The information in this leaflet is about dealing with melanoma, and is intended for patients who have recently been diagnosed with melanoma, and their families.
The Leeds Melanoma Service
Melanoma team
The Melanoma Clinic in Leeds is based at the Cancer Centre at St James’s University Hospital. Patients are seen on Thursdays in the Bexley Wing Outpatient Department. The people that make up the team have different roles to play in your care, and it may be that you meet and have links with some of the team more than others, depending on your needs at any particular time. All members of the clinic team are available to discuss any questions or concerns you may have.
For your information we have set out a brief introduction to the team.
There is a glossary explaining some of the medical words used in the melanoma leaflets on page 14 of the leaflet, ‘Looking after yourself after a diagnosis of Melanoma has been made.’ If you hear any words or phrases that you do not understand, please ask your doctor or a member of your healthcare team what it means. It does not matter how many times you ask.
Consultant Dermatologists – Dr Angana Mitra,
Dr Andy Muinonen-Martin and Dr Hayley Smith.
The team has many years of experience in caring for patients with melanoma. In the Thursday clinic the team sees newly diagnosed patients from Leeds and the surrounding area. They provide follow up and surveillance for melanoma patients after diagnosis, and will discuss with them if further treatment is necessary at any point in the future. Dr Mitra and Dr Muinonen-Martin and Dr Smith also have a pigmented lesion clinic on a Wednesday. During these clinics you may be reviewed directly by a Consultant or by one of our training doctors or specialist nurses, under the supervision of the Consultant. This will be explained to you at the time.
The team also runs a large and established research programme exploring the causes and treatments of melanoma. You may meet some of the research nurses at some point during your visits.
Consultant Plastic Surgeons – Mr Howard Peach,
Mr James Smith and Miss Jenny Goodenough.
They are experts in the surgical treatment of melanoma. They see patients referred either directly to them from GPs or by referral from colleagues in the Yorkshire region. They also run a clinic on a Thursday in the Bexley Wing. The plastic surgeons carry out necessary surgery for melanoma patients. Mr Peach and Mr James Smith operate at the Leeds General Infirmary. Secretary’s telephone: 0113 392 2942
Consultant Oncologists Dr Maria Marples,
Dr Jane Hook and Dr Elaine Dunwoodie.
Our medical oncologists have a special interest in the treatment of melanoma. We also have a clinical oncologist, Dr Satiavani Ramasamy. They see patients with more advanced melanoma (which has spread to other parts of the body) or melanoma that has a higher chance of coming back.
The team has extensive experience of conducting clinical trials to help find new treatments for melanoma.
Research Nurses
During your treatment or follow-up it may be appropriate to discuss a clinical trial with you (see page 24). The team are available in clinic each Thursday to support you in considering participation in a clinical trial if appropriate and to co-ordinate and manage your care should you choose to take part.
Melanoma Clinical Nurse Specialist Team – your key workers
The nurse specialists’ role is to act as a key point of contact for melanoma patients and their carers, through diagnosis, treatment and follow up. They are available to provide emotional and psychological support, advice and education. Individual appointments outside of the clinic environment can be made, which allows an opportunity to discuss and clarify any information given, or to talk over treatment concerns/options.
Contact:
Tel: 0113 206 7660 Monday – Friday, 8am – 4pm. The nurse specialist team do not work on bank holidays.
Multidisciplinary Team Co-ordinator – providing administrative support for the interactions within the team.
Back to topWhat is Melanoma?
Melanoma is a form of cancer which usually develops in the skin.
It starts from a building block of the skin, a cell known as the melanocyte, which produces the brown pigment in the skin’s colour.
Often the melanoma has been a mole first, sometimes it grows from a single melanocyte, in what looks like normal skin. This melanoma on the skin is known as the primary melanoma.
One of the most important causes of melanoma is exposure to too much ultraviolet light in sunlight. The use of artificial source of UV light, such as sunbeds, also increases the risk of getting a melanoma.
Back to topDiagnosis
The diagnosis of melanoma is made by a specialist (usually a dermatologist or plastic surgeon), by looking at the skin. The diagnosis is confirmed, after removal, by the pathologist. The melanoma is usually removed, using local anaesthetic, both to treat the problem and to obtain the tissue which can then be examined by the pathologist.
Usually this operation is a minor one, which removes the melanoma with a thin rim of normal skin. The scar will vary in size with the melanoma but is usually an inch or so in length like the one seen here in the photograph.

