Aches and pains
After coronary intervention (also known as angioplasty) people are often more aware than normal of any little aches or pains that they might get. It is important to remember that flickering pains in your chest lasting a few seconds are quite common after coronary angioplasty and nothing to worry about.
If you get pain that lasts longer than a few minutes you will need to follow the 10 minute rule.
‘The 10-minute rule’
- Sit down, rest and try to relax
- If pain is present and you have been prescribed GTN (Glyceryl trinitrate), use
one spray or tablet under the tongue and wait five minutes - If pain is still present use another spray (or tablet) under your tongue and wait five minutes
If pain is still present dial 999 to call for emergency services.
Introduction
This page is written for people are having or have had a coronary angiogram and/or coronary intervention for coronary heart disease. It aims to give you, and the people who care for you, information about your treatment, hospital stay and recovery.
At different stages of your recovery, you and your family will want to know about different things. Some people find it difficult to remember information given to them while in hospital. Often people do not know what to ask during their hospital stay and find that when they get home they have questions, but nobody to ask.
To help with this, we have provided a list of contacts, self-help groups, advice lines and other sources of information at the end of the page. You will also find an explanation of some medical words that you may have heard used during your stay.
Please feel free to ask questions during your hospital stay or visit. We understand that we cannot cover all of the information that you might want on this page.
If you speak a language other than English and you need an interpreter, please mention this to the ward staff where you are being cared for, or if you are having a planned procedure ring the ward to let them know. If you could do this 3-4 days before you are admitted this will give us an opportunity to arrange an interpreter for you.
If you are having a planned procedure and have any questions about your treatment please contact:
Cardiology admission office: 0113 392 3960 (9.30am-3.30pm)
Ward L14: 0113 392 7414
Explain my procedure
Please access the appropriate website below to watch a video that will explain your procedure:
www.explainmyprocedure.com/angiography-leeds
www.explainmyprocedure.com/angiographyangioplasty-leeds
Back to topKey take home messages
- Angiography is a test which shows x-ray pictures of the heart arteries. This will show any narrowing’s in the coronary arteries that could be limiting blood flow to the heart muscle
- Coronary intervention (also known as angioplasty) is a treatment performed under local anaesthetic to widen narrowed coronary arteries. This usually involves the use of ‘stents’ which act like scaffolding to strengthen the artery
- Coronary intervention relieves angina symptoms for most people. It is also a very effective treatment for patients having a heart attack
- If you are having a planned procedure you will need to prepare for your admission. The pre-assessment nurses along with this page will guide you in how to prepare for your angiography and/or coronary intervention
- Most people having planned procedures are in hospital for six hours after angiography or coronary intervention
- If you have been admitted to hospital unwell, you may be required to stay for longer than if it were a planned procedure
- If you get pain or discomfort in your chest that lasts longer than a few minutes and does not go with rest, you will need to know how to manage it. Information on page three explains how
- When you go home, you and your family can get advice about living a heart healthy lifestyle from this page and the specialist cardiac rehabilitation nurses
- The British heart foundation has a help line that you can ring for advice about heart health – 0300 330 3311
Email: [email protected]
Website: www.Bhf.Org.Uk
You and your treatment
What are coronary arteries?
Your heart is a muscle that works as a pump to ‘push’ blood around your body. It can do this because its walls are made of powerful muscle. To stay healthy and work properly your heart muscle needs its own supply of food and oxygen.
The picture below shows the pipes or blood vessels that carry blood containing food and oxygen to your heart muscle. These pipes are called coronary arteries.
Model of the heart

Why have my coronary arteries become narrowed?
Coronary arteries supplying the heart can become diseased. This process is part of a condition known as coronary heart disease.
The exact cause of coronary heart disease is unknown but there are factors that increase your risk of it developing such as high blood pressure, diabetes, raised cholesterol and cigarette smoking. Coronary heart disease builds up over many years. Fatty deposits can collect inside the coronary artery making it narrow.
The good news is that you can reduce the risk of the narrowing getting any worse by living a healthy lifestyle. This is something that is in your control. Further advice on healthy living and how this can help your heart is provided later on this page.
Remember that you are not alone. Coronary heart disease is a common condition affecting more than two million people in the UK. In time, you can get back to living your normal day-to-day life.
How do I know I have narrowed coronary arteries?
People often get symptoms when their coronary arteries narrow. This is usually what makes people visit their doctor or the hospital for help and advice. No two people have exactly the same type of symptoms. People may feel discomfort, pain, an ache or a feeling of heaviness in their chest when they exercise e.g. walking up a slope. They may also feel slightly out of breath.
Typically these symptoms may occur with exercise during which the heart rate is increased, for example walking up an incline or carrying a heavy load. This is because during exertion the heart muscle needs more blood and oxygen to function. The narrowed arteries cannot supply blood fast enough. This reduced blood supply at a time when the heart muscle is demanding more can result in the symptoms mentioned above.
Sometimes the symptoms caused by narrowing of the heart arteries can come on at rest. It may prompt admission to hospital for more urgent investigation and treatment. If you experience any of the symptoms mentioned and you have a GTN spray or tablet to use you should follow the advice at the top of this page (the 10 minute rule).
What is angina?
Angina is the term used for chest discomfort caused by reduced blood flow to the heart muscle. Angina is a sign of coronary heart disease, it is not a mini heart attack. In other words, the discomfort of angina does not cause damage to the heart muscle. When you rest or take a nitrate medication (such as GTN spray) the chest discomfort or breathless feeling will go away.
In the meantime it is important to let your nurse know if you get any feelings like these during your hospital stay. You can be given medicine to relieve these feelings, should they occur.
What is a heart attack?
A heart attack, also known by the medical term ‘myocardial infarction’ or ‘MI’ for short, occurs when the blood supply to the heart muscle is blocked for a longer period of time. A heart attack develops when there is a rupture or erosion of a fatty deposit, causing a blood clot to form within the artery.
