This leaflet aims to give you an overview of transcatheter (keyhole) stent placement for Coarctation of the Aorta.
Transcatheter (keyhole) stent placement for Coarctation of the Aorta
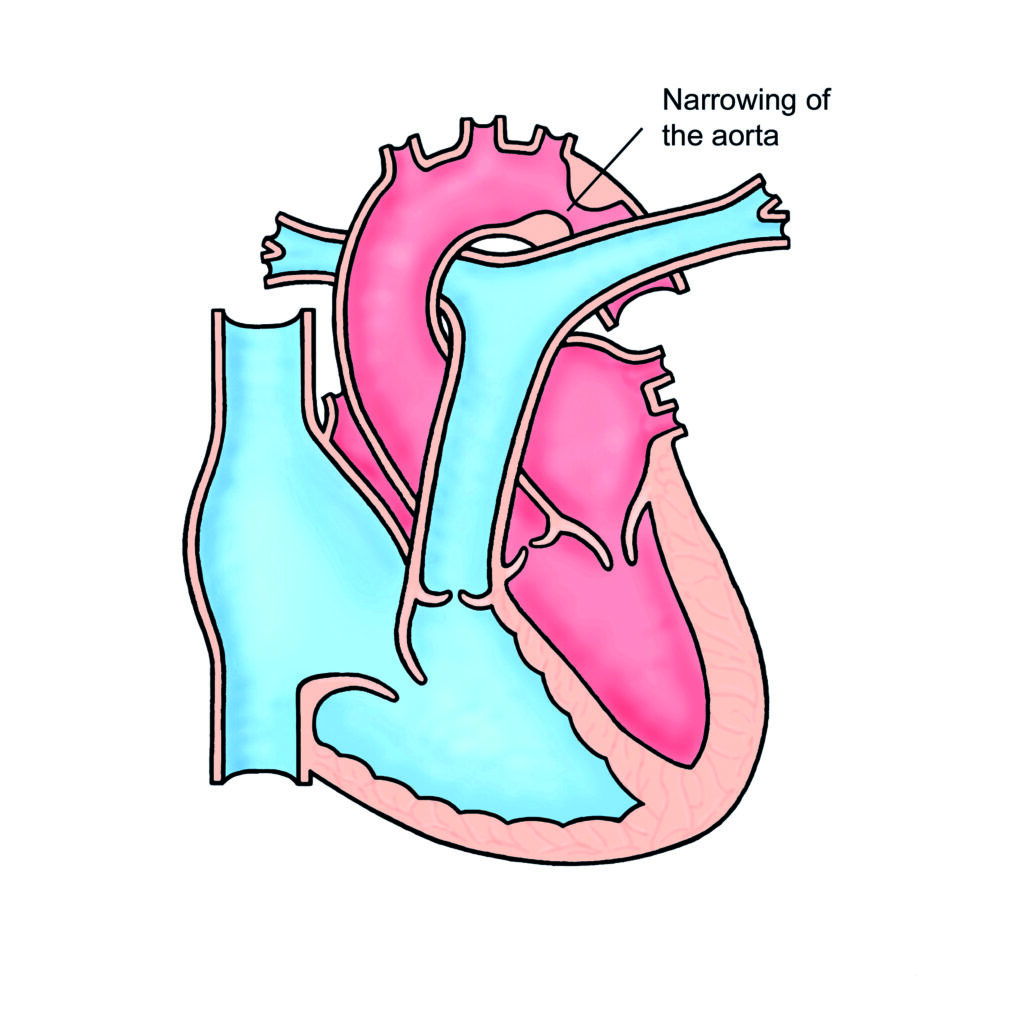
Coarctation of the aorta is a narrowing in the main blood vessel in the body (the aorta). The aorta carries oxygenated blood from the heart to the rest of the body. The narrowing acts like a dam, causing high blood pressure in the top half of the body and reducing blood flow to the rest of the body.
This condition is usually picked up in childhood but is occasionally diagnosed for the first time in adult life, usually because someone is found to have high blood pressure.
Coarctation of the aorta
Why does my coarctation need treating?
Unrepaired narrowings (coarctations) place strain on the main pumping chamber of the heart – the left ventricle, and leads to high blood pressure. Untreated, both of these complications can significantly shorten someone’s life. High blood pressure is related to stroke and heart attack.
What are the options for treatment?
Many coarctations are picked up in early childhood where surgery is the best treatment option. In teenage and adult patients some narrowings can be technically very difficult to repair using surgical methods and can require lengthy operations.
In some patients, the narrowing is not discovered until they are much older or re-narrowing can occur due to scarring at the site of a previous operation. In these patients, it is possible in some (but not all) cases to stretch the narrowing using a keyhole technique.
Most patients who are diagnosed with a coarctation in adulthood will be offered a stent procedure to open the narrowing. You may need a CT or MRI scan to see if you are suitable for this.
What are the advantages of keyhole treatment?
The main advantage of the keyhole technique is that it avoids an operation which leaves a scar on the side of the chest that can be painful afterwards for a number of weeks. The keyhole technique is performed as an overnight procedure whereas surgery requires a short stay on the intensive care unit followed by about a week in hospital.
There are other less serious complications of a major operation and a hospital stay (wound infections, potential for blood clots in the leg etc). Which are avoided by the keyhole approach.
Keyhole treatment is now generally considered first line treatment for adults with coarctation of the aorta.
What are the risks of keyhole treatment for coarctation?
- The risk of death during the procedure is less than 1 in 100.
- Migration (movement) of the stent (metal cage) can occur during the procedure (2%). Generally, a migrated stent can be safely repositioned but in some cases may require an operation to remove it.
- Aneurysm (blow out of the blood vessel) can occur and can require further treatment.
- Stroke can occur in less than 1% of patients.
