You will be given a separate leaflet called ‘Gynaecological Oncology Surgery – Enhanced Recovery Programme’ which will explain about what to expect when you come in for your surgery and advice for recovery at home.
If you have recently been diagnosed with endometrial cancer you may find that you are experiencing a wide range of emotions. These can include fear, anger, denial, low mood and anxiety. Reactions differ from one person to another and there is no right or wrong way to feel.
Your consultant, gynaecology specialist nurse or GP will listen to you and answer any questions you may have. They can also put you in touch with other professionals or support organisations if you wish. Some useful contact numbers are listed at the back of this booklet.
What is a hysterectomy?
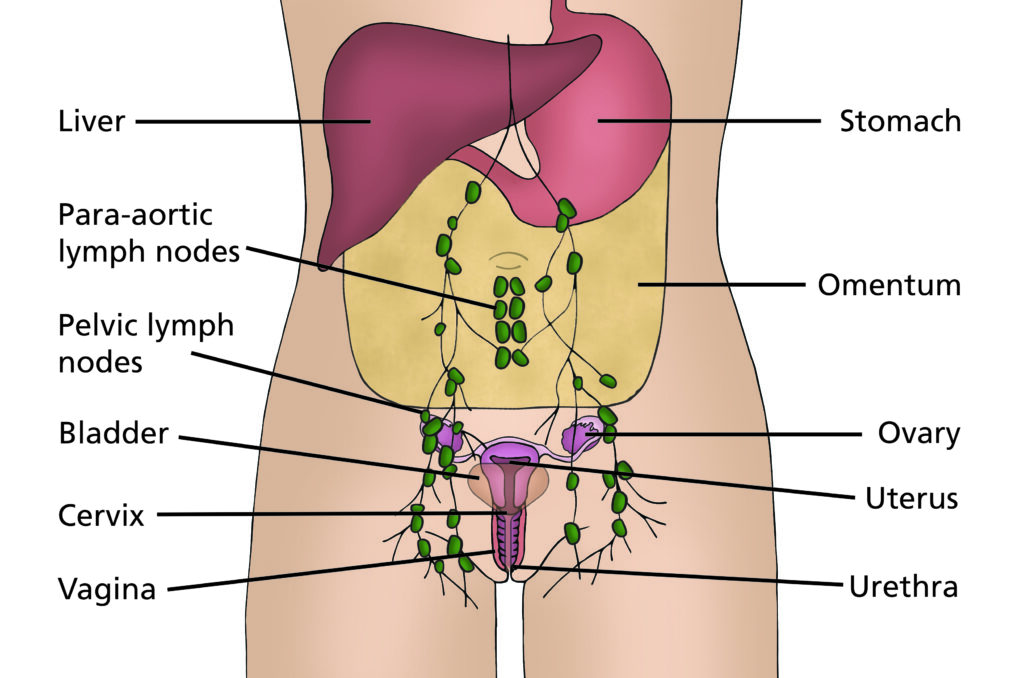
A hysterectomy is an operation to remove the womb (uterus) and the neck of the womb (cervix). The fallopian tubes and ovaries are usually removed as well (bilateral salpingo- oophorectomy). Some pelvic glands (lymph nodes) may need to be removed. A small tissue sample, called a biopsy, may be taken from other lymph nodes in your abdomen.
Your surgeon will talk with you about exactly what will be removed. (See diagram). You will have a general anaesthetic, which means you will be asleep for the entire operation. The operation may be carried out by keyhole surgery (either laparoscopically or robotically) or through open surgery (a bigger cut in your tummy).
During laparoscopic surgery, a telescope attached to a camera (laparoscope) is inserted through a small cut (incision) in your belly button to allow the surgeon to see your internal organs. Instruments are then inserted through other small cuts in your tummy and vagina to remove your womb, cervix, ovaries and fallopian tubes. Sometimes it is necessary to remove some lymph nodes in the pelvis. During robotic surgery, the surgeon sits at a computer console in the operating room and controls a robotic arm with surgical tools attached to it. The surgeon uses the arm to operate through small cuts in your tummy. A small, lighted tool with an advanced camera provides a detailed, magnified 3D view. Robotic surgery helps the surgeon make precise, flexible movements with the surgical tools.
