This leaflet aims to help you and your family understand more about your Total Pancreatectomy (the removal of all of your pancreas) to treat chronic pancreatitis, cysts or a cancer of the pancreas.
It will be given to you in addition to the information you will receive from your surgeon and their team.
We realise this may be an anxious time for you and your relatives. We hope that by providing accurate information you will know what to expect before and after your operation and feel better prepared.
This booklet will explain:
- What the pancreas does.
- Why you need an operation.
- What the operation involves.
- Preparing for and recovering from the operation.
- The potential risks of the operation.
- Preparing to go home.
St James’s University Hospital is a specialist regional centre for surgery on the pancreas. You will be cared for by a healthcare team who are experienced in treating people having this type of operation.
The Pancreas
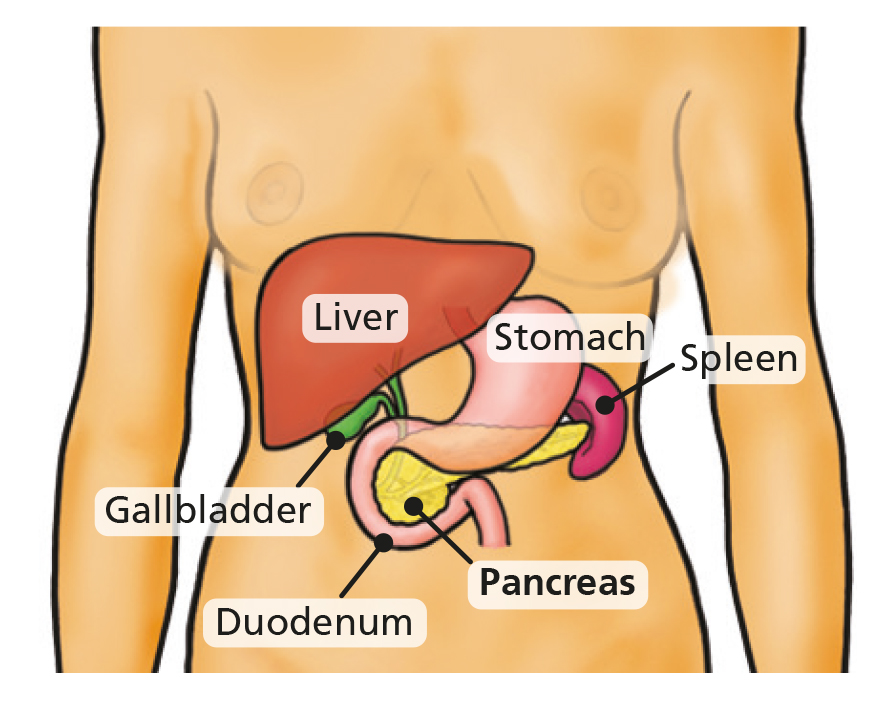
The pancreas is part of the digestive system. It lies at the back of the upper abdomen in front of the spine and behind the stomach. It is about 20cm (8 inches) long. It has four sections: the head, neck, body and tail.
The pancreas produces:
- Pancreatic juice (enzymes) to help digest your food.
- Insulin to control blood sugar levels.
Total Pancreatectomy
For chronic pancreatitis, large tumours, cysts, multifocal (more than one) or some specific types of pancreatic cancer it may be necessary to remove the whole pancreas.
What the surgery involves
A total pancreatectomy is an “open” procedure – this means you will have a long incision on your stomach and will have a scar afterwards.
The operation involves the surgeon removing the entire pancreas, the duodenum, part of the stomach, the gall bladder, the spleen and some of the surrounding lymph nodes.
First, your surgeon will carefully remove all of your pancreas gland, the first part of your small bowel called the duodenum, your spleen and your gallbladder. The team then join the end of your stomach to a loop of your remaining small bowel. Finally, your surgeon joins your bile ducts on the same loop of small bowel. This allows food and the digestive juice made by your liver known as bile to pass in to gut and for food to be digested.
Pancreas before surgery

After surgery

As your pancreas is removed your digestive system will be affected and you will be diabetic.
