Leeds Community Cardiac Rehabilitation Team
Please note this is not an emergency number. If you require urgent medical attention please phone 999
Introduction
This booklet has been written to provide you with information that will guide and assist your journey through heart surgery and help you with your recovery.
It is important for you to use this booklet for reference before and after your surgery. Please ask the ward nurses, cardiac rehabilitation nurses and doctors any questions that you may have. We suggest that you show this booklet to your family and friends so that they can help to support your recovery and ask any questions they may have.
Currently, Leeds Community Cardiac Rehabilitation Team will take patients who have had coronary artery bypass surgery or valve repair or replacement into their service. The advice in this booklet is still relevant for patients who have had other types of cardiac surgery.
The Heart
The heart is a hollow muscular pump which pumps blood around the body.
It is about the size of your fist and is situated in the chest between the lungs, slightly to the left.
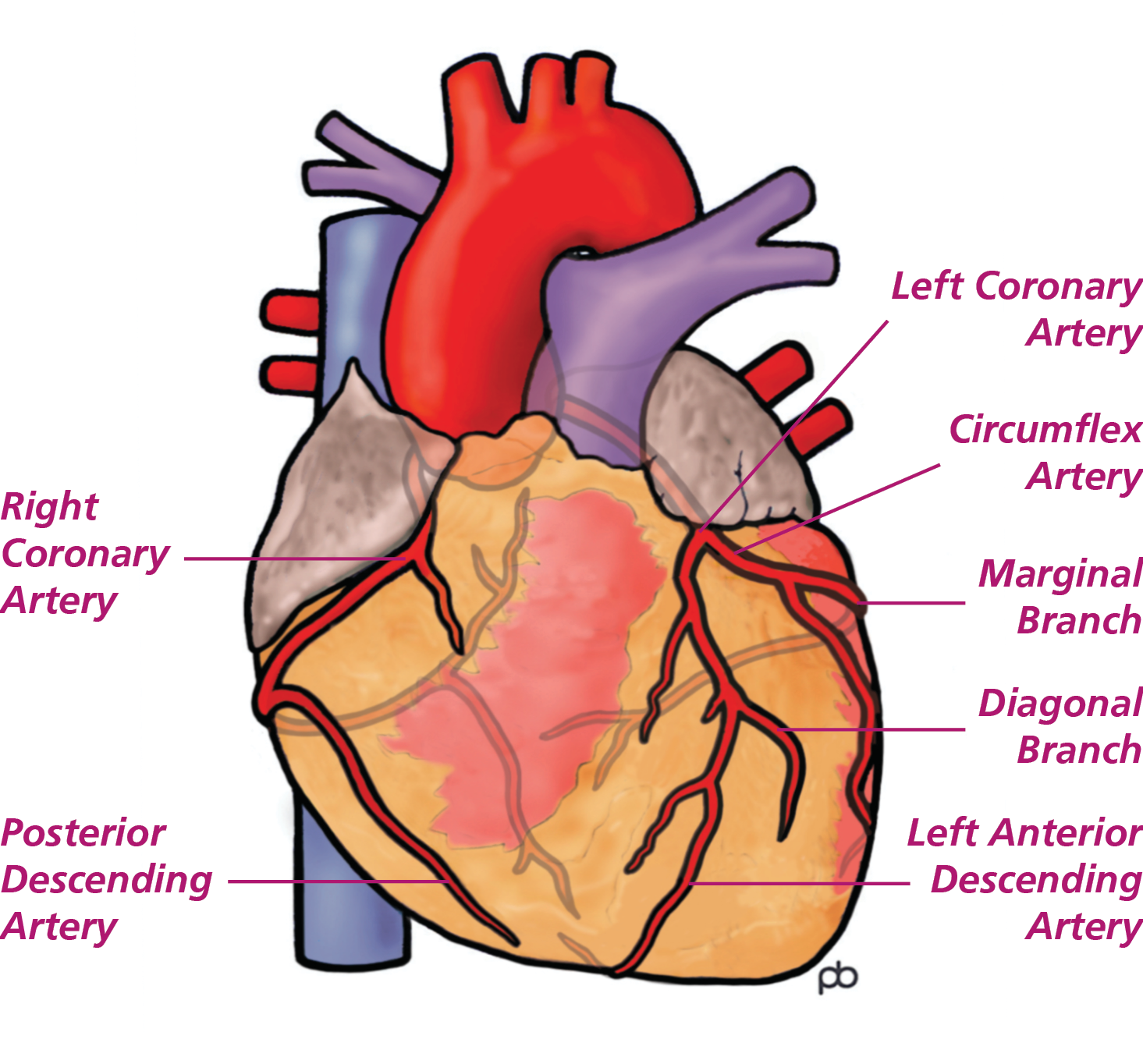
The large blood vessels that begin at the heart carry blood to the lungs and body and back again, whilst smaller blood vessels covering the surface of the heart (coronary arteries) supply the heart muscle with blood.
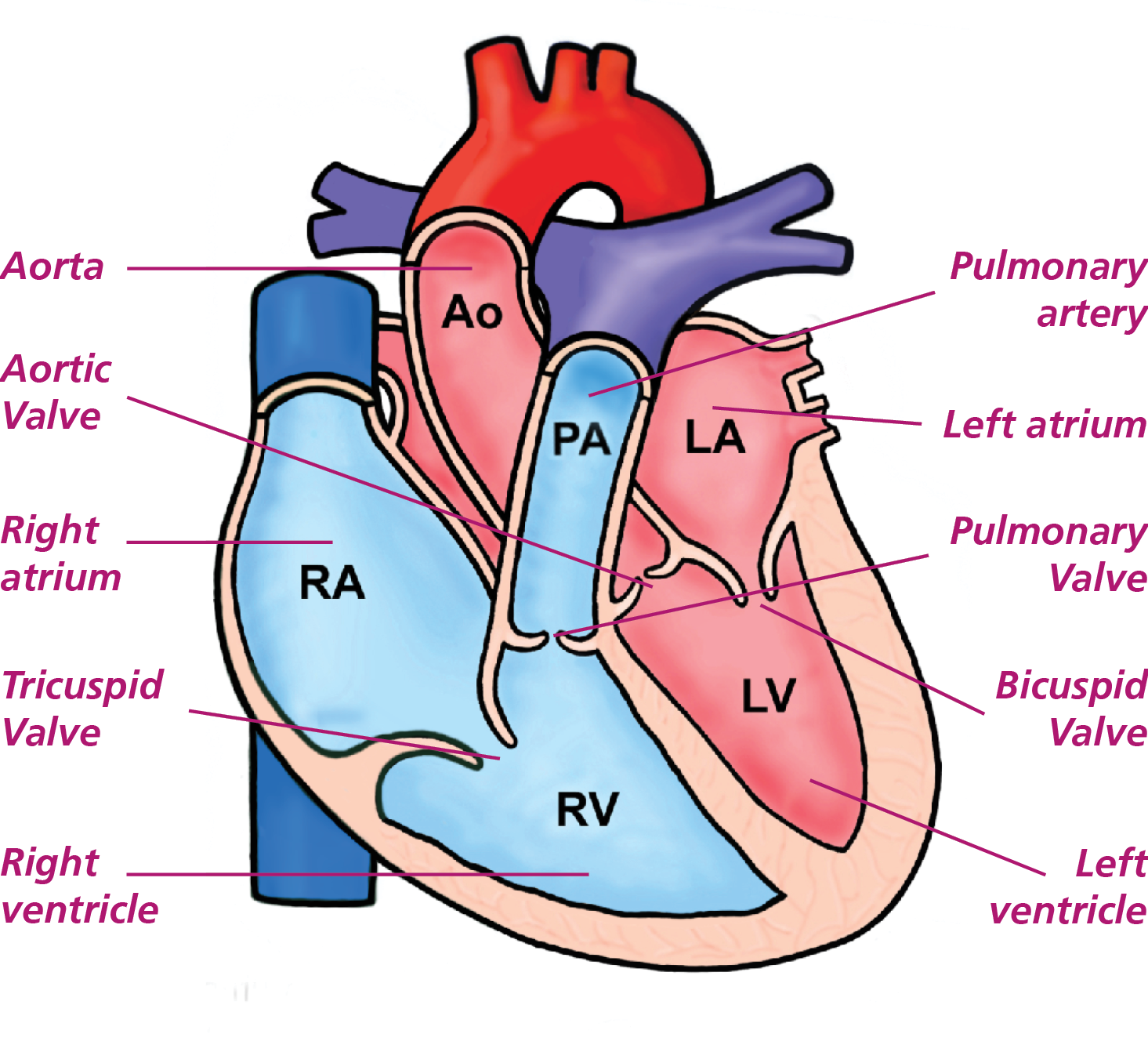
Inside the heart are four chambers. The upper chambers are the right and left atria and the lower chambers are the right and left ventricles.