What does the pathologist do?
When the piece of skin is removed it is sent to a pathology lab where it is processed. This processing takes time. It involves placing the skin in melted wax to form a so-called block. When the wax cools it hardens and the block is therefore firm enough to be handled. The block is placed in a machine, which allows a skilled technician to slice the tissue thinly and place the tissue (called a section shown below) on glass slides.

Stain is then added to the slides so that the nature (type) of the tissue becomes clear to the pathologist. The pathologist is a doctor who then looks at the slide, and interprets the pattern he or she sees and makes the diagnosis.
All of this usually takes a few weeks. Sometimes the pathologist needs more information and may request more sections to be cut or new stains be added.
Sometimes they might send the slides to another pathologist to seek a second opinion when the process may even take several weeks. The sample may also be sent for specialist molecular testing to help make the final diagnosis. This can be frustrating for the patient, but it is always better to take time and get the answer right.
Sometimes, the pathologist, even after discussion with other pathologists, cannot make a definite (clear-cut) diagnosis.
In such cases doctors tend to treat cautiously: that is, to treat the patient as if they have a melanoma, while being optimistic about the future. This is what happens when a lesion, called a spitzoid lesion of unknown malignant potential (STUMP for short or a Melanocytoma), is diagnosed.
Back to topWhat happens when the diagnosis is made?
Once your doctor has received the written report he or she will normally review the slides and the report, with the rest of the melanoma team, at a Thursday morning meeting called the multidisciplinary team meeting (MDT), and he/she will then discuss the results with you. The main issues are:
- Is it a melanoma?
- If it is a melanoma, what type is it?
There are three main types:
- Melanoma In Situ
- Radial Growth Phase Melanoma
- Vertical Growth Phase Melanoma
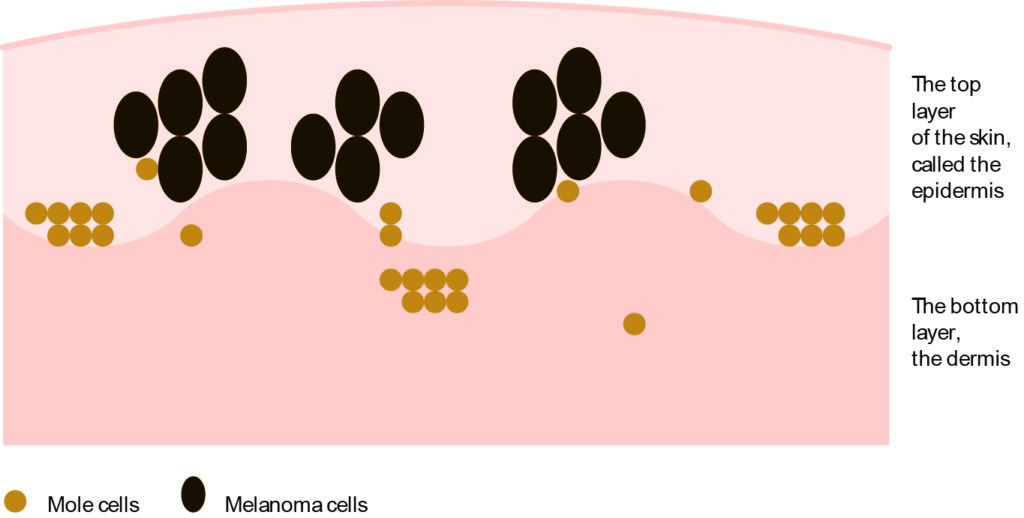
Melanoma in situ
This is a melanoma that is at a very early stage of development. The cancer cells are entirely in the top layer of the skin (the epidermis).
This type of melanoma is entirely curable and should never come back. The diagram shows the appearance of an in situ melanoma; the cancer cells are shown in black.
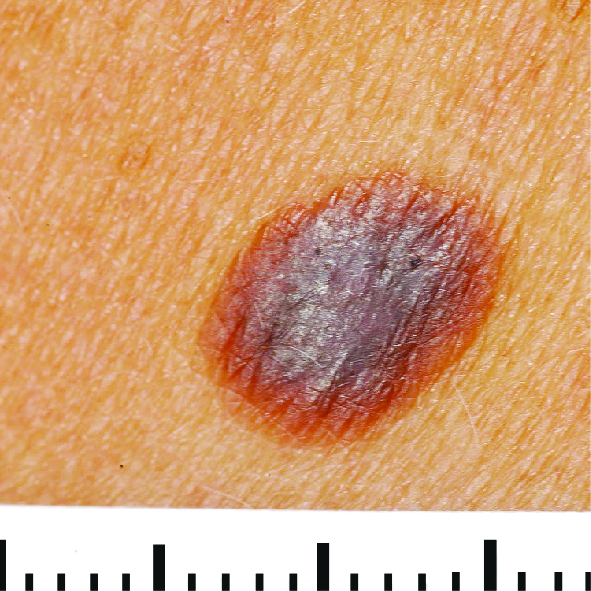
Examples of melanoma in situ