As your spleen is removed you will need to take lifelong antibiotics to prevent infections.
Preparing for your Operation
Before your operation it is important that you stay as fit and well as you can. Taking regular exercise and eating nutritious food is very important. If this is difficult for you please ask for advice from your doctor or specialist nurse.
If you smoke you should try to stop as soon as you can. Stopping smoking, even just a few weeks before your operation, will make a big difference to your recovery and reduce your risk of developing complications.
Pre-assessment
To prepare for your surgery you will need some routine tests to make sure you are well enough for your operation. These tests are usually done in the pre assessment clinic a few weeks before your operation.
You will receive an appointment to attend this clinic or you may have to attended the clinic straight after your outpatient appointment.
This is a good time to start thinking about what support you may need when you go home after your operation. This is especially important if you live on your own. Are there friends, family or neighbours that may be able to help out with shopping, cleaning and cooking for a while until you are feeling stronger?
The nurses in pre-assessment will advise you about the Trust’s infection prevention policy.
Coming into hospital
You will be admitted to hospital the day before your operation. A nurse and a doctor will talk to you and answer any queries you or your family may have. You will be given an identification band to wear on your wrist. If you have an allergy please let the staff know and you will be given an allergy band to wear as well.
You will usually be visited by an anaesthetist who will explain about the general anaesthetic and how your pain will be controlled following your operation.
Consent
A consent form is a document which we will ask you to sign to say that you agree to have the surgery. Your doctor will explain the details of your surgery to you and the risks associated with it.
Please do not be afraid to ask questions since it is important for you to fully understand the operation. If you have any questions about the operation it can be useful to write these down so you can remember the questions when you see the doctor.
The day of your operation
You will need to stop eating and drinking several hours before your operation. The nursing staff will advise you of the exact time (usually around midnight).
You will be given a hospital gown to put on. You will be asked to wear elasticated stockings as they help to prevent a deep vein thrombosis (blood clot) forming during the time you are less mobile.
You will also be given a small daily injection to help thin your blood after surgery, which needs to be continued for 28 days after the operation.
Recovering from the operation
You will be admitted either to the pancreas ward, J82 in Bexley Wing or to the High Dependency Unit (HDU) following your operation. If you go to HDU, this will usually only be for a day or two for closer monitoring. While you are there your family will be able to visit. You will be awake and able to talk when you go to the ward or HDU but you may feel sleepy. You will be attached to various tubes and monitors, which the nurses will explain to you.
These may include the following:
Intravenous Fluids (Drip) – these are given through a tube inserted into a vein in your neck and/or arm to make sure you have enough fluid until you can drink again. Certain medications may be through this tube. Your Consultant will decide when it is safe for you to begin to drink.
Naso-gastric (NG) tube – this is a thin tube that goes up your nose and down to your stomach and is placed whilst you’re having you’re operation. This will drain away any stomach contents to avoid sickness. This will be attached to a bag to allow it to drain freely and will usually be removed a couple of days after your operation.
Naso-jejunal (NJ) feeding tube – if your doctor thinks you need one, you may have a feeding tube. This tube goes up your nose and passes into your small bowel. This is used to give you liquid feed containing essential nutrients. It will stay in place until you are able to eat again.
Oxygen therapy – you will need oxygen for a number of days following surgery. Nursing and physiotherapy staff will advise you on some deep breathing exercises which will help to prevent you developing a chest infection.
A surgical drain – this is a thin plastic tube that may be inserted into your abdomen during your operation. It drains fluid away from the area of your operation. The removal of this drain will be graded by the samples the nurses take from the drain.
Catheter – during your operation a catheter will be inserted into your bladder. This is a tube which drains your urine into a bag, so we can measure how much urine you are passing. The catheter will stay in place until the surgical team advise for this to be removed.
Once you are well enough you will be able to return to the ward.
Pain control
Your anaesthetist will speak to you before the operation about how to control your pain.