The heart receives blood that is low in oxygen from the body, into the right atrium and then the right ventricle pumps it to the lungs.
The left atrium then receives blood rich in oxygen from the lungs and the left ventricle pumps it round the body (see diagram).
There are four valves which separate the chambers and prevent blood flowing back into each chamber of the heart when it is not pumping.
Looking after your heart
Risk factors for heart disease
There are a number of factors that can contribute to the development of heart disease. These factors are known as risk factors. They can be divided into being ‘modifiable’ or ‘non-modifiable’.
Some risk factors cannot be changed. These are known as non-modifiable.
Non-modifiable risk factors
These include:
- Family history – CHD can run in families
- Age – The risk of developing heart disease increases with age
- Gender – Men over 45 on average are more at risk. Women are protected by the hormone oestrogen until after the menopause, then women become as vulnerable to heart disease as men
- Ethnic origin – People from the South Asian population are more at risk of developing heart disease
Modifiable risk factors
These will be discussed in detail in the following pages. If you would like further information about risk factors, speak to your Cardiac Rehabilitation Nurse or Doctor. The modifiable risk factors for CHD include:
- Smoking
- Being overweight
- High blood pressure
- Alcohol
- Cholesterol
- Lack of exercise
- Diet and lifestyle
- Uncontrolled diabetes
Fortunately, you can control many of the modifiable factors that contribute to the narrowing of the coronary arteries. Your Cardiac Rehabilitation Nurse can help you set realistic, achievable goals to reduce the risk factors that apply to you.
Smoking
Stopping smoking is the single most important thing you can do to improve your health.
How does smoking affect my health?
When you smoke, the chemicals released into your body make your blood sticky.
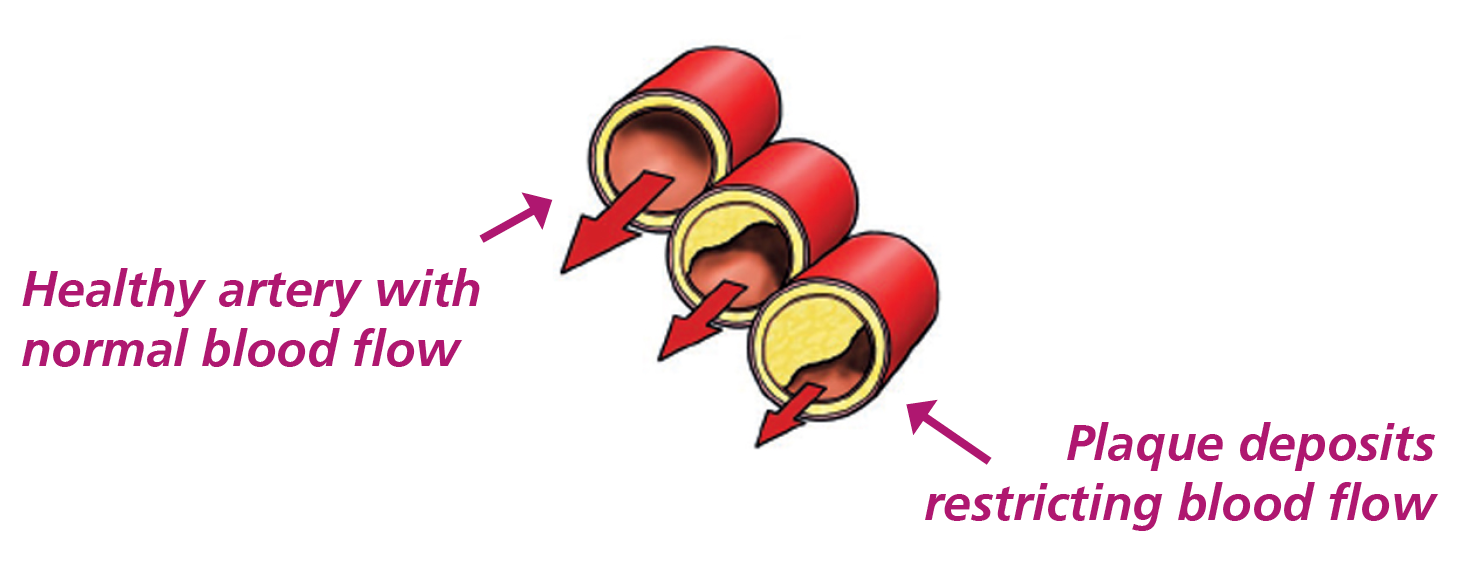
Smoking encourages fatty deposits to collect in the lining of the arteries of the heart. This narrows the arteries which can reduce blood flow to the heart. These fatty deposits can also rupture causing a tear in the lining of the artery causing the fatty deposits to leak out and block the artery, which may cause a heart attack.
Smoking tends to increase your blood cholesterol levels. It reduces the HDL (the good cholesterol), thereby increasing the LDL (bad cholesterol).
When you smoke a cigarette, the burning process produces a gas called carbon monoxide. This gas is poisonous. In the body it sticks to the red protein of blood cells, making the blood less able to carry oxygen. This will starve the heart of vital oxygen and nutrients.
Nicotine, in cigarettes, stimulates the body to produce adrenaline. This makes the heart work harder and can raise blood pressure. The high nicotine levels in cigarettes are the addictive part of the cigarette.
Some of the health benefits, from the minute you stop smoking:
- 20 mins – Blood pressure and pulse return to normal.
- 1 hour – Your circulation improves, your hands and feet feel warmer.
- 8 hours – Nicotine and carbon monoxide levels fall and the oxygen in your blood begins to return to normal.
- 1 day – Carbon monoxide is now completely removed from the body, the lungs work more effieciently.
- 2 days – Nicotine is now removed from the body, your taste and smell improves.
- 3 days – The lungs begin to clear mucus and smoking debris, you may develop a cough but your breathing will soon become easier.
- 2 weeks – Withdrawal symptoms begin to ease, walking and daily tasks should become easier.
- 1 month – Withdrawal symptoms have now stopped, your breathing and energy levels continue to improve.
- 6 months – Risk of heart attack, cancer and other smoking related diseases begins to fall and you feel better about yourself!
What support is there to help you stop smoking?
- Whilst in hospital, you can ask any of the ward staff for advice or help. Your Inpatient stop smoking team will discuss stopping smoking with you and explain approaches to stopping as well as the support available to you.
- Support from healthcare professionals will start in hospital and can continue at home. When you make the decision to stop smoking, you will be given advice on preparing to stop and how to cope once you have stopped. You will also be advised on medication which may be appropriate to help you stop.
- The inpatient stop smoking team can help you put a plan together for how you will stop smoking before you go home. Once home, Leeds Stop Smoking Service can offer continued support. The inpatient stop smoking service can arrange a referral for you once you have been discharged from hospital. If you decide to stop smoking at any time after leaving hospital you can contact Leeds Stop Smoking Service to discuss support on 0800 169 4219. The service provides support sessions throughout Leeds, including one-to-one or group sessions.
- Your community pharmacy might also offer smoking cessation support, advice and medicines. Please ask your pharmacist for advice.
To find out more, ask the ward staff, your cardiac rehabilitation nurse, your pharmacist or phone One You Leeds on 0800 169 4219 or self refer through their website.
Nicotine replacement therapy (NRT)
Nicotine Replacement Therapy (NRT) replaces a small amount of the nicotine that you used to get from cigarettes. It is the addictive nature of nicotine that makes it hard for many people to quit. NRT provides you with some help with the addiction and allows you to deal with the habit side of smoking first. Remember you are four times more likely to quit for good using a combination of medication and specialist support.
Your cardiac rehabilitation nurse or Stop Smoking advisor can advise you on which types of NRT would be most suitable for you and which products can be combined to achieve the best outcomes.
The use of medications to stop smoking
There are two medications that can also be considered to help you stop smoking; these should only be considered under advice from a specialist who can prescribe, such as the Stop Smoking advisor or your GP. Using medications such as these can double your chances of stopping smoking. However, they can have side effects and may not be recommended in certain health conditions.
The use of e-cigarettes to stop smoking
- Electronic Cigarettes or Vapourisers do not contain tobacco; they create vapour from liquid nicotine. E-cigarettes are not licenced for use as Nicotine Replacement Therapy (NRT) at present.
- Public Health England state that e-cigarettes are 95% less harmful than smoking.
- E-cigarettes are the most popular quit smoking aid and when combined with specialist stop smoking support can be the most effective way to quit smoking for good.