- Damage to the leg artery (which is used to put the stent in) requiring treatment occurs in approximately 4% (1/20) patients.
How is the procedure performed?
The procedure is performed under general anaesthetic. A tube is inserted into the artery at the top of the leg and pictures are taken. A balloon with a metal cage (stent) on the outside is inserted into the tube in the artery and positioned across the narrowing. The balloon is inflated and the stent stays in position holding open the narrowed area.
After the procedure the tubes are removed and the hole in the artery is closed using an automatic stitch device.
Coarctation of the Aorta – Treatment Information Video
Coarctation of the Aorta – Treatment
In this video, we explain how coarctation of the aorta can be treated. A separate video explains what coarctation of the aorta is. Coarctation can be treated either by surgery or in a keyhole technique. In general, surgery is used in babies and young children, and in older children and adults, surgery is most frequently performed by opening the chest from the left side, although sometimes the chest has to be opened from the front through the breastbone. A number of different techniques are used to repair a coarctation surgically.
The most common involves removing the narrowed section of the aorta and sewing the two ends together. This is called an end-to-end repair. An alternative technique is called subclavian flap repair. The left subclavian artery is the blood vessel that supplies blood to the left arm. The subclavian artery is cut open up and used to enlarge the area around the coarctation. The left arm still manages to get an adequate blood supply from other blood vessels, although the pulses in the left arm may be difficult to feel in patients who have had a subclavian flap repair. A further type of repair involves sewing in a patch of material around the coordinate to enlarge the narrowed area.
The final type of surgical repair, which is only rarely performed and often for longer narrowings, involves removing the narrowed section of the aorta and replacing it with a tube called an interposition graft. Treating coarctation with the keyhole method involves inserting a tube into an artery in the groin while the patient is asleep. Through this tube, a metal cage called a stent is positioned within the narrowed area and expanded with a balloon. The narrowed area becomes wider, and the stent helps to keep it open occasionally. Just a balloon is inflated to widen a narrowing without using a stent. The keyhole technique can be used to treat coarctation that either has not been treated before or that has previously been treated by surgery. If some narrowing remains or has reoccurred, however a co-occupation has been treated, lifelong follow-up is important.
What happens after the procedure?
If there are no problems, you will go home the following day. Your leg may be sore for a week and there may be some bruising. Follow up will be arranged in the cardiology clinic and usually an MRI scan is performed around 3 months after the procedure to check for any weakness (aneurysm) of the vessel wall as a result of the procedure.
Most people do not need longer than a week off work. You should avoid any heavy lifting/strenuous exercise for 3-4 days until your leg is no longer sore.
You shouldn’t have any worrying side effects or symptoms but if you do you can telephone the specialist nurses for advice during the week (8am-4pm) or 111 out of hours. You will be given specific advice regarding what to look out for when you are discharged from hospital.
Follow up will include reviews with a cardiologist or specialist nurse and usually an MRI scan every 3-5 years.
Do I have a choice?
A small number of patients will decide they do not want any form of treatment at all having understood all the risks. If this is the case, we would still encourage you to come for regular reviews.
Other information
If you decide to proceed you will be placed on the waiting list.
You will receive a letter through the post with your procedure date and with your
pre-assessment date. We try to give you around 4 weeks’ notice but it’s often not possible for us to give you more than a week or two notice of the date of your procedure.
Contact the secretary
Please contact the secretary as soon as you receive your letter to confirm the appointment.
This is very important
If you do not confirm in good time your slot will be offered to someone else.
If you are taking anticoagulant (blood thinning) drugs such as warfarin or rivaroxaban you will need to stop this in advance. You will receive a telephone pre-assessment call approximately 2 weeks prior to the date of the procedure.
Please make sure you have had a recent dental check-up and all outstanding dental treatment has been completed before the procedure due to the small risk of endocarditis (infection in the heart). If you need invasive dental treatment within 6 months of your stent placement, you need antibiotic cover. Please ask your doctor or nurse for more information.
Important points to consider
- Exercise: Regular exercise, to a moderate level, is encouraged. It is good for overall health and can also help to keep blood pressure lower / under control. Activities such as walking, cycling, and swimming are ideal and it is important to warm up and warm down slowly. It is best to avoid really intense cardiovascular exercise, for example sudden ‘bursts’ of strenuous activity. Heavy weight lifting should be avoided, but it is usually okay to do low level weights at the gym (up to 15kg), ensuring that you are able to do 3 sets of 12-15 repetitions without any strain/breath-holding. Other activities that cause you to hold your breath or strain to lift/move objects, for example shovelling snow, trying to push a heavy object or playing some brass/woodwind instruments should be avoided as these can raise your blood pressure too much and this can cause further problems with your aorta.
- Do have your blood pressure checked in the RIGHT arm only. The blood pressure in your left arm is likely to be falsely low.
- Talk to us before you get pregnant. This is to enable the cardiologist to assess your heart in more detail prior to pregnancy and to arrange further tests if necessary. We will need to see you at least once during your pregnancy.
- The chances of having a baby born with congenital heart disease are slightly increased from the general population if you have congenital heart disease yourself. The risk is generally quoted as being about 2-4%, compared to 1% for the general population. Your cardiologist can discuss this with you in clinic prior to planning a family. We can offer a specialised scan of your unborn baby’s heart at 18-20 weeks, which can detect any major abnormality of the heart.
We appreciate it can be quite a wait between your clinic appointment and your procedure so, if in the time waiting for your procedure you have any questions or concerns, then please contact the specialist nursing team who will be happy to assist you.
Contact details
Dr Bentham / Dr Velasco / Dr Kang secretary
Specialist Congenital Intervention Nurses
Adult Congenital Heart Disease Specialist Nurses
Ward L14
Tel: 0113 392 7414