This usually happens without any warning. This results in damage to the heart muscle beyond the area of blockage. Symptoms of a heart attack are usually the same as angina but more severe, commonly last longer than 30 minutes and are not relieved by rest or medication, such as GTN spray. A heart attack may be the first sign of coronary heart disease for some people.
What is a coronary angiogram?
This is a test done under local anaesthetic using X-ray contrast (a clear iodine containing solution) to show up the coronary arteries and highlighting any narrowing.
The test usually takes 20 – 30 minutes. It involves inserting a small flexible tube (catheter) into the artery in your wrist following an injection of local anaesthetic to numb the skin. Occasionally, a tube may be inserted into the artery in the groin instead. Through X-ray guidance, this is passed up to your heart. X-ray pictures are taken as the X-ray contrast goes through your coronary arteries. You should not feel any pain as there are no nerve endings in the coronary arteries, but you may feel a few palpitations (missed beats). The X-ray contrast can occasionally cause you to feel quite hot and flushed but this should pass in a few seconds. The X-ray contrast passes out through the kidneys and in the urine. Sometimes people can experience blurred vision after the procedure until the X-ray contrast clears.
After the test, a doctor or nurse will remove the tube and pressure is applied until the bleeding has stopped, usually with a wrist band device.
What is coronary intervention and how does it work?
Coronary intervention (also known as angioplasty) is a treatment that widens a narrowing or blockage in your coronary artery (for some people this can be performed at the same time that you have your angiography procedure). This means that blood flow to your heart muscle is improved. This treatment restores blood flow and limits damage to the heart in people with heart attacks and helps to relieve symptoms of chest discomfort in people with angina.
Coronary intervention is not a cure for coronary heart disease. The two most powerful things you can do to improve your heart health are to live a healthy lifestyle and take your medicines as recommended.
To widen your coronary artery your cardiologist passes a small balloon into the narrowed or blocked artery under X-ray monitoring.
Once the blockage has been found, the balloon is inflated and in doing so widens the narrowed coronary artery. The picture below shows the difference between a coronary artery before and after treatment.

In most coronary intervention procedures a coronary stent is used to scaffold open the narrowed part of the coronary artery. This helps to stop the coronary artery renarrowing in future.
A coronary stent acts like a scaffold to hold the coronary artery open after it has been widened. The picture below shows a stent which looks like a short, tiny wire-mesh tube.
A coronary stent

Once the stent has been put into your coronary artery it cannot move. In time a new lining grows over it and it becomes part of the wall of your coronary artery.
Complex coronary intervention
Sometimes the nature of the narrowing or blockage means the procedure will be more complex. This could be due to a long-standing complete blockage of the artery or the presence of calcium in the artery.
In cases of long-standing complete heart artery blockages special techniques are used to allow your doctor to open the artery, and often requires two tubes to the heart to deliver the equipment needed. There is a small chance in these cases that despite best efforts the artery cannot be opened. If successful then stents are used to scaffold open the artery.
In cases where there is a lot of calcium the artery is hardened and ‘rock-like’. So, it is safer and better for the calcium to be cracked before the stent is used. Your doctor can use specialist equipment for this, which will be chosen based on the type of narrowing. This can include special balloons, some with the ability to cut into the calcium and some that can deliver sound waves to cause shock cracks in the calcium. Alternatively, a drill or laser can be used that breaks down and cracks the calcium. The drill is noisy and sounds similar to a dentist’s drill. On occasions with these techniques, you can be aware of chest discomfort similar to your angina. Finally, a stent is used to scaffold open the treated artery.
These procedures are technically more challenging and likely to take longer, however the risks are only a little higher than that of a conventional procedure. Your doctor will explain the specific risks of your procedure at the time of your consent. As with other coronary angioplasty/intervention you will be awake and the procedure is still done under local anaesthetic.
Back to topCoronary intervention benefits and risks
It is important that you understand the benefits of coronary intervention and the possible risks. Your doctor and nurse will discuss these with you as part of a process called ‘informed consent’. Before going ahead with the procedure, you will be asked to sign a consent form. The following section provides information on the expected benefits of coronary intervention and the possible risks. The information provided is based on average results from the United Kingdom database of coronary intervention procedures. The risks may be lower or higher in individual cases. You will be able to ask any questions to the doctors and nurses before going ahead.
What are the risks of coronary intervention?
Coronary intervention is an effective and well established treatment for coronary heart disease. Most people undergoing coronary intervention have a successful procedure without any problems. However, as with any medical treatment, it is important to recognise that problems can occasionally occur.
The following section explains the possible risks of coronary intervention. You need to be aware of these as part of the process of informed consent. If you have any questions, please discuss these with your doctor or nurse.
Serious problems
The most serious complications are: major heart attack, need for emergency heart surgery, need for further urgent coronary intervention, stroke or death.
The risk of serious problems depends on whether you are having coronary intervention for stable coronary disease (angina) or for an acute coronary syndrome (myocardial infarction or ‘heart attack’).
Risks
[Numbers from National Institute for Cardiovascular Outcomes Research (NICOR) audit 2017-18]
It is important to recognise that some of these problems may occur due to the acute coronary syndrome itself and not necessarily the coronary intervention procedure.
The following section provides more detailed information on the risks of coronary intervention, divided into problems that can occur at the time of the procedure and those that can occur later.
Complications which can occur at the time of the procedure or shortly afterwards
Complications which may occur later after the procedure
- Narrowing of the stent (restenosis) can sometimes occur, but the risk is low with modern stents (around 5 patients per hundred). If your stent narrows, you may experience symptoms of angina and another coronary intervention or coronary bypass graft surgery may be required.
- Blockage of the stent due to clot (stent thrombosis) is rare – affecting fewer than one patient per hundred in the first year. After one year, stent thrombosis affects between 2-4 patients per thousand per year. Stent thrombosis is serious and can cause a heart attack. To help prevent this risk, it is very important that you take your medication as advised – in particular aspirin and other anti-platelet medications. Stopping anti-platelet medications too early is one of the major causes of stent thrombosis. If you think you will find it difficult to remember to take your medication, please speak to your doctor, nurse or pharmacist before you go home.