High blood pressure
Blood pressure is the force that circulating blood puts on the artery walls. When blood pressure is high, there is more pressure on the artery wall than usual. Some people have high blood pressure and do not know they have it.
This extra pressure damages the smooth lining of the arteries and makes it easier for cholesterol and fat to build up along the artery walls. As the arteries become clogged with these fatty layers (atherosclerosis), less blood gets through. This causes the heart to beat harder as it tries to pump blood through narrowed arteries. If untreated, high blood pressure may in time damage the heart, brain and kidneys. It is a leading cause of heart attacks and strokes, heart or kidney failure.
The exact cause of high blood pressure is not fully known for many people. High blood pressure can be treated and lowered with medication.
How do I control blood pressure?
- Get your blood pressure checked as often as your doctor suggests.
- Stop smoking.
- Take your medications regularly as prescribed.
- Reduce your salt intake and try to avoid processed, convenience and fast foods.
- Fruit and vegetables provide us with a good source of potassium which can help control your blood pressure. Aim for five portions a day.
- Reduce stress by learning ways to relax and by exercising.
- Lose weight if needed. The heart pumps harder to supply an overweight body with blood and oxygen.
- Cut down your alcohol intake.
Cholesterol
Cholesterol and triglycerides are fatty chemicals in the blood. The liver makes them from fats in foods. There are two main types of cholesterol; LDL ‘bad cholesterol’ which carries cholesterol from the liver to the rest of the body, and HDL ‘good cholesterol’ which returns excess cholesterol to the liver.
While foods with plant stanols and sterols are thought to reduce the absorption of cholesterol from the gut (British Nutritional Foundation), they do not provide sufficient reduction in cholesterol and should not replace the medicines prescribed to lower cholesterol. They can be taken alongside the cholesterol-lowering medicines that you were prescribed. Plant stanols and sterols are usually added to particular spreads and yoghurts and they are also found naturally in nuts and seeds and some fruits and veg.
If you have high levels of cholesterol and triglycerides, your risk of CHD is greater. High levels of LDL cholesterol stick to the walls of your arteries and make plaque. This plaque blocks the arteries, interfering with the blood flow which can make a heart attack more likely.
Many people with high blood cholesterol will only need advice about diet, a healthy lifestyle and possibly future blood cholesterol monitoring. The nutrition section later in this book provides information about diet. For others, particularly those who have an inherited type of high blood cholesterol or other risk factors for CHD, different blood tests and simple medical investigations may be needed. If this applies to you, effective medications such as statins are available. The treatment for high cholesterol is now as routine as that of other common conditions. Treating raised blood cholesterol is a positive way you can do something to avoid future heart problems.
The aim of your cholesterol lowering medications is to reduce the bad cholesterol (LDL) to less than 1.8 mmol/L. If LDL is not measured then we aim for more than 40% reduction in non-HDL cholesterol (which is your total cholesterol excluding good cholesterol).
It is recommended that once starting cholesterol-lowering medications, you have your cholesterol checked after three months and then at least yearly, unless advised otherwise. You can arrange this with your local GP practice.
Further dietary and nutritional advice is available further down this page.
Diabetes
What is diabetes?
Diabetes is when either the body does not produce enough insulin, or the insulin that is made does not work properly. This means glucose (sugar) cannot get into your cells. Glucose stays in your blood, causing the level of glucose to be too high. Diabetes can develop later in life, usually after the age of 40.
This type of diabetes (Type 2) is strongly linked with being inactive, over-weight and where there is a family history of diabetes. In certain populations it occurs more often. This is particularly true of people of South Asian and African-Caribbean origin living in this country.
You can greatly reduce the risk of developing Type 2 diabetes by taking regular exercise and controlling your weight.
What effect does diabetes have on the heart?
Diabetes appears to affect the heart in different ways:
- High glucose levels in the blood affect the walls of the arteries, making them more likely to develop atheroma.
- Diabetes can affect the heart muscle itself, making it a less efficient pump.
- It increases the damage done by smoking, high blood pressure and high cholesterol.
- People with Type 2 diabetes often have high triglyceride levels and low levels of HDL cholesterol (the protective type of cholesterol).
- It can affect the nerves to the heart, so symptoms are not felt in the usual way (some patients with diabetes do not feel any pain with a heart attack). This can lead to difficulty and delay in diagnosis of a heart attack if you have diabetes.
What can I do about it?
Diabetes cannot be cured, but it can be managed and controlled. There are two main aims of diabetes treatment. One is to resolve the symptoms of diabetes and the other is to prevent the complications which diabetes can cause.
Diabetes can be controlled by one or more of the following: diet, physical activity, tablets and insulin.
If you have diabetes, you are more than twice as likely to have a heart attack or stroke as someone without diabetes. Your risk of a heart attack is the same as someone who has already had a heart attack.
People with diabetes have a higher chance of also developing high blood pressure, circulation problems, nerve damage, damage to the kidneys and the eyes. The risk is particularly high if you are also overweight, smoke and are not physically active.
You can greatly reduce your risk of developing any of these complications by controlling your blood glucose, blood pressure, eating a healthy diet and taking regular exercise. It is important to attend your regular check ups, where you will have blood glucose, blood pressure, kidney function, eyes and feet checked.
You will have had a routine blood test for glucose whilst in hospital.
Further information on diabetes is available on request.
The operation
Details of your specific operation will be discussed with you. Please speak to your healthcare team if you have any questions.
Coronary artery bypass graft
Why do I need surgery?
This type of surgery is required to improve the blood supply to the heart muscle. The coronary arteries can become narrowed due to build up of fatty deposits (coronary heart disease). Therefore not enough blood can get through them to supply the heart muscle with oxygen and nutrients. The operation can relieve angina and reduces the risk of permanent damage to the heart muscle.
The coronary arteries
What is a coronary artery bypass graft?
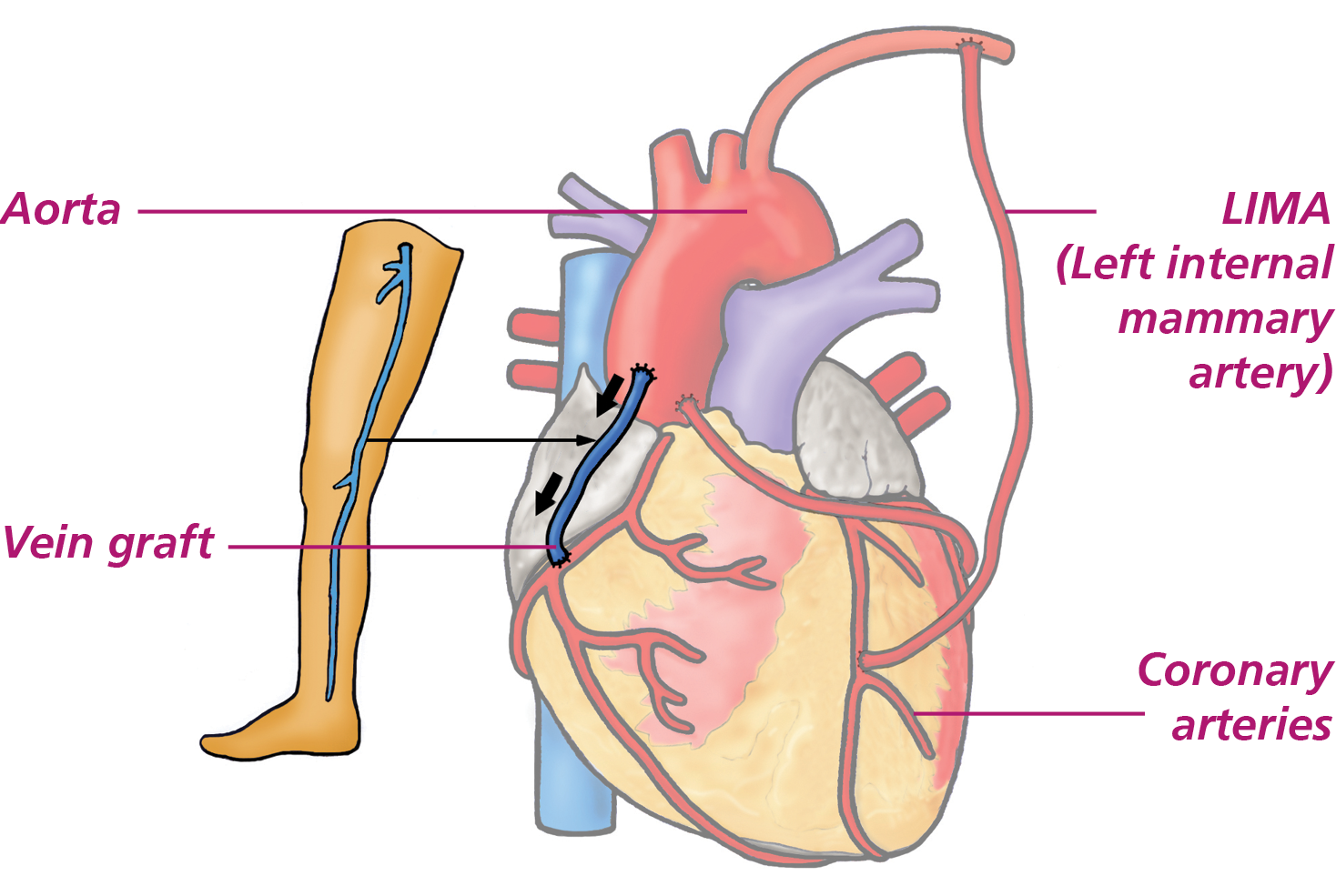
A coronary artery bypass graft improves the blood supply to the heart muscle by bypassing blocked or narrowed coronary arteries. Blood vessels are taken from your arms, legs or chest wall and used to redirect blood from the aorta (see diagram on page 7) to the areas of heart muscle which are not receiving enough blood. The number of bypass grafts used depends upon the number of narrowed or blocked coronary arteries you have.