Radial growth phase melanoma
This is a melanoma that has started to grow but still mainly sideways in the skin rather than downwards into deeper layers. The most common type of melanoma is known as a superficial spreading melanoma, and early superficial spreading melanomas are in radial growth phase. These melanomas typically have an irregular shape and a variable or mixed colour.
The diagram below shows the appearance of a radial growth phase melanoma. The cancer cells are shown in black.
People with this type of melanoma should be cured by surgery. The melanoma is unlikely to come back after it has been removed.

Examples of radial growth phase melanomas



Vertical growth phase melanoma
This is a melanoma that has started to grow downwards into the skin. Again the diagram below shows the cancer cells in black. This is a potentially more serious type of melanoma.
The likelihood of it coming back or having spread to other parts of the body varies and depends on how deeply within the skin it has grown.
This depth is known as the Breslow thickness. Vertical growth phase melanomas may develop from radial growth phase melanomas.
There are different types of melanoma, other than superficial spreading melanoma. They are named according to either which body part they started from or the way that they have grown. The treatment is generally the same regardless of what type of melanoma you have.

Examples of vertical growth phase melanomas

Is melanoma serious?
Melanoma is considered to be the most serious type of skin cancer as it is more likely to spread (metastasize) from the skin to other parts of the body than other types of skin cancer.
If melanoma has spread to other parts of the body, those deposits are known as secondary melanoma (secondaries/metastases). However, the majority of patients never have any further recurrence of their disease.
It is possible to estimate the risk of the melanoma coming back, although of course it is only ever an estimate. Normally the thickness of the melanoma, and whether the skin is intact over the melanoma, are used to define the so-called stage of the primary melanoma. Other features can be seen which can also adjust your stage of melanoma, this can be discussed with you. The AJCC staging system is used internationally and stages melanoma from 1 to 4. Stage 1 is the earliest melanoma and stage 4 is the most advanced.
Stage 1 and 2 melanomas are present in the skin only and have not spread elsewhere in the body.
Stage 3 and 4 melanomas are those that have spread to other parts of the body.
There are statistics available on the likelihood of melanoma recurrence (secondary melanomas) for each stage. Most patients at diagnosis are either stage 1 (1A or 1B) or stage 2 (2A, 2B and 2C). In Leeds we offer sentinel node biopsy which is an additional staging tool which is discussed below. It is a good idea to think about how much detail you want before you talk to your doctor about the risk of melanoma coming back.
Back to topDealing with the details
Dealing with the details of treatment at diagnosis can be emotionally trying.
It may be difficult to take everything in that the doctor tells you during the consultation. This leaflet is designed to add to the information that the doctor gives you, but your own doctor and their team remain the best source of information for you.
If you are not clear about anything during your treatment, then ask. You may want to write down a list of questions to take with you to your appointments. If after leaving the hospital you have queries or concerns then get in touch with the melanoma nurse specialist team. Their contact information is in the information pack.
Back to topDo I need further surgery?
After removal of a melanoma the doctor will discuss with you how much more skin needs to be removed. It is true to say that this remains a controversial issue but there is some agreement around the world. Your doctor will discuss with you how much skin will need to be removed as the recommended margin depends on the thickness of the melanoma. The purpose of this further surgery is to try and make sure that no cancer cells are left behind in the nearby skin.
For melanoma ‘in situ’ it is thought unnecessary to remove a lot of normal skin from around the melanoma. Normally a few millimetres is sufficient and often therefore no further surgery is needed after the initial diagnostic surgery.
For all other melanomas it is usual to take between one and two centimetres of normal skin from around the melanoma. This is called a ‘wide local excision’.
The final decision about the extent of further surgery should be made as a result of a discussion between you and your surgeon, considering safety and the cosmetic result.
If a small further operation is needed this is often performed by the dermatologist. If a larger operation is required, then a plastic surgeon is usually asked to do it.
Swabs are usually taken from the skin before further surgery to test for super bugs such as MRSA which would have to be treated before the operation to reduce your risk of wound infections.
What will my scar look like?