Sentinel Lymph Node Biopsy
The lymph nodes in the pelvis are usually the first place that endometrial cancer can spread to, so a large number of women have some or all of these nodes removed during surgery. Afterwards the lymph nodes that have been removed are checked for cancer. Having lymph nodes removed can lead to a condition called lymphoedema (mentioned later as a risk of endometrial cancer surgery). To reduce your risk of lymphoedema you may be offered a sentinel lymph node biopsy which is a way of checking lymph nodes for cancer without removing all of them.
The sentinel node is the first lymph node that fluid drains to from the womb, so it is the first node the cancer could spread to. If the sentinel nodes are free from cancer, it’s likely that no further lymph nodes have cancer in them and no more need to be removed. To find the sentinel node(s), the surgeon injects a green dye into the neck of the womb (cervix). This is done at the start of the operation when you are asleep. The nodes that take up the dye are the sentinel nodes. These nodes are removed and tested for cancer cells. If the sentinel nodes don’t contain any cancer cells, then no further lymph nodes are removed. However, if there are cancer cells in one or more sentinel nodes then more treatment will be required.
What happens if the sentinel nodes are not found?
If the sentinel nodes are not found, then all the pelvic lymph nodes will need to be removed from the side where the node has not been identified. The chance of not finding the sentinel lymph node is around 15-20%.
Will I have a scar?
es, although it will fade. If you have open surgery, then the surgeon will make either an ‘up and down’ cut (known as a midline incision) or a cut across the top of your pubic hairline (known as a ‘bikini line’ incision). The wound will usually be closed with dissolvable stitches but sometimes stitches and/or staples that need removing are used. The area around the scar will feel numb for a while after the operation but sensation will usually return over time. If you have laparoscopic or robotic surgery then you will have 4-5 small cuts in your tummy closed with dissolvable stitches.
Incision
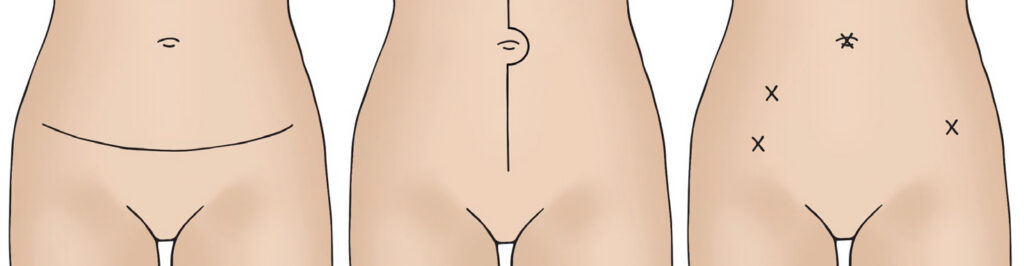
Left illustration shows a horizontal ‘bikini line’ incision in abdomen.
Middle illustration shows a vertical incision in abdomen from just above belly button down to pubic area.
Right illustration shows four little crosses on abdomen to show where laparoscopic and robotic incisions are made.
Please note
There is a minimally invasive surgical procedure available for some women who have an early stage Womb cancer – Transvaginal Natural Orifice Transluminal Endoscopic Surgery, called vNOTES for short. Prior to the procedure you will have a general anaesthetic and your surgeon will remove the womb, fallopian tubes, ovaries and cervix. Surgery and removal is all done via your vagina, there will be no cuts to your abdomen therefore no scar. It is likely that you will able to go home on the same day, however, you will still have to follow the recovery advice in this booklet.
What are the risks of a hysterectomy?