What happens during the operation?
The majority of heart operations leave you with a scar down the front of your chest. This is because your breast bone (sternum) will be cut so that the surgeon can get to your heart. If you have a different scar your doctor can explain why they used this particular method. Once your chest is opened, it is necessary to stop the heart from beating. The doctors do this using a piece of equipment called a cardiopulmonary bypass machine. This machine takes over the work of the heart and lungs, supplying blood and oxygen and pumping it around the body. This means that the surgical team can then safely perform your operation.
Once the operation is completed the cardiopulmonary bypass machine is turned down and your own heart starts beating by itself. Once the surgeons are happy with your heart’s condition, the cardiopulmonary bypass machine is removed. The final stage of the operation is to close your chest.
How is my chest held together?
Your breast bone is held together with stainless steel wire and the muscle and skin are stitched. Your chest is held together firmly and will not split apart when you are deep breathing or coughing even though it might feel like that at first! It does take about three months for the breast bone to be fully healed. The steel wires do not usually need to be removed (they would only need removing if they cause any problems in the future, this is rare). They do not set off the metal detectors at airports.
Coronary artery bypass graft
Which blood vessels are used?
A blood vessel from the chest wall is called the left internal mammary artery. It is known as the LIMA. The LIMA normally supplies blood to your chest wall, but can be redirected and used to bypass a blocked or narrowed coronary artery. NB: It is useful for you to know if your surgeon used this artery because you may experience certain typical aches and pains (see section on aches and pains). Other blood vessels which may be used are either leg veins, arm veins, arteries or all three.
Valve surgery
Why do I need valve surgery?
As previously mentioned, your heart has four valves: these are the tricuspid, pulmonary, aortic and mitral. These valves regulate the blood flow through the heart. If any of the heart valves leak or become narrowed, the blood flow alters and interferes with the heart’s normal function. This can lead to symptoms such as breathlessness, tiredness and swollen ankles. When this happens surgery may be required.
What happens during the operation?
The surgical team open your chest as described for coronary artery bypass grafting and if possible they repair the damaged valve. If they are not able to repair the valve, then it will be removed and replaced with an artificial valve.
Artificial valves
There are two types of artificial valves available: biological or mechanical. As each person is different the surgeon will help you to decide which will be the best for you.
The valves are designed to work like normal valves. However, people who have mechanical valves in place often say they can hear a ticking sound. This is quite normal and often fades in time.
How can I look after my new valve?
You can help by taking good care of your teeth, brushing them twice a day and having regular check-ups at the dentist.
Dental procedures and dental abscesses increase the risk of bacteria entering the bloodstream and infecting your new valve.
You may need to take antibiotics before some dental treatment or minor operations. Always tell the dentist about your artificial heart valve before you proceed.
I have heard that I may have to take warfarin. What is it?
Warfarin is a medicine which helps to prevent the blood from forming clots on your new valve.
For how long will I have to take warfarin?
If you have a mechanical valve, you will need to continue taking warfarin for the rest of your life. The surgeon may also ask you to take warfarin or alternative anticoagulation medication if your heart is beating in an irregular rhythm known as atrial fibrillation (AF). You may need to continue to take the warfarin for a limited time even if your heart returns to normal rhythm.
Will I need regular blood tests?
If you are on warfarin, to make sure that you are receiving the right dose, it is necessary to take regular blood samples, both in hospital and once you have gone home. It is very important that you are taking the correct amount of warfarin each day, as too little warfarin will not protect your valve from potential blood clots.
The good news is that the testing can be arranged at a hospital closer to home or sometimes by your g.P. And once the correct dose has been found for you, the testing becomes less frequent.
Can I drink alcohol when taking warfarin?
Alcohol can affect the way Warfarin works so check with the staff on the ward for further information.
Other important things to remember:
Too much warfarin can cause bleeding, so look out for these signs:
- unexplained bruising
- nose bleeds
- bleeding gums when brushing teeth
- dark or black stools
- blood in the urine
- If any of these occur see your G.P. at once. Never alter your warfarin dose without asking your doctor first.
If you are taking warfarin consult your doctor if:
- You suspect you are pregnant or have plans to become pregnant.
- You need to take anything that contains aspirin e.g. flu remedies. Try to avoid these and use paracetamol instead. (If in doubt, ask your local chemist).
L16 Cardiac Surgery Ward
Ward 16 is the ward where you will be admitted to before your heart surgery. It is on F floor in Jubilee Wing at the Leeds General Infirmary (LGI). It is a mixed sex ward, however male and female toilets and bathroom facilities are available and the bays are single sex. The only bay that could be mixed sex is the higher observation bay where you may go following the intensive care and high dependency unit.
Some things to think about before admission:
- Have you got someone to do your shopping when you go home?
- Is your fridge/freezer stocked up?
- Will your pets be looked after? (you won’t be able to walk your dog on a lead for 12 weeks after surgery)
- Can someone help with housework and gardening?
- Can someone bring you in and take you home from hospital?
Admission
On your day of admission the ward will phone you between 11:00 and 12:00 to let you know whether there is a bed available for you. Please arrive on the ward by 3pm unless the ward staff give you a different time. When you arrive you may be asked to wait in the day room until a bed becomes available.
Medications
It is very important that you bring all your medications into hospital with you so that they can continue to be used during your admission.
Property
You will be encouraged to wear your own clothes during your hospital stay. You will need enough clothing for approximately one week. We advise that these are comfortable and loose fitting including some front fastening clothes. Healthcare staff will need to review your wounds daily so please wear clothes which allow the team easy access to your chest and any leg wounds. Storage is limited on the ward; please bring only a few personal items. The ward can provide you with towels.
Things to bring into hospital
- toiletries
- pyjamas
- slippers
- a few loose items of clothing including some front fastening
- your medications
- your decolonisation wash
- a ‘hand luggage’ sized bag – belongings will be kept in a locked store cupboard on L16 when you go for surgery
- a book
- a small amount of money to buy a newspaper, etc.
- You can bring your mobile phone or other device if you wish
- This book – ‘Your Journey Through Heart Surgery’
On the morning of your surgery you will be asked to pack up your pyjamas, toiletry bag, teeth, hearing aids, glasses and medications including the chlorhexadine wash. You will be given a bag to put these in and a member of intensive care staff will collect them.
Valuables
You are advised to leave valuables at home. A safe on the ward is available for patient’s valuables. However, sums of cash over £20.00 cannot be kept on the ward; they will have to be sent to the finance department for safe keeping.
Smoking
The Leeds Teaching Hospitals Trust has a no smoking policy throughout all hospitals, buildings and grounds. There is nowhere to smoke at the Leeds General Infirmary.
Visiting
Visitors are welcome between 12 noon – 8pm. Two visitors at a time are allowed to visit at the bed area. Children under 12 are not advised to visit (as per Leeds Teaching Hospitals Trust guidelines). If children wish to visit, please speak with the nurse in charge of the ward.
Restaurant and snack facilities are available on B and C Floors. We politely request that visitors do not bring food and drink onto the ward for their own consumption.
There are no toilet facilities on the ward for visitors. The nearest ones are situated on B Floor in the reception area.
Telephone number – Ward L16
0113 392 7416
Your relatives are welcome to ring the nursing team on the ward and the Intensive care unit for an update on your progress, but we would encourage you to nominate the same person throughout your stay and they can pass on these details to your extended family and friends where possible.
Bedside telephones are available and are provided free by Take Heart for patients to make calls. Mobile telephones may be used on silent mode by patients only.