This will depend upon several things:
- Where on the body the wound is. Lumpy scars called ‘keloids’ may result from operations. They occur most commonly on the upper arms, the lower back and over the breast bone. The scar feels hard and itchy at first but these scars fade and soften with time.
- The amount of spare skin available to cover the wound and therefore whether a skin graft is needed.
- How much normal skin needs to be removed from around the melanoma.
- Individual healing, as some people heal better than others.
- Whether there are any complications such as infections.
What is a skin graft?
When the removal of a melanoma leaves a gap too big to fill with existing skin, a skin graft will be needed. This operation is usually, but not always, carried out using a general anaesthetic (when you are asleep).
Most skin grafts now are full thickness grafts. Others are called split skin grafts. A special knife is used to take off the top layer of skin from another area of the body (often the thigh); this is known as the donor site.
This knife is a bit like a Dutch cheese knife, which slices off a thin sheet of skin, which is composed mainly of the epidermis (the top scaly layer of the skin). This is the graft, and it is placed carefully over the gap and is stitched to the edge.
The donor site and the grafted site will then both be firmly bandaged. The purpose of the bandage is to keep the grafted skin in position so that it will settle down and start to grow. Sometimes if the grafted site is near a joint then the surgeon may place the limb in plaster to prevent movement till the graft has taken.
Possible complications of skin grafts
Infection in the wound or breakdown of the graft may occur occasionally and when this happens then the surgical result may be poorer.
Wounds usually look worse soon after the surgery than they do later. Redness fades and in time the skin takes on a more normal appearance. Don’t panic if your wound looks awful to you when you first see it. It will get better.

The operation often leaves a depression or dint in the skin so that the shape of the body is changed and many patients find this difficult to cope with. However, this usually fills in a good deal with time, and most patients feel content after six months or so. Usually however the scar continues to get better for years.

The donor site
The bandages will be taken off after seven days or so. The donor site will look and heal up like a graze. It often feels more sore, and for longer, than the grafted site. Both photographs here show healed donor sites.


Flaps
Sometimes it is possible to fill the gap using something called a ‘flap’. This means moving a piece of skin around on a ‘stalk’ to fill the gap. This technique is very valuable because the normal body shape is often retained.

This photograph shows the scar resulting from a flap, six months after surgery. The scar will become less red with time. The scar is long but the shape of the back is normal.
Back to topWhat is sentinel node biopsy?
If melanoma recurs, it usually comes back in a swollen gland (also known as lymph glands).
A sentinel node biopsy is currently an optional test to see whether there has been spread of a small number of melanoma cells to those glands, early before the swelling can be detected. It is the most accurate way of detecting any spread of melanoma cells. It is not routine for all patients, but if your doctor recommends it is usually following a discussion by the team of your case, as to whether it is clinically beneficial to you.
The Sentinel node biopsy is performed at the same time as the Wide Local Excision (WLE), under general anaesthetic, while you are asleep. The first part of a sentinel lymph node biopsy is called a lymphoscintiogram. This involves injecting a radioactive liquid into the skin near to where the melanoma was located.
Only a small amount of radioactivity is required which is not harmful to you or to anyone else. It can take a period of 2-3 hours for the dye to travel to the nodes.
A scan, using a gamma camera (shown here), is then carried out to see which node or nodes the liquid reaches. This identifies the closest lymph node to the melanoma (the sentinel node) and the one most likely to contain melanoma cells.