All surgery carries some risks and your surgeon will explain the risks of a hysterectomy to you before you sign your consent form. This form confirms that you agree to have the operation and understand what it involves. Possible risks and complications are:
- Problems caused by having a general anaesthetic; for example, you may feel sick afterwards. It is also possible to have an allergic reaction, although this is rare. Please tell your doctor about any allergies you have.
- Heavy bleeding during or after the operation; this may need to be treated with a blood transfusion.
- Infection; this would be treated with antibiotics.
- Damage to your bowel, bladder or ureters (the tubes that carry urine from the kidneys to the bladder) during surgery – this would be repaired during your operation.
- A blood clot in the leg (deep vein thrombosis) which can sometimes lead to a blood clot in the lungs (pulmonary embolus); moving around as soon as possible after your operation can help to prevent this. You will be given surgical stockings (known as TEDS) to wear and injections to thin the blood which both help to reduce the risk of blood clots. You may continue to have these injections for up to four weeks.

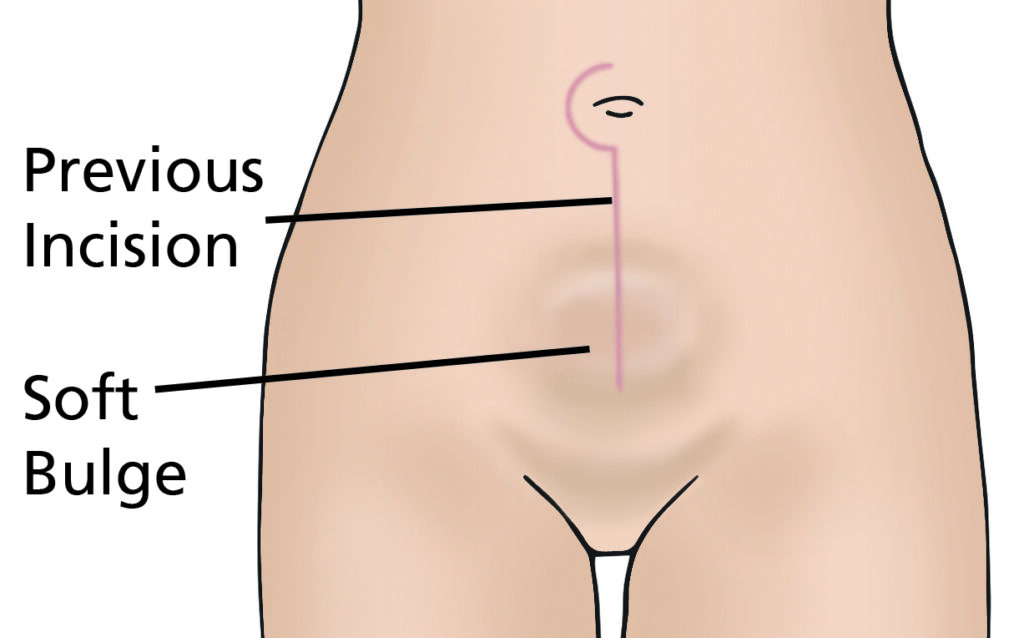
- Incisional hernia; a weakness in the wound, allowing tissue or bowel to push through and appear like a bulge. Incisional hernias can develop months or years after surgery and are repaired by another operation.