Cancellation
Unfortunately operations may sometimes be cancelled for a variety of reasons. If your operation is cancelled we would let you know at the time the reason for this. Your operation will be rescheduled as soon as possible but you may be sent home to wait for another date.
Discharge
On the day of discharge you may be asked to vacate your bed and sit in the dayroom to allow a new patient to be admitted or someone to return from ICU. This allows other patients to have their surgery.
Intensive Care
You will go to the operating theatre on the day of your surgery. When your surgery is completed, you will be moved to the Cardiac Intensive Care Unit. Here the nursing team and doctors will monitor your recovery closely. They will also provide the care you need in the immediate post-operative period.
When we are sure that your recovery has progressed well, we will transfer you back to your cardiac ward after 12-72 hours for you to continue your recovery. If your recovery is slower than we might have expected, you will stay a bit longer until we are sure that you are ready to go to the ward.
Sedation
When you arrive in intensive care you will still be asleep. We will continue to keep you asleep (by using a short acting sedative into one of your drips) until your condition has stabilised and your body temperature following surgery has returned to normal. When you are warm and your condition is stable your nurse and doctor will make the decision to wake you up. The length of time you are asleep will be dictated by your condition. Waking will only happen when it is safe to do so.
Ventilator
While you are asleep, a ventilator is used to help you breathe. The ventilator works by pushing a mixture of air and oxygen into your lungs through a breathing tube in your mouth. As you wake you will become more aware of the tube in your mouth. It may be uncomfortable but it is important that you do not pull it out. Whilst the tube is in your mouth you won’t be able to drink or speak but your nurse will use mouth swabs and water to keep your mouth comfortable. Your nurse will use simple questions requiring a nod or head shake to communicate with you.
The nursing staff will assess when you are awake enough to remove the breathing tube and take you off the ventilator. You will then be able to breathe independantly. Your nure will encourage you to deep breathe and cough once you are breathing by yourself.
You will still need extra oxygen and will be asked to wear an oxygen mask. You will then be able to talk and start to eat and drink, but only when it is safe to do so.
Medical devices and pumps
Different devices and pumps are used to do a range of jobs in the intensive care and high
dependency unit.
Some monitor your condition; others are used for drug administration. There will be a ventilator to your left which is used to help you breathe whilst you are sedated. The machines have alarms fitted to them. When you wake up you will hear alarms sounding around the intensive care unit. The alarms are nothing to worry about. The nurse at each bedside uses them as signals providing them with information.
Drips
Cardiac surgery requires a number of drips to be put in, some in your arms and some in the side of your neck. Most of these are sited when you are asleep in the anaesthetic room. Some are used to give medications and fluids during and after surgery. Others are used to measure your blood pressure or for blood samples. Most of them will be removed before you return to the cardiac ward. They are important for your care, so it is helpful to try not to dislodge them as you move yourself around the bed. Your nurse will advise you about this.
Chest drains
Your surgeon will put two or three chest drains in during your surgery to drain away any fluid which can collect there. The drains can be uncomfortable. We will provide pain killers to minimise the discomfort. These drains are typically removed the morning after surgery, though sometimes they stay in slightly longer. Your nurse will explain what they are going to do and the part that you need to play in it when we take the drains out.
Pain
While you are still asleep, the medical team will give you pain relief. When you are awake we will ask you whether you have any pain by using a pain score of 0 to 3, 0 being no pain, 3 being severe pain. Your nurse will administer you pain relief depending on this score. This may be a tablet or sometimes the pain relief will be given through a drip. Please let the nurse know if the pain relief they are providing is enough for your needs. This is important as part of your recovery is that you feel comfortable enough to take deep breaths, cough and to be able to move yourself around the bed and sit in a chair.
Catheter
It is important for us to measure your urine output following cardiac surgery. The amount of urine your kidneys produce is an indicator of how well your heart is working. For this reason, a catheter is inserted into your bladder in the operating theatre and connected to a measuring device. The catheter will usually be removed prior to being transferred back onto the cardiac ward.
Location
Intensive Care is situated on C floor of Jubilee Wing in the Leeds General Infirmary. Ask your family to phone before visiting. The phone numbers are on the following page.
Visitors
We restrict visiting to particular times of the day. visiting times are 1pm – 3pm and 5pm – 7pm. We ask that only close family visit, and no more than two visitors at a time. This is so that we can give you the care that you need, and so you have time to rest.
Please ask the staff if you would like children under 12 to visit. It is advisable to wait until you are back on L16 for children to visit.
There is an intercom at the door to get in. The ward clerk or nurse who answers will want to know who is visiting. Your nurse or the ward clerk will come and greet your visitor prior to their first visit to ICU. They may be asked to wait a short while if you are receiving care when they arrive. Please tell your relatives to let the nurses know if it is their first visit so they can explain what has been happening so far.
Relatives are welcome to telephone at any time to ask how their family member has been. We ask, if possible, that one family member is nominated to make enquiries on behalf of your family. This allows the nurse caring for you to spend as much time looking after you as possible.
Telephone numbers – L04 Intensive Care
0113 392 7404 and 0113 392 7405
Staff
Your recovery is assisted by a large number of people. This includes nurses, nursing assistants, surgeons, anaesthetists, physiotherapists, pharmacists, radiographers, ward housekeepers, laboratory staff and others.
While you are in Intensive Care, there will always be one nurse at your bedside who will provide you with the nursing care that you need. They will also coordinate and plan the care provided by the rest of the team. As you recover you will receive high dependancy care which means your nurse will care for you and another patient. You will remain on L04 whilst this happens.
When you are well enough you will return to the surgical ward L16. You may spend a short period of time on L16’s high observation area (HOBS) or you may return to the main ward. The consultant anaesthetist on ICU/HDU will make the decision as to where you will go. You will be looked after by a nurse and the healthcare team. You may continue to have daily bloods and regular observations to monitor your progress. The nursing team will help to support your recovery and start to prepare you for your discharge home.
Physical activity after surgery
On your first day following your surgery, you can expect the nursing staff to help you to get out of bed, stand up and transfer into a chair. On your second day the nursing staff will encourage you to stand up regularly during the day and walk on the spot. The staff on ICU and L16 will help you to set daily goals to help you through your recovery.
When you are on the ward it is important for you to get up and about as much as you can. You should aim to walk the full length of the ward by the time you go home. Some people may feel able to walk further than this, for example downstairs to the shop or to the roof garden. Make sure you check with the ward staff before you leave the ward. Those who are unable to walk independently will receive assistance from the nursing and Physiotherapy staff. If required you may be seen by a physiotherapist on the ward to help you achieve your goals. Don’t worry if you don’t see the physiotherapist on the ward, this means they are happy with your progress on returning from ICU. Feel free to ask members of the team any questions you may have before you go home.
Use these daily goals to track your progress on the ward after you have stepped down from ICU
These are tasks that most people can achieve by these points in their recovery. Try to choose one or two you would like to aim for so you have a target.
What are the benefits of exercise after surgery?
- Helps your lungs re-expand and improves oxygen levels
- Improves your ability to cough and reduces the risk of chest infections
- Tones and strengthens muscles and keeps joints flexible
- Increases circulation to the heart and other major organs
- Helps to reduce cholesterol and blood pressure
- Reduces the risk of blood clots and strokes
- Improves wound healing
- Increases independence when walking
- Helps with weight loss
- Improves mood and helps you to sleep better
- You will be able to do more with less effort as your fitness improves
What sort of physical activity can I do?
Walking will have formed an important part of your hospital recovery and is the best way to progress your rehabilitation on the ward and when you go home. You can also try the exercises described later in this booklet.
How much exercise is too much?
Everybody recovers differently after surgery, but the ‘How it Feels’ Scale on the next page is a good guide. Try to exercise within the green zone.
Another good indicator is the ‘Walk-Talk Test’ to ensure that you do not overdo it. This simply means that you should be able to talk and be active at the same time.
Remember that extremely hard or maximal exertion is something you should not be asked to do in any circumstance. If you feel this is the case you must stop and take time to recover.
I feel really tired at the end of the day, is this normal?
Yes it is normal to feel tired after surgery and some tasks that you found easy before may feel difficult. It is important to pace yourself; you may find it helpful to break down an activity into more manageable chunks. This gives you more time to recover.
How long should it take to get back to normal?
There is no specific time frame, but it can take two to three months before you feel back to your normal self. The Cardiac Rehabilitation Nurses will be able to give you more individual advice once you have gone home.
Advice when having a bath or shower?
The nursing staff will assist you until you feel stronger and more confident with a wash and a shower. Try not to use very hot water because this can affect your circulation and make you feel dizzy.
