What is sickle cell disease?
- Sickle cell disease is a condition that children are born with. It affects haemoglobin, a part of the red blood cells that carries oxygen around the body.
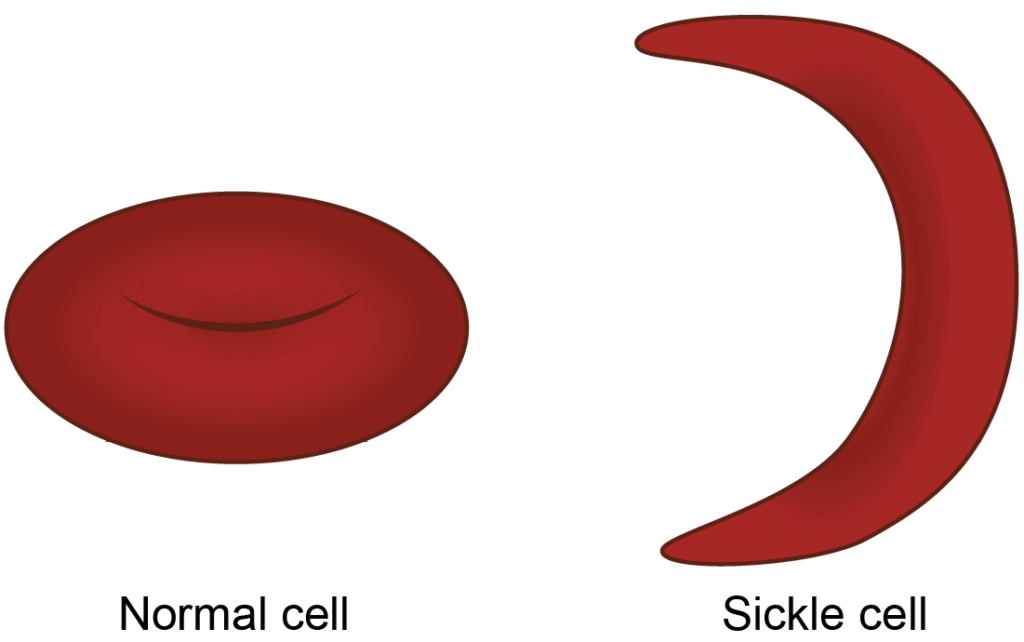
- In sickle cell disease, red blood cells can change shape. Instead of being round and flexible, they can become curved like a crescent moon or a farmer’s sickle. When this happens, the cells become stiff and sticky.
- These misshapen cells can get stuck in small blood vessels and block the flow of blood. When a blockage happens, oxygen cannot reach that part of the body properly. This can cause pain and may lead to damage in that area.
Sickle cell crisis can be triggered by:
- Dehydration
- Not having your recommended medications and vaccinations
- Being too cold or too hot
- Excessive physical exertion/stress
- Emotional stress and anxiety
Information about the sickle cell clinic
Why do I/my child need to come?
Sickle cell disease affects each child differently. Some children have frequent, severe pain and may need to go to hospital often. Others may have mild pain or no symptoms at all, especially when they are younger.
Even if your child seems well or does not have regular problems, it is still very important to attend clinic appointments. Sickle cell disease can sometimes affect other parts of the body, such as the heart, liver, brain, or lungs, and it can increase the risk of stroke. These issues are not always obvious at first.
Regular check-ups help us spot any problems early. When we find concerns early, we can start treatment sooner and reduce the chance of serious complications.
Some children may be on treatments such as hydroxycarbamide or may need regular blood transfusions. These treatments need careful monitoring, which is another important reason to attend clinic appointments regularly.
What to expect in clinic
All children and young people who are newly diagnosed, or who live outside the Leeds area, will be invited to their first appointment on a Tuesday afternoon. After this, follow-up appointments will usually take place on a Thursday afternoon for patients living in Leeds, and continue on a Tuesday for those who live outside of Leeds.
In most cases, your child will need to have a blood test at the start of the visit. The results will then be ready for the doctor to review during your appointment. Please note that the appointment time you are given is for the blood test, not the time you will be seen by the doctor.
After the blood test, there is usually a waiting time of at least 30 minutes before you are called to see the doctor. We aim to see families within an hour of the blood being taken.
Who will I see at clinic?
Receptionist
Please report to reception on arrival. You can contact reception to make or rearrange an existing appointment.
Clinical Nurse Specialist
You will have access to our clinical nurse specialist (CNS) team, who are here to support you and your child. The team consists of three nurses: Suzie Preston, Ben Sykes, and Rebecca Young.
If you need advice or support, you are welcome to contact the team by phone, text, or email.
Doctors
Your child will be seen by one of our Haematology Consultants (senior doctors who specialise in blood disorders) or by a Haematology Specialty Registrar (an experienced doctor training in blood disorders).
Social Worker
All children and young people with sickle cell disease can be referred to a social worker if needed. They can provide support and guidance with issues such as education, housing, benefits, and immigration advice, and can help connect you with other services.
Nurses / Clinical support workers
Your child may be seen by a nurse or clinical support worker to check things such as blood pressure, pulse, and oxygen levels.
Play specialists
Play specialists use play and distraction techniques to help children feel more comfortable during medical procedures and to help them understand their diagnosis in a supportive way.
If you need to speak to someone from the haematology team
In the first instance, you can contact the clinical nurse specialist (CNS) team.
Clinical Nurse Specialist
You will have access to our clinical nurse specialist (CNS) team, who are here to support you and your child. The team consists of three nurses: Suzie Preston, Ben Sykes, and Rebecca Young.
If you need advice or support, you are welcome to contact the team by phone, text, or email.
You can also contact the OWLS team, who are nurses specially trained to assess children who are unwell.