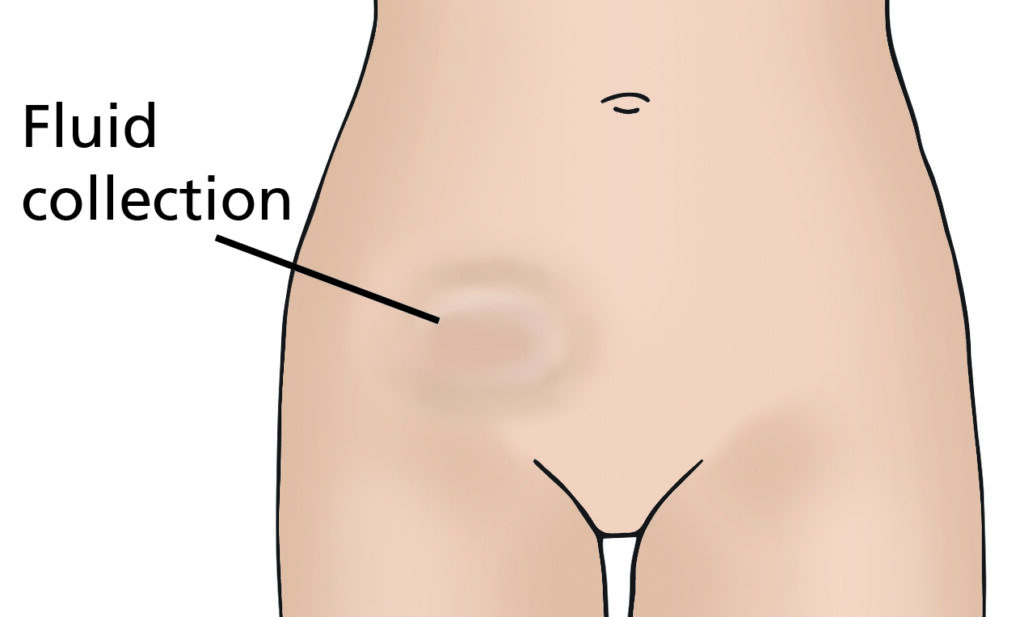
- Lymphocyst; this is a fluid collection at the site where lymph nodes have been removed. It is often naturally reabsorbed by your body but may require draining if large or causing you discomfort.
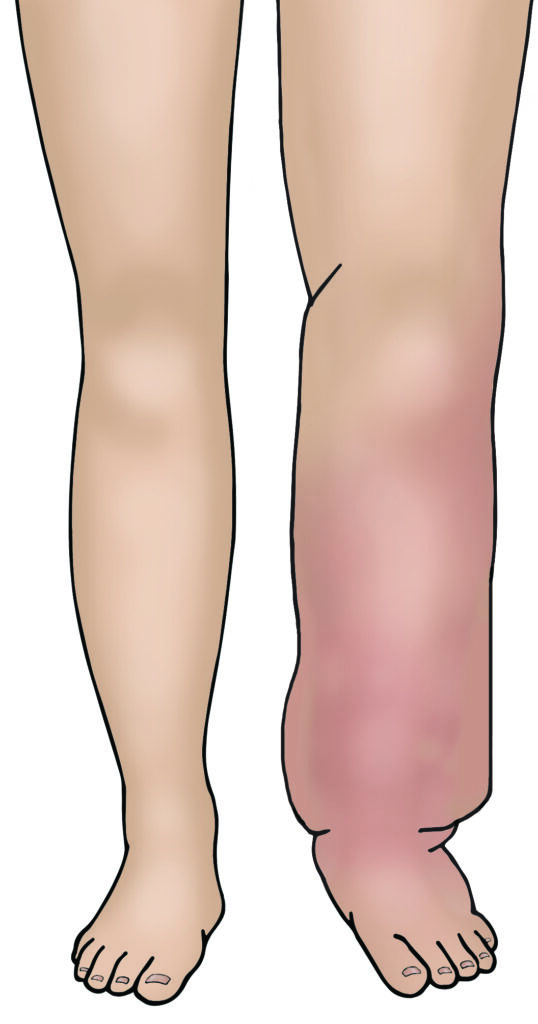
- Lymphoedema; if you have some lymph nodes removed during surgery there is a small risk that in the future your body will find it harder to drain fluid from your legs and lower body. This causes swelling of the legs and lower body known as lymphoedema. If you develop this problem then you can be treated by a lymphoedema specialist. You can discuss this further with your gynaecology specialist nurse or doctor. There is also a booklet you can read that can give you more information.