It would be better to use a shower rather than a bath as it is important not to pull yourself up and out of the bath before your breast bone is fully healed. If you don’t have a shower then it would be advisable to have a wash by the sink initially until you feel stronger and your wounds have healed fully.
Surgical wounds
All patients who have had cardiac surgery will have a breast bone wound. Patients who have had a coronary artery bypass graft may have wounds on one or two legs which will initially be covered with a surgical dressing.
Many things effect the rate at which your wounds heal. These include:
- your physique
- the foods you eat
- other medical conditions such as diabetes
- your age
- smoking
When will my stitches be removed?
Different surgeons use different methods to close the skin. You may have:
- stitches (sutures)
- clips
- dissolvable stitches
- beads
You will be advised before leaving the hospital if and when these should be removed.
Some common questions asked about wound healing:
Tips for effective wound healing
- Keep your wound clean by taking regular showers. This will prevent a build up of bacteria. Do not use soap or perfumed products directly on the wounds.
- Pat your wounds dry with a clean towel after bathing/showering using a different part of the towel for your chest and leg wounds.
- Ensure you eat a well-balanced diet. Protein which is found in low fat dairy products or lean meat and pulses will help wound healing.
- Wound healing takes place during rest and sleep, so do try to ensure that you get enough rest
- Protect your wound from damage i.e. knocking the wound
- Try not to poke at the wound, as this may cause infection
- Do not use any dressings, creams, talcs etc. on the wound unless advised to do so by your doctor or nurse
- Try not to expose your wound to sunlight without protection. The wound is prone to sun burn, so keep it covered or apply a total sun block (make sure the skin is not broken before applying sun block).
How long will it take for my breast bone to heal?
Following the operation your breast bone is held together firmly by wires. These stay in place for the rest of your life. The bone is fully healed after about twelve weeks and even after the bone edges have healed, the wires will remain in place.
Normally these wires do not cause any problems, but seek advice from your G.P. if:
- you can feel the wires under the skin and they are uncomfortable
- you think infection is present because your breast bone is more painful, itchy or you have a temperature and feel generally unwell
- you think your breast bone is not fixed firmly enough together and it moves about unequally.
Aches and pains
After your operation it is normal to experience aches and pains. Everyone is different and the aches and pains you experience may be different from those experienced by someone else.
To help you become active again as quickly as possible, it is important that you take enough pain relief. We recommend that you take all pain relief medication as prescribed. If this is not adequate, please speak to your Cardiac Rehabilitation Nurse or GP.
Other effects of the operation
After your operation you may notice several changes in your senses and moods. These effects will usually resolve or improve within three to six months, if not sooner.
Medicines you may need after your surgery
Some of the common medicines that you may need to take following your surgery are listed below, but if you are taking any others, ask the doctor, pharmacist or Cardiac Rehabilitation Nurse to explain them to you.
Diuretics
How diuretics work
Diuretics are more commonly known as ‘water tablets’. They help to remove excess fluid from the body by making you pass more urine.
Cardiac surgery itself, as well as the fluids you are given during your bypass operation, can alter the distribution of fluid in your body.
You may need a diuretic for a short time following your surgery, until all the excess fluid is removed. This is usually when your weight has returned to your pre-operative weight. The time taken for this to happen varies. The diuretic may be stopped before you are discharged from hospital. If not, it will be reviewed by your GP or by your cardiac surgeon at your follow up appointment. You should continue to take your diuretic until a healthcare professional tells you it is OK to stop.
Common diuretics used after cardiac surgery:
- Furosemide
- Co-amilofruse (furosemide and amiloride)
- Bumetanide
Unwanted effects
It is normal to pass more urine whilst you are taking a diuretic. If you have been asked to take a diuretic more than once a day, make sure you take the last dose no later than the afternoon to avoid having to go to pass urine during the night.
Diuretics can sometimes cause your body to lose substances called electrolytes, especially potassium. They can also have an effect on your kidney function. For these reasons you may find that you need to have regular blood tests.
Amiodarone
How does amiodarone work?
Amiodarone is an ‘anti-arrhythmic’ medicine, which regulates the pace and rhythm of the heart beat.
Approximately one third of patients undergoing cardiac surgery may develop an irregular heart beat called atrial fibrillation. If you have never had atrial fibrillation before, you may be treated with amiodarone to regulate your heart rate.
Amiodarone is usually continued when you are discharged from hospital and will be reviewed by your cardiac surgeon in your follow up appointment at 6-8 weeks. Often it can be stopped; however, in a small number of cases it may be beneficial to continue this medicine longer term.
Unwanted effects
In rare cases, amiodarone can have effects on the lungs, thyroid and liver. You will have a chest x-ray and blood tests to check your liver and thyroid function before you start taking amiodarone and these may be repeated periodically if you keep taking amiodarone long term.
Amiodarone stays in your body and keeps working for a long time, even after stopping it. If you experience any of the following symptoms, even if you have stopped taking amiodarone, tell your doctor straight away:
- shortness of breath
- stomach pain, dark urine or yellowing of the skin or eyes
- feeling hot and active, or cold and slow
- problems with your vision.
It is important to protect your skin from sunlight, even on a bright but cloudy day, by covering up or wearing high factor sunscreen. You should also avoid using sunbeds.
Amiodarone can interact with other medicines. All the medicines you are taking in hospital will be checked by the healthcare professionals taking care of you. Please ask your nurse, doctor or pharmacist if you are unsure about any new medications you are prescribed.
You should avoid eating grapefruit whilst taking amiodarone as it can increase the level of amiodarone in your blood and cause side effects.
Anticoagulants
How do anticoagulants work?
Anticoagulants are more commonly known as ‘blood thinners’. They help to make your blood less sticky, to reduce the risk of blood clots and strokes.
If you develop an irregular heart beat which lasts for longer than 48 hours you may be asked to take an anticoagulant.
Common anticoagulants include:
- Warfarin
- Apixaban
- Dabigatran
- Edoxaban
- Rivaroxaban
Your doctor or pharmacist will discuss the different options available with you and help you decide which one is right for you.
Your anticoagulant is usually continued when you are discharged from hospital and will be reviewed by your cardiac surgeon at your 6-8 week follow-up appointment.
Antiplatelets – Aspirin, Clopidogrel, Prasugrel, Ticagrelor
How do aspirin and other antiplatelets work?
Whenever a blood vessel wall is damaged, platelets collect around the area of the damage and clump together to form a clot. If the clot becomes too large it can block the blood vessel and prevent blood from reaching the heart muscle. This is what happens when you have a heart attack. Aspirin and other antiplatelets help stop platelets sticking together, which prevents clots forming. Therefore taking asprin or other antiplatelets will help to prevent your new grafts from blocking.
When aspirin and a second antiplatelet (clopidogrel, prasugrel or ticagrelor) are prescribed together, usually the second antiplatelet is taken for no more than one year and aspirin is continued alone thereafter, in most cases for life.
If you are unable to take aspirin, your doctor may suggest that you take clopidogrel instead of aspirin. In situations like these clopidogrel is taken long term.
Unwanted effects
Aspirin, clopidogrel and, to a lesser extent, ticagrelor can cause indigestion and heartburn. To try and prevent this, you should always take them with food or just after a meal. If you do get indigestion with aspirin, you may find that the coated form of aspirin is better. If you have had a stomach or duodenal ulcer in the past, you should tell your doctor before you start taking aspirin or other antiplatelets. In some people, aspirin can bring on an asthma attack. Please tell your doctor if you suffer from asthma.
Some people may experience shortness of breath from ticagrelor which is usually a harmless side effect. If your shortness of breath gets worse or lasts a long time, discuss it with your healthcare professional who will work with you to decide if ticagrelor, your condition, or other factors are causing the breathlessness.
Please report any signs of fever, excessive bruising or bleeding to your nurse, doctor or pharmacist.
For the full information about the side effects of aspirin and other antiplatelets read the information leaflet that you get with your tablets. If you have any questions speak to your doctor, nurse, or pharmacist.
Proton pump inhibitors – Lansoprazole, Omeprazole, Esomeprazole, Rabeprazole, Pantoprazole
How do proton pump inhibitors work?
Your body produces a natural mucous barrier to protect the lining of your stomach from ‘stomach acid’. Antiplatelet medications can alter this natural barrier and make the lining of your stomach and gut more susceptible to damage. Proton pump inhibitors reduce the amount of acid produced in the stomach, which protects the lining of your stomach and gut from irritation and ulceration.
If you are taking ‘dual antiplatelets’ (aspirin plus a second antiplatelet) or a single antiplatelet with an anticoagulant, you may be prescribed a proton pump inhibitor. It is important to keep taking a proton pump inhibitor to protect your stomach for the duration of your dual antiplatelet treatment. You may be able to stop taking your proton pump inhibitor after 12 months and this should be discussed with your GP.