OWLS team
Nurses specially trained to assess children who are unwell.
If you are unable to reach either of these teams, please contact:
Children’s Haematology and Oncology Day Unit
Inpatient Ward
Please note
You DO NOT need to go through Accident and Emergency (A&E).
What should I do if I can’t come to clinic?
It is very important that you let us know if you are unable to attend your clinic appointment. If you inform us in advance, we can offer your appointment time to another child who needs it.
If you cannot attend, please call 0113 392 7179 between 9:00am and 4:30pm (Monday to Friday excluding Bank holidays).
Situations in which you should contact the hospital immediately
Always contact us if you or your child has:
- Pain that is not controlled with pain medication
- Chest pain even if it gets better after pain killers Breathing becomes fast or laboured
- Swollen fingers or toes
- A temperature of 38°c or above
- Is pale, lethargic or shows any signs of anaemia
- Swollen tummy and pain on left side of the stomach
- A painful erection of the penis that does not stop
Any sign of stroke (as below)
F – Facial weakness, can they smile? Has their face or
eyes drooped?
A – Arm weakness can they raise both arms?
S – Slurred Speech
T – Time to ring the hospital, this is an emergency
Guidance to help you care for your child if they have pain
When sickle cells become stuck in small blood vessels, they can block normal blood flow. This can lead to pain in the affected areas of the body. Pain is most commonly felt in the arms, legs, back, or tummy, but it can occur anywhere.
These blockages may also cause swelling in the hands and feet, stiff or painful joints, and extreme tiredness. Episodes of severe pain are known as “crises”.
Sickle cell pain can happen at home, at school, or anywhere else. Because of this, it is important that children, families, carers, and teachers understand how best to manage and respond to pain.
Managing sickle cell pain at home
Mild pain can often be managed at home. In babies and young children, it can sometimes be difficult to recognise pain. You may notice that your child is not behaving as usual, is unsettled, crying more than normal, or crying when being moved. As children get older, they are usually better able to describe where their pain is.
It is important to give pain relief as soon as your child starts to complain of pain, as this helps to control it more effectively. Waiting until the pain becomes severe can make it harder to manage. Please also ensure your child:
- Drinks plenty of fluids to avoid dehydration
- Is checked for fever. If your child has a fever, contact the sickle cell centre
- Stays warm and does not become cold
We advise you use pain medication as follows:
Remember
If your child has any of the symptoms described in the ‘Situations in which you should contact the hospital immediately’ section contact the hospital for advice.
Please note
Only give medications as directed by pharmacist’s instructions on the bottle or packet.
Use Paracetamol as soon as your child complains of pain
- If still in pain after 30 minutes add Ibuprofen (Neurofen) but continue to give Paracetamol as directed
- If pain does not ease contact the CNS team, OWLS team, day unit: or Ward L31 (if out of hours).
Regular treatment for sickle cell
Penicillin V
People with sickle cell disease have difficulty fighting infections, particularly pneumococcal infection, and they risk becoming seriously ill. By taking penicillin V regularly, you can protect your child from these infections.
The penicillin helps you to fight infection. It does not weaken their immune system.
You must give the penicillin twice every day to protect yourself, even if you think you are well.
Folic Acid
In patients with sickle cell disease, there are fewer red bloods cell than normal because sickled cells usually die after 10 to 20 days, in contrast to 120 days for normal red cells.
The bone marrow, where the blood cells are made, has to work hard to keep making more cells. Folate is needed to make red blood cells and the body’s stores of folate can run low.
Folic acid replenishes the depleted folate stores necessary to make more red blood cells.
Potential treatment options
Vitamin D
Is needed to keep bones, teeth and muscles healthy and helps you grow. A lack of vitamin D can lead to bone deformities or bone pain. We get Vitamin D from sunlight so in the UK it is very normal to have low levels.
Hydroxycarbamide (also known as hydroxyurea)
Is a medicine that is available as a liquid or a tablet and is used to reduce the frequency and intensity of sickle crisis.
Blood transfusions
If the sickle cell disease is causing significant harm we may need to use blood transfusions to dilute out the sickled red cells with healthy blood cells from a blood donor.
Admission to hospital
Sometimes it may be necessary to treat your child in hospital. Our inpatient facilities consists of three wards that provide treatment and care for children and young adults, who are being investigated or treated for cancer as well as sickle cell disease and other blood disorders.
- Ward L31 – For children between 0-13 years old.
- Ward L32 – Bone Marrow Transplant Unit
- Ward L33 – Teenage unit
Visitors are encouraged at any time up until 8pm.
Who can stay?
Due to limited space only one person can stay with your child at night time. We do encourage parents or family members to stay if possible. We do understand that sometimes this is not possible. Please let staff know if no one will be staying with your child. It is not possible for anyone under the age of 16 years to stay with your child.
What do I need to bring to hospital?
If you think there is a possibility your child might be admitted to Hospital it is a good idea to bring:
- All your child’s medication
- Change of clothes
- Towel
- Toothbrush/Toothpaste /Soap / shower gel Nappies, Nappy bags, wipes / formula etc.
Useful information
The Sickle Cell Society
Feedback
We appreciate your opinion, please let us know if there is something we can do to improve our service or fill in a comment slip and place in one of the suggestion boxes on the day unit.
Rachael Newby – Unit Manager
Patient advice and Liaison Service (PALS)
The aim of PALS is to resolve any problem or concern quickly.
We do value concerns and complaints as a means of improving the quality of our service and staff within the Patient Experience Department will be happy to guide you through the process, or answer any questions you may have.
As a point of information, if you are solely seeking compensation we are unable to deal with such requests under the NHS complaints procedure.