An example of a scan showing the highlighted nodes.
Once the node is identified by the gamma camera, the skin overlying the node is marked (shown here in the picture). There may be more than one node that is identified.

The second part of the test takes place at the time of the WLE when the surgeon injects blue dye into the same place that the radioactive liquid was injected. This makes the node visible to the surgeon. The diagram below shows the process of identifying the Sentinel Node.
The combination of the radioactive liquid and blue dye is the best way to identify the sentinel node (shown on the next page). The nodes are arranged like a bunch of grapes.
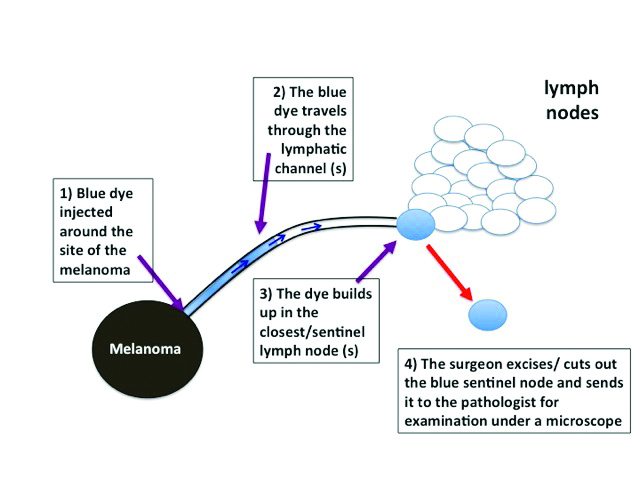
The lymphoscintigraphy and blue dye helps your surgeon to pick out the grape within the bunch, which looks after the part of your body where your melanoma was.