Proton pump inhibitors should be taken at least 30 minutes before food and other medicines.
Unwanted effects
The most common side effects are on the gastro-intestinal system and include constipation, diarrhoea, bloating, flatulence, feeling sick and tummy pain.
For the full information about the side effects of proton pump inhibitors read the information leaflet you get with your tablets. If you have any questions ask your doctor, nurse or pharmacist.
Beta-blockers – Atenolol, Bisoprolol, Metoprolol, Carvedilol
How do beta-blockers work?
Beta-blockers block the actions of hormones such as adrenaline that make the heart beat faster and stronger. They prevent the heart from beating as quickly and forcefully when you exercise or feel under stress. This reduces the work that the heart has to do.
Unwanted effects
Beta-blockers can narrow the air passages. For this reason beta-blockers may not be prescribed for some people with asthma. If you have asthma, your condition will be assessed by your cardiac surgeon or doctor before prescribing a beta blocker. They may also narrow small blood vessels which can cause cold hands and feet.
Minor side effects are common and include tiredness and cold hands and feet. Other less frequent effects include nausea, diarrhoea, skin rashes, impotence or other sexual disorders, nightmares and pins and needles in the fingers. Some of these side effects may get better when your body gets used to beta-blockers. However, if any of the side effects persist or become troublesome please discuss this with your doctor.
Beta-blockers are usually started at lower doses and the dose is gradually increased (up titrated) to the maximum tolerated or target doses.
In some cases your healthcare professional might decide to stop Beta-blockers 12 months after your operation. Beta-blockers should not be stopped suddenly. You must see your doctor if you think you need to come off your beta-blocker.
For the full information about the side effects of beta-blockers read the information leaflet that you get with your tablets. If you have any questions speak to your doctor, nurse, or pharmacist.
Cholesterol (lipid)-lowering drugs (‘statins’) – Atorvastatin, Fluvastatin, Pravastatin, Rosuvastatin, Simvastatin
How do statins work?
Cholesterol is produced in the liver with the help of an enzyme. Statins block the effect of this enzyme and reduce the production of cholesterol. Statins reduce the levels of bad cholesterol (LDL’s) and increase the levels of good cholesterol (HDL’s).
Why will I benefit from taking statins?
It is recommended that people who have coronary artery disease take lipid-lowering drugs to reduce their blood cholesterol level. Even if your cholesterol is not high, reducing it will lessen the chance of you having a heart attack.
What time of day should I take statins?
Most statins should be taken at night because most cholesterol is produced by the liver at night. However, atorvastatin and rosuvastatin can be taken at any time in the day as they are long acting.
Unwanted effects
Statins can cause stomach pain, wind, constipation or diarrhoea. If this happens to you, tell your doctor because reducing the dose may make this better. A rare but serious side effect of statins is inflammation of the muscles (myositis). You must tell your doctor if you have any unexpected muscle pain, tenderness or weakness.
Drinking grapefruit juice or eating grapefruit should be avoided if you are taking a statin drug called simvastatin. This is because it can increase the levels of simvastatin in your blood and potentially causing side effects. However, if you are taking another statin, such as atorvastatin, then grapefruit juice (or the grapefruit) can be taken in small quantities. If you have any concerns regarding statins and grapefruit then you should talk to your doctor, nurse or pharmacist.
For the full information about the side effects of statins read the information leaflet that you get with your tablets. If you have any questions speak to your doctor, nurse, or pharmacist.
What about other cholesterol-lowering drugs?
If you do not tolerate statins or they are not reducing your cholesterol sufficiently you might be offered one or more of the following drugs:
- Ezetimibe, which works by reducing the absorption of cholesterol from the intestine.
- PCSK9 inhibitors, which work by increasing the removal of bad cholesterol from the blood. These are injectable medicines that are administered twice a month and supplied by the hospital.
Please ask your doctor, nurse or pharmacist to provide more information about these medicines where needed.
What about monitoring my cholesterol?
It is recommended that after starting or altering cholesterol-lowering medications, you have your cholesterol checked after three months and then at least yearly, unless advised otherwise. You can arrange this with your GP surgery.
Ace inhibitors – Captopril, Enalapril, Lisinopril, Perindopril, Ramipril
If you are already taking an ACE inhibitor, it may be stopped before your surgery. Your cardiac surgeon will tell you if and when he/she wants you to do this. After your surgery your doctor or surgeon will decide when it is the right time to restart your ACE inhibitor. It may be restarted before you are discharged from hospital. If not, it will be reviewed by your GP or by your cardiac surgeon at your 6-8 week follow up appointment.
How do ace inhibitors work?
ACE stands for ‘angiotensin converting enzyme’. ACE is a substance in the body which makes angiotensin 2. Angiotensin 2 is a chemical normally produced in the body which makes blood vessels narrower. ACE inhibitors stop ACE from making as much angiotensin 2. This leads to the widening of the blood vessels and reduction in blood pressure, this reduces the work load on the heart muscle.
Why will I benefit from taking an ace inhibitor?
They help to reduce damage to the heart muscle which can cause heart failure.
Unwanted effects
Most people take ACE inhibitors without any problem. However some people get a persistent, dry, irritating cough. This is not serious but if you find it unbearable, speak to your doctor. He or she may prescribe an alternative treatment for you.
ACE inhibitors sometimes affect how the kidneys work and lower blood pressure. When your doctor starts the treatment, they will take care to start you on a low dose and will regularly check your blood pressure. They will check your kidneys are working well, at least once, by taking a blood test. If your blood pressure and kidneys are working well, your doctor may increase the dose.
If you cannot tolerate an ACE inhibitor your doctor may suggest that you take an alternative class of drugs called “Angiotensin II receptor antagonists” such as valsartan (Diovan®), Iosartan (Cozaar®), or candesartan (Amias®). This is a newer class of drug which is similar to ACE inhibitors and some patients tolerate them better.
For the full information about the side effects of ACE inhibitors read the information leaflet that you get with your tablets. If you have any questions speak to your doctor, nurse, or pharmacist.
GTN spray
Before your surgery you may have been using a GTN spray to relieve angina symptoms. Following your surgery, provided all of the narrowings in your coronary arteries have been treated, you are unlikely to experience angina symptoms. For this reason, in most cases GTN spray is stopped after surgery.
It is possible that some people who have had heart surgery may develop angina again in the future. If you experience chest pain or any other angina symptoms in the future, these should be assessed by your doctor. In some cases, people may need to start using a GTN spray again.
Commonly asked questions:
Nutrition
Do I need to keep to a special diet?
After your operation it is important to eat as varied a diet as possible. Eating normal amounts of a wide range of foods will help your wounds to heal. It will also help you to get your strength and energy back. If your appetite is poor, choose foods which you find tempting.
In hospital, you may find that your appetite is very poor initially. This may be because you feel sick, are in pain or are constipated. If this is the case, please tell the doctors and nurses, as they may be able to give you something to help. If you still cannot manage more than half your meals within a few days of your operation, a dietitian is available for help and advice. You may also be offered information to use when you get home.
What happens once I go home?
Try to eat meals that are of a normal size. If you cannot manage that or you find you are missing meals, try eating small snacks e.g. biscuits and cheese, a sandwich, yogurt etc. between meals.
Diet: getting the balance right
Overall dietary balance is important. No single food contains all the essential nutrients the body needs to be healthy and function efficiently. A balanced diet should include a variety of foods. The picture below represents each of the five food groups and gives a guide to the proportions of food we need to achieve a balanced diet.