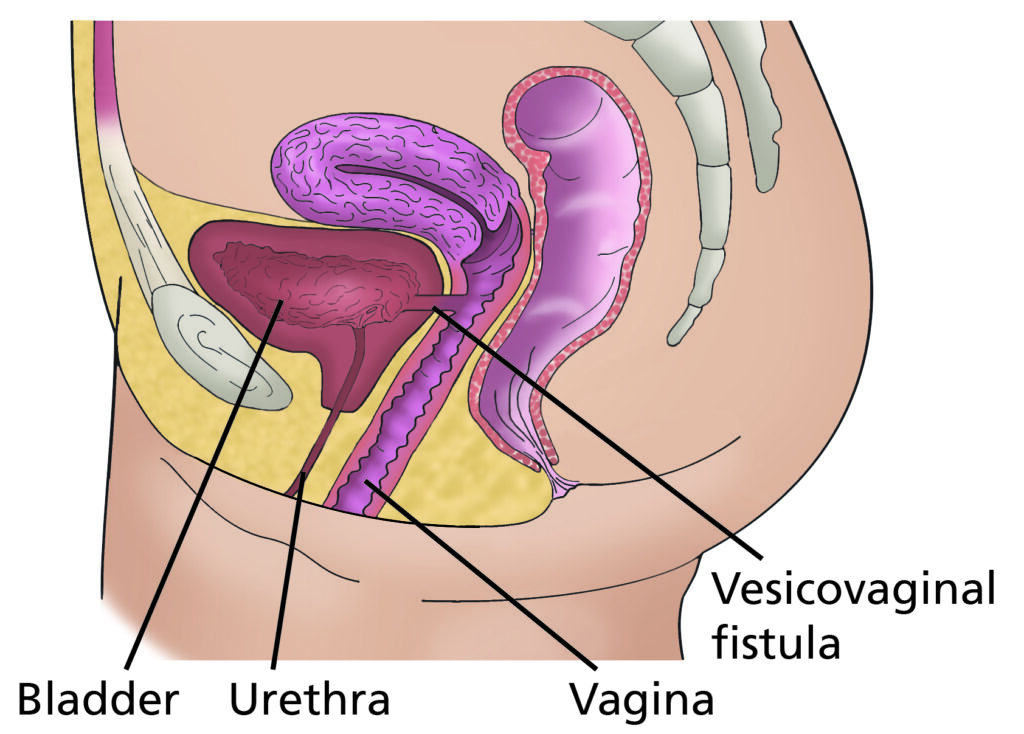
- A vesicovaginal fistula is a hole between the bladder and vagina. It allows urine to pass from the bladder to the vagina.
- A rectovaginal fistula is a hole between the rectum and the vagina. It allows faeces to pass from the rectum to the vagina.