Sometimes reading lists of possible problems that could occur after medical procedures can seem frightening. It is important to remember that the majority of patients do not experience any complications. Your doctor has recommended coronary intervention taking into account the risks and benefits to you. If you have any concerns or require further information please do not hesitate to ask any of the doctors or nurses before going ahead with the procedure.
Notes
Information on the risks of coronary intervention in the UK was accessed from the British Cardiovascular Intervention Society
(https://www.bcis.org.uk/resources/audit-results/)
Acute admission to hospital
You experience chest pain or other symptoms that prompt you to go to seek medical attention.
Your symptoms, ECG and blood tests suggest the problem is related to the heart.
You are admitted to a cardiology ward for further investigations, monitoring and treatment. Occasionally where there are no beds available on a cardiology ward, you may be admitted to a more general ward and our cardiology doctors will visit you there.
If the doctors feel that your symptoms are related to a narrowed heart artery or heart attack (myocardial infarction), you remain in hospital for further investigation and treatment.
You are prescribed medications to help protect your heart and reduce the risk of further problems. Blood tests are performed to check your cholesterol levels and determine whether or not you have diabetes. Often a cardiac ultrasound (echo) is carried out to assess the pumping action of the heart.
Among other tests and treatments that are recommended, you are likely to undergo coronary angiography and potentially coronary intervention. Depending on your condition coronary angiography and coronary intervention may all be carried out at the same time. This will be decided by the doctor whose care you are under on the ward.
If you are diagnosed with a heart attack or you undergo coronary intervention you may see a cardiac rehabilitation nurse in hospital. During this visit you will be offered further information about your condition, medication management and advice on recovery and lifestyle risk factor management. Referral to a specialist community based service will also be discussed. If you are diagnosed with unstable angina which is treated with medications, you can still see a cardiac rehabilitation nurse for support, you will need to ask the nurse caring for you on the ward to request this.
After you go home, it is important that you take your medications as recommended. The dose of some of the medications usually needs to be increased (or titrated) over the next 4-6 weeks to achieve maximum benefit. You will need to contact your GP practice to make sure this takes place.
What to expect when you have an unplanned admission to hospital
If you attended the hospital with pains in the chest or other symptoms that suggest a problem with the heart you are likely to have had a number of routine tests to help the doctors diagnose the problem.
Acute coronary syndrome
Acute coronary syndrome is the name given to a group of conditions linked to coronary heart disease, where fatty deposits or plaques develop inside the heart arteries. In most cases, the fatty deposit becomes disrupted by a small ‘rupture’ or ‘erosion’ developing on its surface. This causes a blood clot to form within the artery, which can reduce or stop the blood flow to an area of the heart muscle. Because this can happen without an obvious trigger, patients with acute coronary syndrome often experience symptoms without any warning. The symptoms are similar to those in angina, but usually occur without provocation and are often more intense and longer lasting. These symptoms can vary between individuals, but most commonly include heaviness in the chest which may spread to the shoulders, arms, or throat; breathlessness; sweating; nausea and vomiting.
Types of acute coronary syndrome
There are three main types of acute coronary syndrome which are diagnosed depending on your symptoms, your ecg and the results of troponin levels on your blood tests:
The presence of clot in the artery reduces the blood flow and causes some degree of heart muscle damage, which is detected as elevated levels of troponin on your blood tests. NSTEMI is treated in the first instance by intensive medication to reduce clotting in the coronary arteries and improve blood flow. A coronary angiogram is usually carried out over the next few days.
Unstable angina is a type of acute coronary syndrome in which one of your arteries is sufficiently narrowed to cause symptoms on minimal exertion or at rest. There may or may not be clot within the artery. There is no heart muscle damage, such that troponin levels on your blood test are not elevated. Unstable angina is not technically a heart attack, but because the underlying cause is the same it is often dealt with in the same way as the other acute coronary syndromes.
All patients with suspected acute coronary syndrome are admitted to hospital for investigation and treatment.
While you are in hospital it is very important that you tell the nursing staff if you develop further discomfort in the chest or symptoms similar to that which brought you in to hospital. You may have a GTN spray already but it is best to tell someone before you use it, this way the nurses can ensure your safety and carry out tests such as an ECG to get more information at the time of your symptoms.
If you are suspected to have had an acute coronary syndrome (ACS) you are likely to be offered an angiogram with the option of coronary intervention if needed as part of your investigations. You need to stay in hospital whilst this is arranged. We hope to carry out procedures such as this within 2-3 days however occasionally that wait can be slightly longer. This is because our cardiac catheter labs care for urgent patients from across the region and also have to accommodate emergency admissions. This can sometimes delay the procedures for more stable patients. We try to inform you of the timing of your angiogram as soon as possible. However, please bear in mind that plans can sometimes change at the last minute if emergency procedures need to be carried out. We know that this can be very frustrating when you are waiting on the ward, but if this happens your understanding is much appreciated.
While you are waiting for your procedure in hospital, treatment for the heart has already started in the form of cardiac medications. These medications help stabilise the heart and heart arteries based on your initial diagnosis and form the mainstay of treatment for acute coronary syndromes. These medications will continue if you are found to have a narrowed or blocked heart artery.
Other tests which we may carry out while you are waiting for your procedure include:
The first part of this page gives information on Coronary Heart Disease and tells you what to expect from angiogram procedures and coronary intervention. Recovery in hospital after these procedures depends on the findings of your angiogram. Often following straightforward Coronary
Intervention patients are discharged home the same day. Sometimes further tests or treatments are required. Your doctor and the nursing staff on the ward will discuss this with you.