There is a possibility of an allergic reaction to the dye but this is very rare. The surgeon removes that node (or in some cases 2-3 nodes), the operation is usually less than an hour. The pathologist then looks for melanoma cells in the node and the WLE under the microscope.
If a melanoma is removed from the leg then the sentinel node is usually in the groin. If the melanoma was on the abdomen, then the sentinel node could be in the groin or under the arm. Sometimes when the melanoma is on the trunk then there might be more than one sentinel node, for example one in the groin and one in the arm pit. When the melanoma was on the head then too many glands might show up as sentinel nodes and in these circumstances then the surgeon will tell you that sampling a lymph gland would not be sensible.
After the sentinel node biopsy, there maybe some discomfort at the operation site. There will be a scar where the lymph node(s) is removed. You may also notice some loss of sensation (numbness) in the area. Infection is uncommon, but if it occurs you will need antibiotics.
Pathology of sentinel node biopsy
During the following weeks the pathologist will look carefully at the removed lymph gland and the WLE, under the microscope, for tiny deposits of melanoma. These are often referred to as micro-metastases (see the picture below). Patients normally get the results 3-4 weeks after the surgery.
If a small melanoma deposit (micro metastases ) is detected then the doctor will discuss the options with you. Historically this may have involved removing the remaining nodes. This is known as a lymph gland dissection/completion lymphadenectomy/ lymph node clearance. If micro-metastases are detected (a positive sentinel node biopsy) then the doctor will discuss management of this with you.
If the deposits of melanoma found are larger or there are multiple deposits, they may recommend that the rest of the glands in this area be removed. This is known as a lymph gland dissection/completion lymphadenectomy/lymph node clearance.
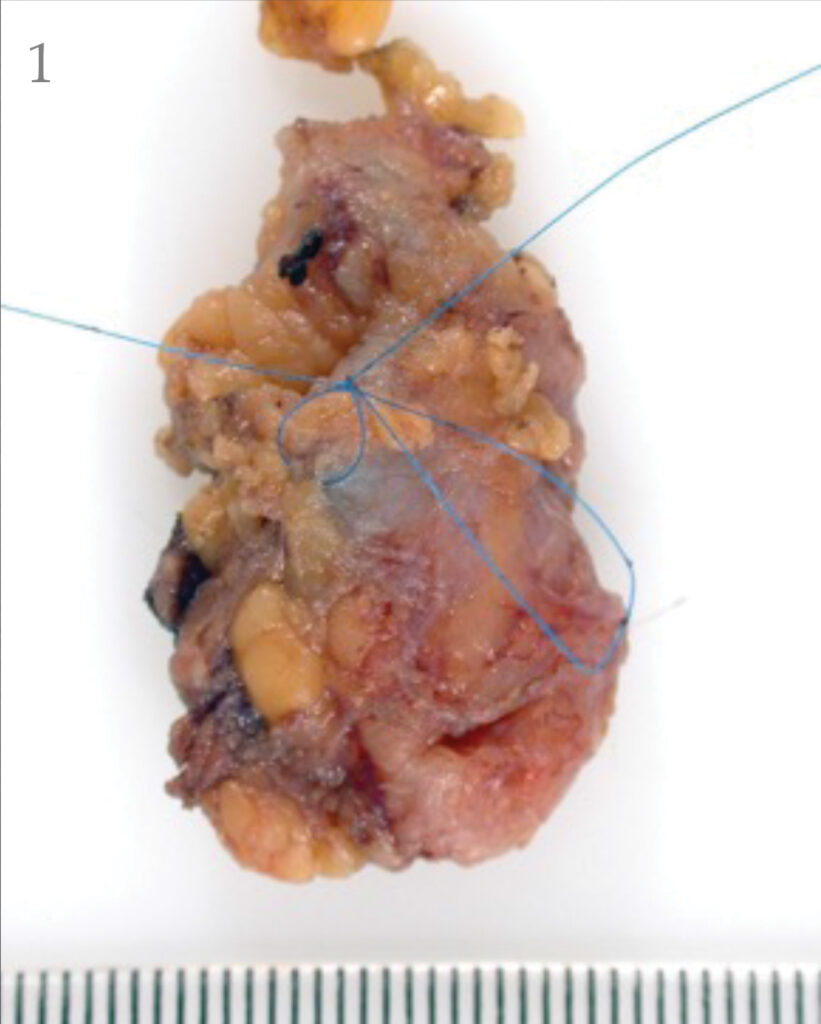



