellor Wing at St James’s University Hospital, Leeds) a few days after surgery for a blood test to check their calcium levels. You will be advised about this prior to discharge.
If you experience any tingling to your fingers or around your mouth once you go home, it could be a sign that your calcium levels have dropped. Please contact Ward J23 (0113 206 9123) for advice. You may be required to attend the Ward urgently for a blood test to check your calcium levels.
When will I be seen in clinic?
Most patients will be seen in clinic four weeks after discharge from hospital. Sometimes the appointment date will be given to you prior to leaving the ward but it is more likely you will receive this through the post or via text message.
Please contact Ward J23 on telephone number: 0113 206 9123 if you have not been offered an appointment within four weeks of your operation.
When can I go back to work/normal activity?
Patients are generally well enough to return to work two weeks after surgery. It is advisable not to drive for a few days after surgery and to review your car insurance policy for specific limitations. If you require a sick note for work, please let the team know during your admission.
Further information
Parathyroid surgery is a common operation performed regularly with relatively few risks.
Please consider how the benefits and potential risks of surgery might affect you as an individual including your occupation and/or hobbies.
Further information can be found on the following websites:
www.baets.org.uk
British Association of Endocrine and Thyroid Surgeons
www.amend.org.uk
Association for Multiple Endocrine Neoplasia Disorders