While you are in hospital it is a good time to consider any lifestyle risk factors that may have contributed to the development of narrowing in the coronary arteries and how these can be managed. While you are in hospital you can also talk to a cardiac rehabilitation nurse for further advice and support. Ask the ward nurse caring for you if you would like to see a member of the cardiac rehabilitation team. If you are diagnosed with a Heart Attack you will automatically receive a visit from a cardiac rehabilitation nurse.
Back to topPlanned procedures
Information for day case patients undergoing planned procedures
Clinic visit before your planned procedure
The pre-assessment clinic is run by nurses with the aim of preparing you for your planned coronary angiography and/or coronary intervention. Not all patients coming in for a planned angiogram will be preassessed. If you need a preassessment appointment you will be informed of that in your admission letter.
During your visit a blood sample will be taken for routine tests, as well as a tracing of your heart and measurement of height and weight. Please bring a copy of an up to date repeat prescription slip with you. That way we can see which medications you take.
At the clinic you may be started on an anti-platelet medication such as Clopidogrel if this is not already in place. This reduces the risk of blood clots forming in the heart arteries during and after your procedure. The preassessment nurse will guide you in terms of which medications to stop and which to continue. Please inform the pre-assessment nurse if you take an anti-coagulant (blood thinning medication) or metformin for diabetes.
It is important that you tell the pre-assessment nurse if you have ever experienced an allergy or adverse reaction to the x-ray contrast or to latex.
A pre-assessment nurse will also ask you some questions about your health and talk to you about your procedure. You may like to bring a family member or friend with you. You will be given the opportunity to ask questions. So it may also be useful to jot down any questions that you have before you come to clinic. There are notes pages at the back of this book which can be used.
We would appreciate it if you could telephone us if you cannot attend your appointment.
The telephone number is: 0113 392 5639 or 0113 392 8110
This may help us to allocate the clinic place to another person.
Use the checklist below to prepare for your planned admission
- You should avoid caffeinated drinks (tea, coffee, fizzy soft drinks and chocolate) for 24 hours before your procedure. Caffeine can interfere with some of the tests we may need to carry out during the procedure.
- You can have a light breakfast on the day of your procedure
- Take your usual medications on the morning of the procedure unless advised otherwise at your pre-assessment appointment. Please bring your regular medications in to hospital with you.
- For most day case procedures you will be able to wear your own clothes during the procedure. Please wear something old and comfortable in case of marking (see the notes below for further information). A T-shirt and loose fitting trousers are ideal.
- Bring a dressing gown and slippers with you in case you are required to wear a hospital gown or stay longer for monitoring after the procedure. You may wish to bring an overnight bag with some toiletries just in case a longer stay is advised.
- Please remember to take any tablets the evening before the procedure if you have been advised to take a loading dose.
Notes: If you have been advised that your procedure will be performed via the groin, we ask you to shave a small area in your groin the night before you come into hospital, using an electric or disposable razor.
The groin area
The picture shows you two blue square areas which indicate where you need to shave in your groin area. Shave here! Each square about 7cms by 7cms

Patients should avoid wearing:
- Tight fitting pants/jeans
- Remove bra prior to procedure, Bras with no metal including clasps can be kept on
- No buttons on shirts/blouses.
- Sleeves below the elbow
- More than two layers of clothing if possible
- Jewellery (especially necklaces)
- Clothing with zippers or any other metal above the waist
- Any clothing which you would not want to get damaged
On the day of your procedure
After your procedure
After your coronary angiography/coronary intervention you will be taken back to your chair within the Take Heart Suite or bed on ward L14. The duration of bedrest and monitoring depends on whether you had coronary intervention or if you had angiography only. It also depends if the procedure was performed by the wrist or groin. Generally the recovery period is between two and four hours.
Your nurse will look at your wrist or groin for any signs of bleeding or swelling. Your blood pressure and pulse will also be monitored. This is routine for anybody treated with coronary intervention.
If you experience any pain, aches or discomfort in your chest, leg or arm it is important to let your doctor or nurse know immediately. Pain relief can then be given. It is common for people to be aware of a bruised feeling in the chest for a few hours or days after coronary intervention.
Back to topGoing home and your recovery
Your hospital stay is short and before you know it you will be back at home.
Many people want to know about what they can or cannot do during early recovery. During the first week:
Feeling emotional
- Being told that you have coronary heart disease can come as a shock to people and their families.
- The important thing to remember is that this condition is very common and you can go on to live a full and active life. By making healthy lifestyle changes and taking your medicines you can take control of things and reduce your risk of heart problems in the future.
- In the first few days you may feel quite different from day to day. Up one day and down the next. There is no right or wrong way to feel. It is totally
- individual. It may take time for you and your family to come to terms with what has happened.
Aches and pains
After coronary intervention (also known as angioplasty) people are often more aware than normal of any little aches or pains that they might get. It is important to remember that flickering pains in your chest lasting a few seconds are quite common after coronary angioplasty and nothing to worry about.
If you get pain that lasts longer than a few minutes you will need to follow the 10
minute rule.
‘The 10-minute rule’
- Sit down, rest and try to relax
- If pain is present and you have been prescribed GTN (Glyceryl trinitrate), use
one spray or tablet under the tongue and wait five minutes - If pain is still present use another spray (or tablet) under your tongue and wait five minutes
If pain is still present dial 999 to call for emergency services.
We have included this information because many people worry about what to do if they get chest discomfort or chest pains. This information provides you with a plan of action. We have not included this because we think you will have a heart attack.
It is important to remember that if your pain is caused by angina it will go away with rest and/or your nitrate spray or tablets. It is not a mini heart attack.
People who have a heart attack have pain that stays whatever is done. There are treatments that can be given to people who have a heart attack. These are more effective if people who have chest pain or discomfort for longer than 10 minutes call an ambulance immediately.
Don’t delay! If you have pain that lasts more than 10 minutes it is important that you do not drive yourself to hospital or get a family member to drive you. The earlier you get treatment the better. Ambulance staff will be able to start your treatment there and then if needed.