- Sentinel node with radioactive hotspot marked.
- Sentinel node with hotspot inked.
- Sentinel node with hotspot ink visible.
- Sentinel node pathology with hotspot ink visible near the melanoma deposit in the node.
If the deposit/deposits of melanoma are very small in the lymph node you may not require any further treatment apart from the regular three monthly monitoring, which will include skin and lymph node examination.
If the sentinel node biopsy is negative, it is reassuring because it means that there is less chance of further trouble from the melanoma. It does not mean that the melanoma will not come back, but the chances are much lower.
How useful is sentinel node biopsy?
Sentinel lymph node biopsy remains optional because there are advantages and disadvantages to the procedure. It is your choice as to whether you want to have this operation or not. Although sentinel node biopsy seems like a good idea, there is no evidence as yet that removing the glands early in this way improves the chances of survival from melanoma.
This chart highlights the possible advantages and disadvantages of the Sentinel Node Biopsy
| Possible advantages of sentinel lymph node biopsy | Possible disadvantages of sentinel lymph node biopsy |
| The operation helps to find out whether the cancer has spread to the lymph nodes. It is better than ultrasound scans at finding very small cancers in the lymph nodes. | The purpose of the operation is not to cure the cancer. There is no good evidence that people who have the operation live longer than people who do not have it. |
| The operation can help predict what might happen in the future. This information is useful for many.A positive sentinel node biopsy may allow access to adjuvant therapies (risk reducing treatments ). | The result needs to be interpreted with caution. Of every 100 people who have a negative sentinel lymph node biopsy, around 3 will subsequently develop a recurrence in the same group of lymph nodes. |
| People who have had the operation may be able to take part in clinical trials of new treatments for melanoma. These trials often cannot accept people who haven’t had this operation. | A general anaesthetic is mostly needed for the sentinel node operation whereas wide local excision alone can usually be done with local anaesthetic |
| The complications from the complete lymph node clearance are reduced when the deposits of melanoma are micro metastases (positive sentinel node) and removing these glands before the melanoma grows into a larger lump is an easier procedure. | The operation results in complications in between 4 and 10 out of every 100 people who have it.Complications include:InfectionBleedingNumbness/tinglingScarring – another scar is created and sometimes several scars if more than one lymph node shows up on the scan.Seroma – sampling /removing lymph nodes may leave a swelling called a seroma, which is a build up of fluid that cannot drain through lymphatics as it once did before the surgery. A seroma may take a while to settle after surgery. Extremely rarely the seroma might persist.Lymphoedema – Occasionally there may be some permanent swelling of the limb called lymphoedema. |
It is important to continue to assess the value of sentinel node biopsy and it is very possible that views may change, but to date sentinel node biopsy remains an operation that is offered in Leeds. Sentinel node biopsy has a more valuable role ultimately in selecting patients for treatment with adjuvant therapies.
Back to topWhat is adjuvant therapy?
Adjuvant therapies
An adjuvant therapy is one that reduces the risk of cancer recurrence (reducing the risk of secondaries). Some adjuvant therapies have been approved for use in melanoma patients who have a higher risk of developing recurrence. Your consultant will discuss this option with you . These treatments may be given as tablets ( targeted therapy) or as infusions (immunotherapy). Adjuvant treatment starts within 12 weeks of surgery and continues for a year.
What is a clinical trial?
A clinical trial is a study designed to see whether a treatment works or not. The best way to find this out is to carry out a randomised clinical trial.
The patient is counselled about the trial and if they choose to take part a computer then ‘decides’ whether they will receive the trial treatment or not. That is, the decision as to whether the patient has trial treatment is made randomly by the computer.
Some of these studies will be comparing the effect of treatment with observation. That means that half the patients in the study will have follow-up with observation and the other half will have the experimental treatment. In other studies, the trial treatment will be compared with a standard treatment.
Sometimes, the patients who do not receive the active treatment will receive a placebo, a harmless but ineffective injection or pill.
Back to topWebsites for information about melanoma
Cancer Research UK
Wessex Cancer Trust
MARC’s Line
Macmillan Cancer Support
BBC health information
Marie Curie Cancer Care
Melanoma Focus
The Melanoma Genetics Consortium
Information and advice
Leeds Cancer Support
Leeds Cancer Support complements care provided by your clinical team. We offer access to information and a wide range of support, in a welcoming environment for you, your family and friends. We can be found in the information lounges in Bexley Wing and also in the purpose built Robert Ogden Macmillan Centre.
The Sir Robert Ogden Macmillan Centre
The Centre is on the St James’s Hospital site and offers a variety of support services including counselling, support groups and complementary therapies. These therapies include Reiki, relaxation and visualisation, hand and foot massage and many others. Open from 10am – 4pm Monday to Friday.
Contact numbers for Leeds Cancer Support
Information Lounge Level 1 Outpatients Department
Open from 10am – 4pm. Tel: (0113) 206 8816
Information Lounge Level -2 Radiotherapy Department
Open from 8.30am – 4.30pm Tel: (0113) 206 8940
Sir Robert Ogden Macmillan Centre
Open from 10am – 4pm. Tel: (0113 206 6498)
All the above services can be emailed on:
Maggie’s Centre
A Maggie’s Centre is next to the visitors car park at St James’s Hospital. The centre provides drop in support for all patients and their families, as well as activities to help promote health and wellbeing.
Back to topMacmillan Cancer Support
Freephone 0808 808 0000, 9am to 6pm Monday to Friday
A textphone service for deaf and hard of hearing people on 0808 808 0121.
website: www.macmillan.org.uk
Back to topRefreshments
There is a restaurant and coffee shop available on Level 0, Bexley Wing, which are open daily. They serve drinks, light snacks and hot meals. Vending machines are also available in the main radiotherapy waiting room and Level 0. There is also a shop on Level 0 with books, papers and snacks.