PCAS (patient controlled analgesia system) – you may be given this strong painkiller through your drip. You will be given a button to push which, when pressed, will give you a dose of painkiller. There is a safety lockout system which means you cannot overdose however many times you press the button. This system is usually used if you do not have an epidural.
Oral medication – once the PCAS is removed you will be given regular painkilling tablets. Our aim is for you to be as pain free as possible. If you experience pain please inform your nurse. The more comfortable you are, the more mobile you will be. The more mobile you are, the less likely you are to develop a chest infection or blood clot in your leg.
Wounds
Your wound will be checked regularly by the nurse for signs of healing and infection. A dressing will be applied where necessary. Your stitches or staples are likely to be removed around 10-14 days after your operation. This may be whilst you are still in hospital or if you have gone home, by the practice nurse at your doctor’s surgery or district nurse. Sometimes we use dissolvable sutures, or glue, that do not require removing and these will dissolve over time.
Personal care
After your operation you may need some help with washing and changing your clothes. You will be encouraged to take part in your care more as you feel stronger and have fewer tubes attached. If you have any special needs or are worried about this aspect of your care please speak to your nurse.
Eating and drinking
You will not be allowed to eat or drink for a few days after your operation. This is to make sure the new joins inside your abdomen are allowed to heal.
The nurses will help you to brush your teeth and tongue and use mouthwash to prevent your mouth and lips becoming dry and sore.
You will firstly be allowed sips of water which will gradually be increased until you can drink freely. You will then be given a light diet.
Potential risks and long term effects of surgery
As with all surgery, problems can happen during or after your operation. This can usually be dealt with by your doctor. The following information is specific to the type of surgery you are having.
It is important to remember that the majority of patients recover well from this major operation but complications can happen. Unfortunately 1 in 3 patients having this operation will experience some kind of complication. Most of the complications can be dealt with easily. These include chest infection, wound infection or a urinary tract (waterworks) infection.
More serious complications include:
- thrombosis in the legs or lungs.
- heart attack or stroke.
The assessment you have before your operation help us to identify patients who are more at risk of these complications. For all patients we have standard practices to reduce these risks. For those at increased risk you will be assessed by an anaesthetist and medications changed as necessary.
Serious complications can arise from the area of the operation and can include the following:
- Bleeding – some bleeding is expected during your operation and occasionally a blood transfusion is needed. Bleeding can happen after surgery but this is rare. This can be managed either by the surgeon in theatre or by the radiologist in the x ray department.
- Infection – some patients may develop an infection such as wound, chest or urine infection. Infections can be treated promptly with antibiotics if necessary.
- Digestive juice leak – any of the new joins have the potential not to heal properly. If that happens digestive fluids can leak out between the stomach and the bowel or bile ducts and the bowel and make you unwell. If this occurs it may delay your recovery and keep you in hospital longer than expected. It is usually treated by draining the fluid requiring further surgery or a drain inserted in radiology department.
Long term effects
Diabetes
When your pancreas is removed your body will not produce enough insulin to control your blood sugar levels. Initially after your operation you will be connected to a continuous insulin pump, in the form of a drip. During this time your blood sugars will be checked every 2 hours. Once you are able to eat and drink you we will then be able to start on a new insulin regime. You will be seen by the Diabetes specialist team who will provide education and support how to control your blood sugars.
You will be given information on how your diet may need to change, how to take the necessary medication, and how to check your blood sugars.
Pancreatic insufficiency
Without your pancreas you will not be able to digest your food without taking a pancreatic enzyme replacement. These come in a form of capsules that need to be taken with every meal and snack to allow you to absorb the nutrients from your food.
The doctors, dietician and nurses will explain how to take these. Your Consultant may start these before your operation.
Absent spleen and gallbladder
The spleen is important in helping fight-off infections you come in to contact with. Without your spleen you will also have to take a low dose antibiotic every day and will need to be vaccinated against certain infections. The vaccinations are usually given two weeks before the operation or two weeks after the operation, followed by a booster vaccination a month later. Whenever you see a doctor, you should tell them you no longer have a spleen.