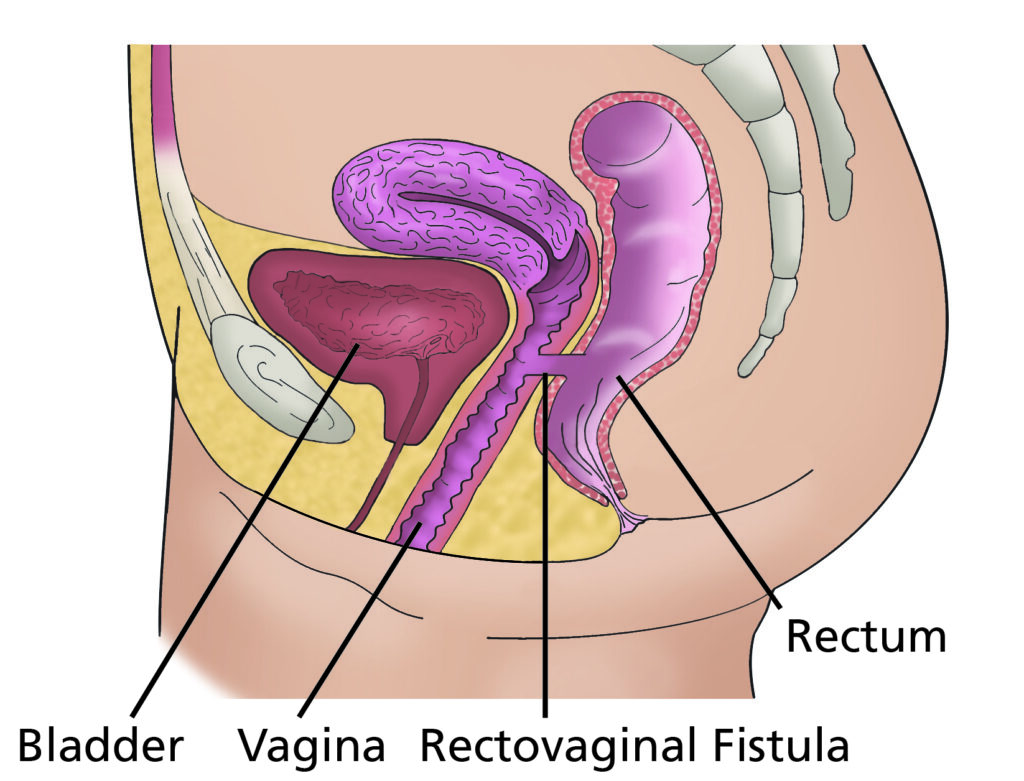
Fistulas can be repaired but sometimes it will involve another operation.
What else may happen as a result of surgery?
Your bladder may take some time to begin working properly again. Some women have a loss of feeling in their bladder and therefore do not know when their bladder is full. This may take some time to return to normal. During this time you need to go to the toilet regularly to empty your bladder. Some women find that their urine stream is slower so it may take longer to pass urine. This usually improves as your body recovers from surgery. Rocking gently backwards and forwards or side to side whilst sat on the toilet can help to fully empty your bladder.
Your bowels may take some time to begin working properly again. Some women have a sluggish bowel for a number of days after surgery which can cause you to feel sick until it starts to work again. If this happens then you will be advised to walk around the ward as much as possible to stimulate your bowels to work. This can be difficult if you are feeling unwell but it is important to do so to speed up your recovery. We will also give you anti-sickness medication. Passing wind is a good sign that your bowels are starting to work.
Trapped wind and wind pain is very common after surgery. Walking around as much as possible can help relieve this. You may find that peppermint tea and/or peppermint capsules helpful which are both available on the ward. Wind usually starts to improve once you are having your bowels opened.
What about losing my fertility?
At any age, having your ovaries and/or womb removed can affect the way you feel about yourself. A hysterectomy will prevent you from getting pregnant.
The loss of fertility can have a huge impact on you if you have not yet started or completed your family and you have an operation that takes that choice away. You may want to make sure that you have explored all your options. It is important that you have the opportunity to discuss this and your feelings with your specialist nurse before your operation. They will continue to offer you support when you are recovering from the operation. Advice is also available from our specialist fertility team.
Will I need Hormone Replacement Therapy (HRT)?
The use of HRT for women who have been diagnosed with a gynaecological cancer is not straightforward. A number of different factors influence whether or not HRT is recommended. Please discuss the options available to you with your consultant or specialist nurse.
Should I continue to have cervical smears?
No, cervical smear tests are usually not necessary after this operation, as your cervix will have been removed. However, it is important to come for regular examinations in the outpatient clinic.
Is it normal to feel weepy or depressed after my operation?
Yes. It is a very common reaction to the operation. If these feelings carry on when you leave the hospital, you may wish to discuss them with your GP or specialist nurse.
There are also local and national support groups that you can contact. Details are given at the end of this page.
Is there anything I should do to prepare for the operation?