Making lifestyle changes
Risk factors for heart disease
There are a number of factors that can contribute to the development of Coronary Heart Disease (CHD) and therefore increase your risk of having a heart attack or developing angina. These factors are known as risk factors for CHD. They can be divided into being ‘modifiable’ or ‘non-modifiable’.
- Modifiable risk factors: factors that may increase your risk of CHD which can be changed to reduce the risk of future problems. These will be discussed in detail over the following pages.
- Non-Modifiable risk factors: factors that may increase your risk of developing CHD which cannot be changed.
Fortunately, you can control many of the modifiable risk factors that contribute to the narrowing of the coronary arteries. Your cardiac rehabilitation nurse can help you set realistic, achievable goals to reduce the risk factors that apply to you.
Smoking
Stopping smoking is the single most important thing you can do to improve your health.
From the minute you stop smoking there are health benefits.
Nicotine replacement therapy (NRT)
Nicotine Replacement Therapy (NRT) replaces a small amount of the nicotine that you used to get from cigarettes. It is the addictive nature of nicotine that makes it hard for many people to quit. NRT provides you with some help with the addiction and allows you to deal with the habit side of smoking first. Remember you are four times more likely to quit for good using a combination of medication and specialist support.
Your cardiac rehab nurse or Stop Smoking advisor can advise you on which types of NRT would be most suitable for you and which products can be combined to achieve the best outcomes.
The use of medications to stop smoking
There are two medications that can also be considered to help you stop smoking; these should only be considered under advice from a specialist who can prescribe, such as the Stop Smoking advisor or your GP. Using medications such as those listed below can double your chances of stopping smoking. However, they can have side effects and may not be recommended in certain health conditions.
The use of e-cigarettes to stop smoking
- Electronic Cigarettes or Vaporisers do not contain tobacco; they create vapour from liquid nicotine. E-cigarettes are not licenced for use as Nicotine Replacement Therapy (NRT) at present.
- Public Health England state that e-cigarettes are at least 95% less harmful than smoking.
- E-cigarettes are the most popular quit smoking aid and when combined with specialist stop smoking support can be the most effective way to quit smoking for good.
High blood pressure
Blood pressure is the force that circulating blood puts on the artery walls. When blood pressure is high, there is more pressure on the artery wall than usual. Some people have high blood pressure and do not know they have it. This extra pressure damages the smooth lining of the arteries and makes it easier for cholesterol and fat to build up along the artery walls. As the arteries become clogged with these fatty layers (atherosclerosis), less blood gets through. This causes the heart to beat harder as it tries to pump blood through narrowed arteries. If untreated, high blood pressure may in time damage the heart, brain and kidneys. It is a leading cause of heart attacks and strokes, heart or kidney failure.
The exact cause of high blood pressure is not fully known for many people. High blood pressure can be lowered with medication.
Cholesterol
Cholesterol and triglycerides are fatty chemicals in the blood. There are two main types of cholesterol; LDL ‘bad cholesterol’ which carries cholesterol from the liver to the rest of the body, and HDL ‘good cholesterol’ which returns excess cholesterol to the liver.
While foods with plant stanols and sterols are thought to reduce the absorption of cholesterol from the gut (British nutritional foundation), they do not provide sufficient reduction in cholesterol and should not replace the medicines prescribed to lower cholesterol. They can be taken alongside the cholesterol-lowering medicines that you were prescribed. Plant stanols and sterols are usually added to particular spreads and yoghurts and they are also found naturally in nuts and seeds and some fruits and veg.
If you have high levels of cholesterol and triglycerides, your risk of CHD is greater.
High levels of LDL cholesterol stick to the walls of your arteries and make plaque. This plaque blocks the arteries, interfering with the blood flow which can make a heart attack more likely.
The treatment for high cholesterol is now as routine as that of other common conditions. Treating raised blood cholesterol is a positive way you can do something to avoid future heart problems. The next section provides information about diet which can help you to control your blood cholesterol levels.
The aim of your cholesterol lowering medications is to reduce the bad cholesterol (LDL) to less than 1.8 mmol/L. If LDL is not measured then we aim for more than 40% reduction in non-HDL cholesterol (which is your total cholesterol excluding good cholesterol).
It is recommended that once starting cholesterol-lowering medications, you have your cholesterol checked after three months and then at least yearly, unless advised otherwise. This can be carried out by your local GP practice.
Cholesterol

Diet: getting the balance right
Overall dietary balance is important. No single food contains all the essential nutrients the body needs to be healthy and function efficiently. A balanced diet should include a variety of foods.
The following illustration represents each of the five food groups and gives a guide to the proportions of food we need to achieve a balanced diet.