Not having a gallbladder anymore shouldn’t cause you any problems and you are unlikely to notice it has been removed.
The risks and benefits of the operation
There is a very small risk of dying from this operation. Around 3 in every 100 patients will die as a result of having this operation. This of course means that 97 out of every 100 people do not die. Your consultant will discuss your own risk of having the surgery. It is important to remember that in general the surgery is performed for a diagnosis of cancer and therefore the risk of not having surgery has to be balanced against the risks of the operation itself.
Going home
It is important that you and your family, together with the nursing staff make plans for home as early as possible. This helps to make sure you do not have to stay in hospital longer than necessary. You and your family may have concerns about how you will manage and what to do if any problems arise. Please discuss any concerns you have with your doctors and nurses who will offer you help and advice.
It is hoped that the following information will inform you of what you can expect when you go home.
Tiredness
By the time you go home you will be able to walk around your home and get yourself washed and dressed. You will feel tired however. Recovery from this operation is slow and may be 3-6 months before you feel back to your normal self. During this time you will gradually become stronger.
If you live alone and are concerned about who will help you with shopping, cleaning and cooking etc., please speak to the ward staff who will discuss options with you.
It is important you take plenty of rest during the early days and weeks at home. You may feel you benefit from a sleep during the day. Increasing your level of activity as the weeks go by is important. Taking a short walk each day, increasing the distance gradually will have positive benefits.
Eating
By the time you are ready for home you will be eating and drinking again. Your appetite is likely to be greatly reduced and you may feel full very quickly.
You will be advised to eat small meals and snacks but often throughout the day rather than three large meals.
It is likely if you eat too much you may feel abdominal discomfort and bloating. You will soon learn how much food you can eat at any one time and you will adjust to smaller meals but more often during the day.
Your doctor may have prescribed you medication to help absorb your food. It is important that you take this medication just as you are about to eat your food. This will enable it to work more effectively. Most people do lose weight following this type of surgery, please be reassured that as your appetite improves your weight loss will stop and you will slowly start to gain weight.
Pain
Your wound may feel tender for a period of time after going home. Please make sure you take your painkillers as needed to keep you comfortable and be able to move around freely.
Bowels
Normally it takes a few weeks for your bowels to settle down into a regular pattern. Occasionally your painkillers may make you constipated. Please contact your GP or nurse specialist if you are concerned.
Returning to normal
It is understandable to want to know when you will feel back to normal after your operation. You may want to know when you can resume work, start driving or go on holiday.
Although we know that recovery from this surgery takes several months, the rate of recovery is different from person to person and it is difficult to predict how long this will take in your case.
Follow up
Following your operation you will return regularly for check- ups at the hospital. Your first clinic appointment will be about four weeks after going home. This will give you the opportunity to discuss any concerns or queries you may have. At the follow up appointment we will explain the pathology results found at the time of surgery and discuss the options for your next stage of treatment/after care.
Contact numbers
Pancreatic & liver nurse specialists
Mr Smith’s secretary
Mr Young’s secretary / Mr Pine’s secretary
Ward 82
High Dependency Unit Ward 81
Useful organisations and contact numbers
Leeds Cancer Support
Complementing care provided by your clinical team, offering access to information and a wide range of support, in a welcoming environment for all. We can be found in the information lounges in Bexley Wing and also in the purpose built Sir Robert Ogden Macmillan Centre.
Contact numbers for Leeds Cancer Support
Information Lounge Level -2 Radiotherapy Department
Open from 8.00am – 6.00pm
Information Centre Level 1 Outpatients Department
Open from 10.00am – 4.00pm.
Sir Robert Ogden Macmillan Centre
Open from 10.00am – 4.00pm.
Maggie’s Centre
A warm, welcoming place where you can meet people who are experiencing similar things to you. Next to the multi storey car park.
Open Monday to Friday 9.00am – 5.00pm.
Macmillan Cancer Support
Open 9.00am to 6.00pm Monday to Friday. A textphone service for deaf and hard of hearing people is also available.
Textphone: 108001 0808 808 0121