Make sure that all of your questions have been answered and that you fully understand what is going to happen. You are welcome to visit the ward and meet the staff before you are admitted to hospital – ask your specialist nurse or
pre-assessment nurse to arrange this.
You should eat a balanced diet and if you feel well enough, take some gentle exercise before your operation, as this will help your recovery afterwards.
Your GP, practice nurse or the doctors and nurses at the hospital will be able to give you further advice about this.
Before you come into hospital for your operation, try to organise things ready for when you come home. If you have a freezer, stock it with easy to prepare food. Arrange for relatives and friends to do your heavy work (such as changing your bedding, vacuuming and gardening) and to look after your children, or other dependants if necessary. Arrange for somebody to take you home from hospital when you are discharged. If you think you may have problems coping at home, you can discuss this with the nurses on the ward
When can I go home?
If you have had keyhole surgery you will usually be able to go home one to two days after your operation. If you have had your operation through a cut in your tummy, you will usually be able to go home three to five days after your operation. This depends on your individual recovery, how you feel physically and emotionally and the support available at home.
If you need hospital transport for your discharge home, please let a member of staff know well in advance.
Will I need to visit the hospital again after my operation?
Yes. It is very important that you attend any further appointments arranged for you whether this is at your local hospital or in Leeds.
Everything that is removed during your surgery will be sent to the histology laboratories for testing. These tests take around 3- 4 weeks. You will be brought back to clinic to discuss these results with your consultant, where you will be told the grade and stage of your cancer. The staging is a process of investigations which may be used to determine type/size of the tumour and if there is any spread. Staging is important to help decide further treatment options. The grade of a cancer depends on what the cells look like under a microscope. In general, a lower grade indicates a slower-growing cancer and a higher grade indicates a faster-growing one.
If the cancer has not been fully removed or if cancer is found in your lymph nodes, you may be referred to a clinical oncologist for consideration of further treatment.
Useful Numbers
For queries regarding your admission please call the relevant secretary.
Secretary to Mr Broadhead, Mr Nugent and Mr De Jong
Secretary to Dr Kaufmann, Dr Thangavelu and Mr Theophilou
For advice on any medicines you have received from the hospital call:
Medicines Information
Gynaecological Cancer Surgery Website
On our website you will find information about our team, what we do, information leaflets and videos.
Visit the Gynaecological Cancer Surgery websiteContacts
For advice please call your Clinical Nurse Specialist (CNS) or Ward J98 (Open 24/7).
Ward J98 – Gynaecological Cancer Ward
You can ring anytime.
Airedale CNS team
Bradford CNS team
Calderdale CNS team
Harrogate CNS team
Leeds CNS team
Mid Yorkshire CNS team
York CNS team
If your nurse specialist is not available then please leave a message on the answering machine and they will ring you back. Please note this may not always be the same day. In an EMERGENCY please attend your nearest Accident and Emergency Department.
Local Support Services
Leeds Cancer Support
Leeds Cancer Support complements care provided by your clinical team. We offer access to information and a wide range of support, in a welcoming environment for you, your family and friends.
We can be found in the information lounges in Bexley Wing and also in the purpose built Sir Robert Ogden Macmillan Centre (behind the Thackray Medical Museum).
The Sir Robert Ogden Macmillan Centre
This centre offers a variety of free health & wellbeing and supportive therapies for patients, their family members and carers. These include hypnotherapy, mindfulness coaching, acupuncture (for hot flushes) and pilates.
Maggie’s Centre
If you or someone you love has cancer you may have lots of questions. Maggie’s is a warm, welcoming place where you can meet people who are experiencing similar things to you.
You may also be able to find support groups specific to your needs and get advice and information from their professional staff.
You don’t need an appointment and all support is free.
National Information and Support
Macmillan Cancer Support
They also offers an interpretation service. When you call, just state in English, the language you wish to use.
The Eve Appeal
Information about all gynaecological cancers.