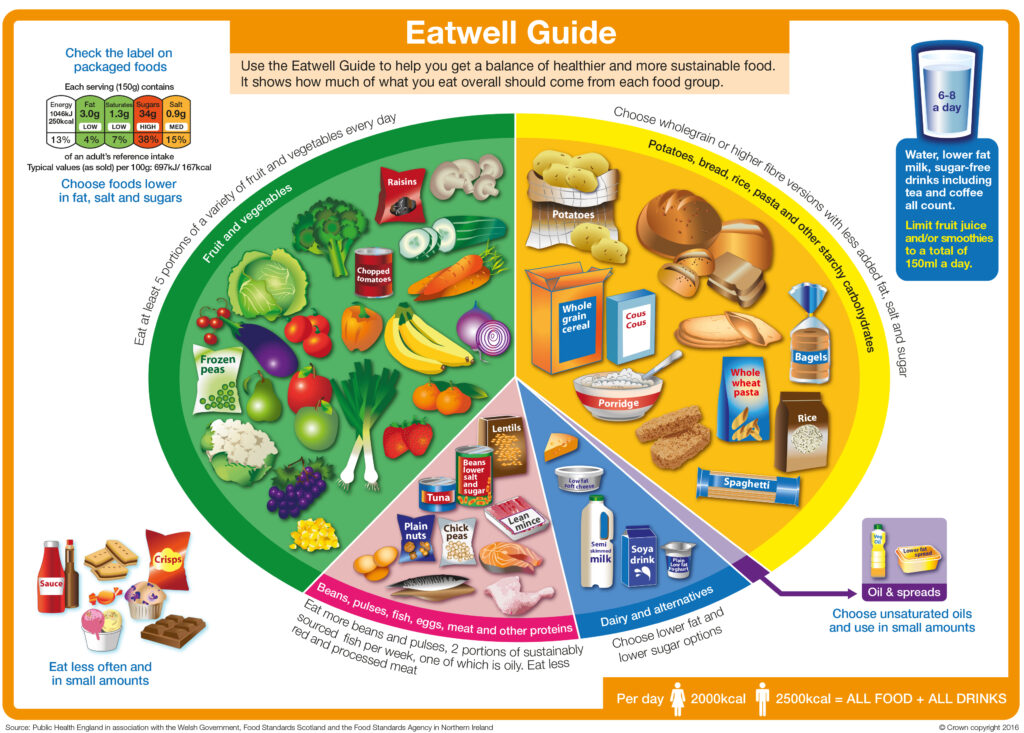
Adapted from The Eatwell Guide as per crown copyright protection.
Five easy ways to five a day
Check this website for further examples (https://www.bhf.org.uk/informationsupport/support/healthy-living/healthy-eating/recipe-finder)
Cardioprotective diets
Cardioprotective diets generally follow the Eatwell Guide principles and are linked with a healthier heart. One example would be a Mediterranean style of eating. This is one well known whole dietary approach that may suit you.
Be mindful that other dietary approaches may work better for you, but the most important thing is to think of your diet as a whole. Continue with any cardiac beneficial, whole dietary approaches that suit you.
Fat
A cardio protective style of eating is not necessarily low in fat, but the type of fat is important. There are two groups of fats: saturated and unsaturated. Healthy fats are better than very low fat. The cardio protective diet is more beneficial than a very low fat diet in prevention of CVD. If you need to reduce your weight, then you need to eat less fat of any kind and this should be a small proportion of your overall diet. Replacing saturated with unsaturated fat is better than replacing it with carbohydrates or protein.
| Unsaturated Fat Unsaturated fats in small amounts are thought to be better for us as they help to lower your LDL (bad chol; total cholesterol and helps to lower your LDL (‘bad’ cholesterol). There are two types: Monounsaturated and Polyunsaturated. | Examples of foods Monounsaturated Fat: Avocados, olives, olive oil, rapeseed oil. Almonds, cashews, hazelnuts, peanuts, pistachios, spreads made from these nuts. Polyunsaturated Fat: Oily fish, corn oil, sesame oil, soya oil, and spreads made from those oils. Flaxseed, pine nuts, sesame seeds, sunflower seeds, and walnuts. |
| Saturated Fat Saturated fats usually come from animal products These fats tend to be solid at room temperature. Although we need a small amount of these fats in our diet, larger amounts can be harmful because they can raise your LDL or ‘bad’ cholesterol, so try to reduce the amount you eat. They need to be a very small percentages (less than 10%) of your diet. Try to reduce the amount you eat or substitute with polyunsaturated fats. | Examples of foods Processed meats like sausages, ham, burgers. Fatty meat. Hard cheeses including cheddar. Whole milk and cream, butter, lard, dripping, ghee, suet, palm oil and coconut oil, pies, cakes, biscuits, pastries, fried foods. |
| Trans Fat Trans fats are thought to behave in a similar way to saturated fats and are therefore harmful when taken in excess quantities. Try to avoid these when possible. | Examples of foods May be in some fried foods, takeaways, processed snacks like biscuits, cakes or pastries. Hard margarines |
Salt
Most of us consume more salt than we need. High salt intakes can contribute to high blood pressure and fluid retention. Gradually reduce the amount of salt you add to foods – in cooking and at the table to allow you to adapt to the change in taste. Use other means of seasoning such as pepper, herbs, spices and lemon juice to flavour foods. Pre-prepared foods, sauces and soups can contain lots of salt – check the labels and try lower salt varieties, or prepare foods yourself without adding salt if possible.
Foods high in sugars
These foods should be eaten in small quantities. They provide excess calories and can contribute to weight gain. It is important to limit the amount of ‘free sugars’ in the diet. Too much free sugar can raise your triglycerides (fatty chemicals in the blood). Free sugar includes sugar added to food and drinks (either at home or during manufacturing) and sugar naturally found in foods like honey, agave syrup or fruit juice. Adults can have up to 30g of ‘free sugars’ a day. The sugar found naturally in whole fruits and vegetable is not free sugar and does not need to be included in this amount. There is advice on how to cut down on sugar on the NHS live well website. This group includes biscuits, cakes, ice cream, sweets, chocolate and fizzy or sweetened drinks.
How do I understand food labels?
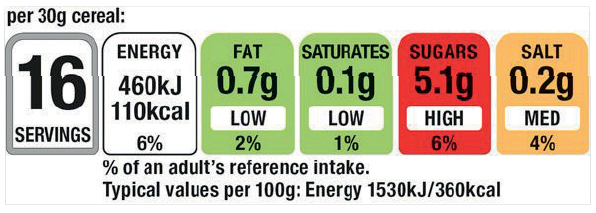
Nutrition labels can help you choose between products and keep a check on the amount of foods you are eating that are high in fat, saturated fat, sugar and salt.
Packaging often shows foods in ‘traffic light’ colours, so that you can see at a glance if they are high (red), medium (amber) or low (green) in fats, sugar or salt. For a healthier choice, try to choose products that have more greens and ambers than reds.
If you have a smart phone you can download the food4life food scanner App. You can scan product bar codes to check levels of sugar, saturated fat, salt and calorie content of the item. This will allow you to make an informed choice about your purchase (or product at home).
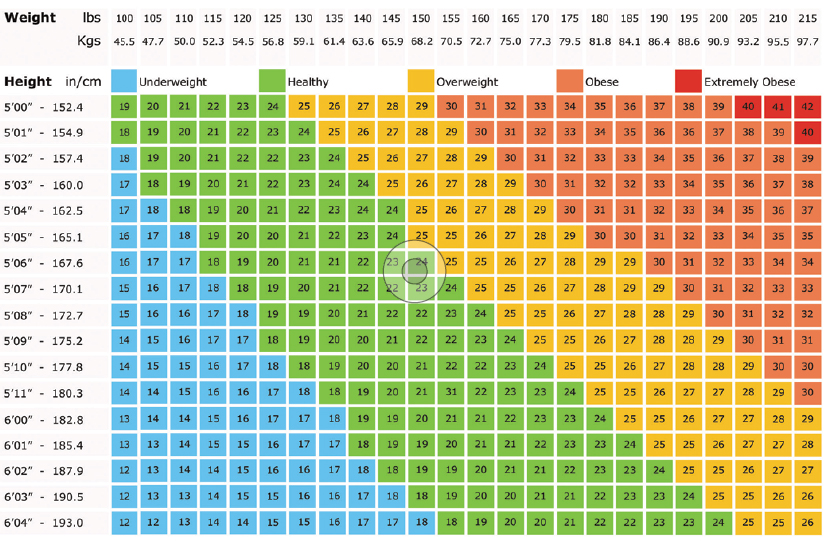
Back to topBeing overweight
If you are overweight, then aiming to reduce your weight by 10% is beneficial. For example, if you are 18 stone, aim for 16 stone or if you are 14 stone aim for 13 stone. This will reduce the strain on your heart and will help lower your blood pressure. If you follow the dietary advice to reduce fat intake, your weight should come down. Waist size is an indicator for heart disease risk. 37 inches for a man and 31.5 inches for a woman is the top end of waist measurement that is considered healthy (BNF).
You can reduce your energy intake by changing the snacks you eat, (e.g crisps, cakes, biscuits) to the fruits and vegetables suggested. Do not forget that all alcoholic drinks contain calories.
Be careful when choosing low fat foods as some can still be high in calories due to the amount of sugar in the foods e.g fruit juices, reduced calorie biscuits and low fat yoghurts.
You may notice that you tend to eat more when you are feeling worried, low in mood or bored. If this happens to you, try and find an activity or hobby that will take your mind off food or have a glass of water or no added sugar squash instead.
Keeping a diary of what you eat and drink can also help you to find ways in which you can reduce the amount of energy you eat. The support of your friends and family is also important to help you to keep motivated.
See the following website for further details: https://www.nhs.uk/better-health/lose-weight/
There are also tools and information on the British Heart Foundation website that can help you to build healthier eating habits into everyday life (for example Heart Matter Healthy Recipe Finder).
BMI Chart
Diabetes
What is diabetes?
Diabetes is a condition which occurs when either the body does not produce enough insulin or the insulin that is produced by the pancreas does not work properly. This means that the glucose (sugar) cannot enter the cells in the body where it would normally be converted into energy. It therefore stays in the blood stream, causing the level of glucose to be too high.
Diabetes can occur at any age. The most common is called Type 2 which mainly affects those people over 40 years of age. Type 2 diabetes is strongly linked with being inactive, over-weight and often has a link with family history. It can also happen more commonly in certain populations, for example those with South Asian and African-Caribbean origins.
The risk of developing Type 2 diabetes can be reduced by taking regular exercise and maintaining a healthy weight.
Type 1 diabetes occurs when the pancreas is unable to produce any insulin and is usually diagnosed in young people or children. We do not know at present what causes this.
What effect does diabetes have on the heart?
People with Type 2 diabetes often have high triglyceride levels and low levels of HDL cholesterol (the protective type of cholesterol).
High glucose levels can affect the nerves to the heart, so dangerous symptoms are not felt in the usual way (for example, people with diabetes may not feel any pain with a heart attack which can lead to difficulty and delay in the diagnosis of heart problems).
What can I do about diabetes?
Diabetes cannot be cured, but it can be managed and controlled. The two main aims of diabetes management are to resolve the symptoms of diabetes and prevent the health problems associated with this condition. Glucose levels can be improved by following a healthy diet, being physically active and taking the medications prescribed. Keeping to a recommended weight is also beneficial.
What are the health risks associated with having diabetes and what can be done to keep healthy?
People with diabetes have a higher chance of developing high blood pressure, circulation problems, nerve damage, damage to the kidneys and the eyes. The risks are particularly high in someone who is also overweight, who smokes and is not physically active.
It is important to attend regular check-ups, where blood glucose, blood pressure, kidney function, eyes and feet are monitored and overall diabetes control can be assessed. Further information about diabetes is available on request.
Back to topAlcohol
Drinking more than the recommended amount of alcohol can have a harmful effect on your heart and general health. It can cause abnormal heart rhythms, high blood pressure, damage to your heart muscle and other diseases such as stroke, liver problems and some cancers.
Alcohol is also high in calories so it can lead to weight gain. (See drinkaware.co.uk to check calorific value of alcoholic drinks.) It also lowers your inhibitions which might mean you find it harder to stick to your healthy eating plans when you have been drinking. If you are trying to lose weight, cut down on alcohol.
Most people don’t drink alcohol every day – but if you do, try having some days off – aim for at least two alcohol free days a week. Just make sure you don’t increase the amount you drink on the other days.
Drinking large amounts of alcohol in one go can cause damage to your heart muscle so avoid drinking 6 or more units in a day on a regular basis.
Your GP can help to support you in reducing your alcohol consumption if you decide you would like to do this. If you are a dependent drinker, please seek medical advice before you stop drinking suddenly.
You can find more information at www.drinkaware.co.uk
Alcohol units

Ensure you check the strength of what you are drinking, as this will affect the units, particularly if you are drinking stronger ales or lagers.
Consider the measures you pour when you are drinking at home, as these tend to be more generous than standard pub measures.
If you require further information or support with reducing your alcohol intake, please seek advice from your cardiac nurse or GP.
Back to topExercise and physical activity
Back to topCardiac rehabilitation
We mentioned earlier that there is professional help available to help you take control of your life again. The name given to the structured program of education and support is Cardiac Rehabilitation. If you have had coronary intervention you may be contacted by the community cardiac rehabilitation team in your area.
There may be a local cardiac exercise group near to you that you can join. Doing this may help you to continue to take regular exercise.
You can get details if you contact the British Heart Foundation Helpline on 0300 330 3311 or via their website at www.bhf.org.uk or see the list near the back of the book for the contact in your area.
Back to topMedication after your procedure
After planned angioplasty you will need to take several medicines. Some of these will be taken for a period of months, others will be for life.
Antiplatelets
Examples: Aspirin, Clopidogrel, Prasugrel, Ticagrelor.
After your stent is in place you will need to take medicines to reduce the risk of a blood clot forming in the heart arteries. These drugs are called antiplatelet drugs.
After a few weeks the lining of your artery will grow over the stent and it will become part of your artery. Until then anti-platelet drugs help to reduce the risk of clots forming on the stent. (If you normally take Warfarin or a DOAC (Rivaroxaban, Apixaban , Edoxiban or Dabigatran) this will be discussed with you on discharge.)
Are there any side-effects?
Medicines that thin the blood can mean that you bruise more easily. Aspirin and Clopidogrel should be taken with food as they can cause indigestion. Tell your doctor if you get indigestion.
Proton Pump Inhibitors
Lansoprazole, Omeprazole, Esomeprazole, Rabeprazole, Pantoprazole
How Do Proton Pump Inhibitors Work?
Your body produces a natural mucous barrier to protect the lining of your stomach from ‘stomach acid’. Antiplatelet medications can alter this natural barrier and make the lining of your stomach and gut more susceptible to damage. Proton pump inhibitors reduce the amount of acid produced in the stomach, which protects the lining of your stomach and gut from irritation and ulceration.
If you are taking ‘dual antiplatelets’ (aspirin plus a second antiplatelet) or a single antiplatelet with an anticoagulant, you may be prescribed a proton pump inhibitor. It is important to keep taking a proton pump inhibitor to protect your stomach for the duration of your dual antiplatelet treatment.
You may be able to stop taking your proton pump inhibitor after 12 months and this should be discussed with your GP.
Proton pump inhibitors should be taken at least 30 minutes before food and other medicines.
Unwanted effects
The most common side effects are on the gastro-intestinal system and include constipation, diarrhoea, bloating, flatulence, feeling sick and tummy pain.
For full information about the side effects of proton pump inhibitors read the information leaflet you get with your tablets. If you have any questions ask your doctor, nurse or pharmacist.
Beta-blockers
Beta-blockers slow your heart rate which reduces the work load of the heart and improves cardiac function. They are particularly important if your heart has been damaged by a heart attack or if you have heart failure. Some people experience side effects with these medications such as cold hands and feet, nausea, diarrhoea, skin rashes, erectile dysfunction and nightmares.
If you are affected in this way, please talk to your doctor but do not stop taking the beta blocker unless you are advised to do so.
Statins
Statins reduce the production of cholesterol. They reduce levels of bad cholesterol and increase levels of good cholesterol. Statins also make any fatty deposits in your coronary arteries more stable. This means that they are less likely to cause a blockage in your coronary artery.
Statins can sometimes affect your digestive system. Inform your doctor if this does not get better after a few weeks. A rare side effect of statins is pain or weakness of your muscles. If you experience this please visit your GP. Some statins react with food containing grapefruit.
ACE inhibitors
ACE stands for angiotensin converting enzyme. Angiotensin is a chemical in the body that makes blood vessels narrower and can damage the heart. ACE inhibitors act by lowering blood pressure and protecting the heart.
People usually start on a small dose of this medicine to see how it affects them. The dose will need to be increased by your GP. If you have had a heart attack, it is important that the dose is increased to the target dose over 4-6 weeks. Your GP will monitor this. Sometimes people get a dry irritating cough with this medicine.
Back to topCommon medical terms explained
Back to topFurther contacts
Health advice
Advice
Alcohol/drug misuse
Anxiety & Depression
Bereavement
Carers
Disability
Driving
Exercise
Information
Medication
Older people
PALS
Voluntary services/networks in Leeds
If you’re looking for support/assistance on discharge there is a vast amount available. You can get assistance with practical tasks such as shopping and gardening, assistance with checking benefits and completing the forms, social groups and drop-in centres to name a few.
These services are available through three main networks that can be accessed by telephone or on-line. They are:-
Back to topCommunity Cardiac Rehabilitation Teams Contact Numbers
Airedale Cardiac Rehabilitation Team
Tel: 01535 294 557
Bradford Community Based Cardiac Rehabilitation Nurse:
Bradford City – Tel: 01274 383 718
Bradford South & West – Tel: 01274 322 131
Calderdale Cardiac Rehabilitation Team
Tel: 07909 290265
Huddersfield Cardiac Rehabilitation (Local)
Areas included: Cleckheaton, Batley, Liversidge, Mirfield, Heckmondwike, Huddersfield
Tel: 0300 304 5555
Harrogate Cardiac Rehabilitation Team
Tel: 01423 553 355
Mid Yorks Cardiac Rehab Service
Normanton Office: 01924 543 460
Dewsbury Office: 01924 816 129
Leeds Community Cardiac Team
Tel: 0113 843 4200
Pontefract / Wakefield Cardiac Rehabilitation Team
Tel: 01924 327 923
York Cardiac Rehabilitation Team
Tel: 01904 724 697