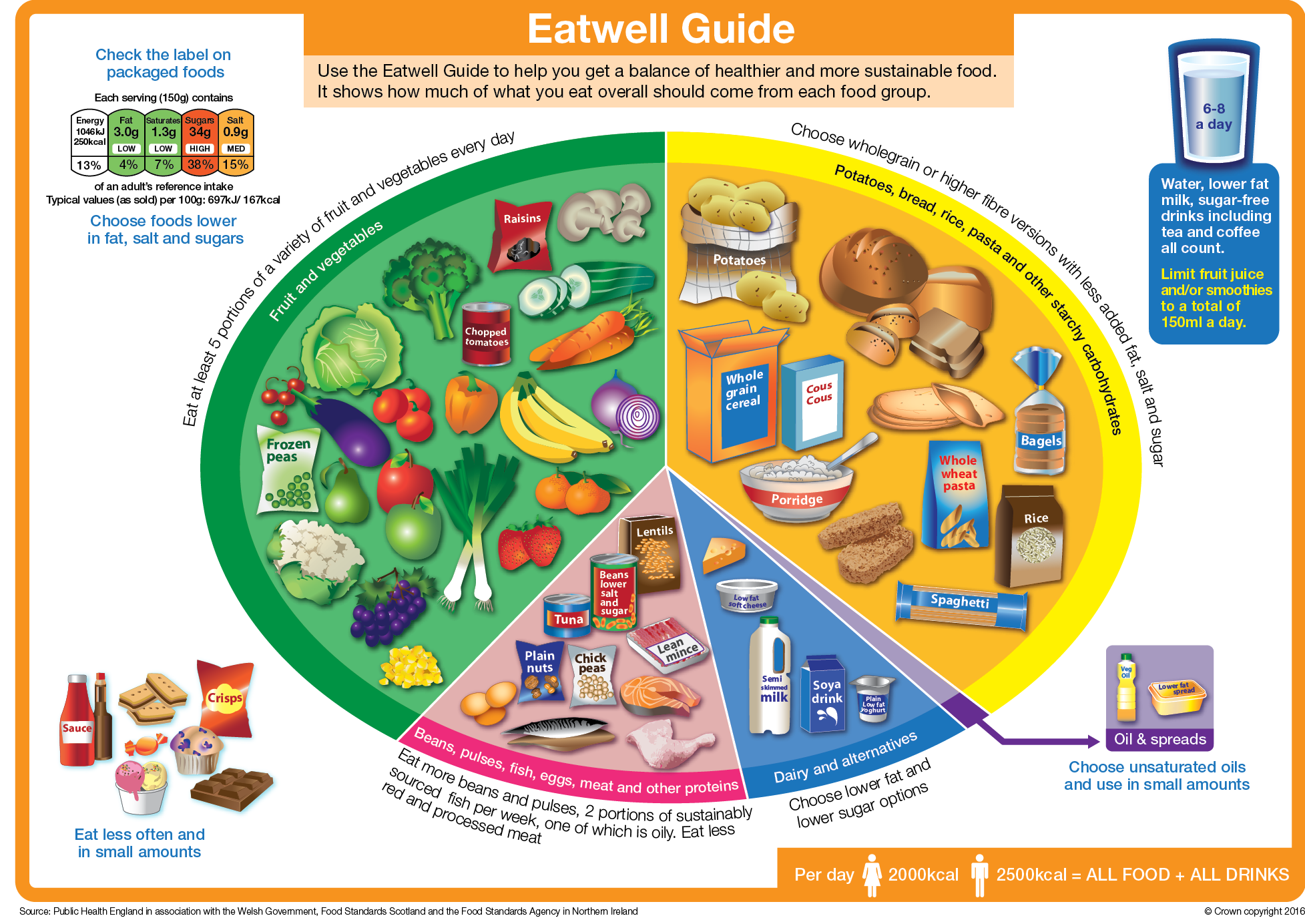
Potatoes, bread, pasta, rice and other starchy carbohydrates
Ideally these foods should make up just over a third of the food we eat. Starchy foods are bulky, low in fat and the wholegrain versions are higher in fibre, so it can be a good idea to choose brown rice, wholewheat pasta, wholemeal bread for example. Choosing wholegrain or wholemeal varieties is beneficial as they contain more fibre, vitamins and minerals. This group also includes rice, pasta and noodles
Fruit and vegetables
Aim to eat five portions of fruit and vegetables each day. Choose a variety, fish, frozen, tinned, dried and juiced all count. These foods provide us with important antioxidant vitamins and minerals such as potassium and folic acid. They are also an excellent source of soluble fibre. Fruit and vegetables are low in fat and calories, so they make the ideal snack!
Dairy and alternatives
Where possible try to choose low fat varieties. These foods provide us with a good source of protein, calcium and some fat soluble vitamins. This group includes milk, cheese, fromage frais, yoghurt, cream, butter and calcium fortified dairy alternatives.
Beans, pulses, fish, eggs, meat and other proteins
This group provides us with a good source of protein, iron, B vitamins, zinc and magnesium. Try and choose lean cuts and low fat alternatives where possible. You can include your oily fish in this group, which is an excellent source of omega 3 fatty acids. This group includes eggs, nuts, textured vegetable protein, beans, lentils and tofu.
Fish
If you eat fish, eat a variety, including oily and white (such as cod or haddock) and have 2-3 servings per week.
Oily fish are rich in omega 3 oils. These can help to make your blood less sticky, reduce the risk of blood clots and help the blood to flow around the body more easily.
If you don’t eat fish, you may need to take in omega oils in other ways, which may be nuts and seeds, but could be other ways (see cardioprotective diets).
The most common oily fish are mackerel, pilchards, sardines, kippers and salmon. These can be fresh, frozen or tinned. A portion is around 140g (4.9oz). Fresh and canned tuna do not count as oily fish.
Ideas to get you started:
- Sardines/pilchards on toast
- Tinned salmon sandwiches
- Salmon steak with potatoes and vegetables
The healthiest choices of tinned oily fish are those in tomato sauce or spring water rather than those in brine. You should aim for one portion of oily fish a week and one or more portions of another type of fish.
Nuts and seeds
Flaxseed and walnuts are another source of omega 3 oils. Try to include 4-5 servings of unsalted nuts, seeds, beans or lentils per week particularly if you do not eat fish.
Fruit and vegetables
These are an important part of keeping healthy. Aim for at least five portions a day. This should be a variety of fruits and vegetables. Fruit and vegetables contain antioxidant vitamins, minerals and fibre that can help to keep your heart healthy. It is recommended to have more vegetables than fruit.
A portion is:
- One third of an aubergine or half a pepper
- 2 x broccoli spears
- 3 tablespoons of vegetables (these can be either fresh, frozen or tinned) like carrots, peas, sweetcorn, cabbage, beans.
OR
- A small bowl of salad
OR
- 1 x apple, banana or nectarine
- 1 x handful of grapes, strawberries or cherries
- 1 x slice pineapple, pawpaw, mango or melon
- 2 x plums, satsumas or kiwis
- 3 x dried apricots, prunes or figs
- 5-6 x passion fruits or lychees
- 1 small glass of fruit juice (150mls) – this only counts once a day!
Fresh, frozen, tinned and dried fruit all count towards your 5 a day. (Potatoes are starchy and therefore do not count towards 5 a day).
Five easy ways to 5 a day
Breakfast:
- One glass of fresh fruit juice/vegetable juice
- One bowl of cereal with dried fruit
Lunch:
- Salad in a sandwich
- Add salad or vegetables to a hot meal
- Piece of fruit as dessert
Evening meal:
- Serve two types of vegetables with your main meal
- Tinned fruit in fruit juice and low fat yoghurt
- Stewed fruit
Snacks:
- Try raw vegetable sticks like celery, carrots and cherry tomatoes, fresh fruit or dried fruit.
Cardioprotective diets
Cardioprotective diets generally follow the Eatwell Guide principles and are linked with a healthier heart. One example would be a Mediterranean style of eating. This is one well known whole dietary approach that may suit you.
Be mindful that other dietary approaches may work better for you, but the most important thing is to think of your diet as a whole. Continue with any cardiac beneficial, whole dietary approaches that suit you.
Fat
A cardio protective style of eating is not necessarily low in fat, but the type of fat is important. There are two groups of fats: saturated and unsaturated. Healthy fats are better than very low fat. The cardio protective diet is more beneficial than a very low fat diet in prevention of CVD. If you need to reduce your weight, then you need to eat less fat of any kind and this should be a small proportion of your overall diet. Replacing saturated with unsaturated fat is better than replacing it with carbohydrates or protein.
The following information is taken from British Heart Foundation website: www.bhf.org.uk
Unsaturated Fat
Unsaturated fats in small amounts are thought to be better for us as they help to lower your LDL (bad chol; total cholesterol and helps to lower your LDL (‘bad’ cholesterol).
There are two types: Monounsaturated and Polyunsaturated.
Examples of foods
Monounsaturated Fat:
Avocados, olives, olive oil, rapeseed oil. Almonds, cashews, hazelnuts, peanuts, pistachios, spreads made from these nuts.
Polyunsaturated Fat:
Oily fish, corn oil, sesame oil, soya oil, and spreads made from those oils. Flaxseed, pine nuts, sesame seeds, sunflower seeds, and walnuts.
Saturated Fat
Saturated fats usually come from animal products These fats tend to be solid at room temperature. Although we need a small amount of these fats in our diet, larger amounts can be harmful because they can raise your LDL or ‘bad’ cholesterol, so try to reduce the amount you eat. They need to be a very small percentages (less than 10%) of your diet. Try to reduce the amount you eat or substitute with polyunsaturated fats.
Examples of foods
Processed meats like sausages, ham, burgers. Fatty meat. Hard cheeses including cheddar. Whole milk and cream, butter, lard, dripping, ghee, suet, palm oil and coconut oil, pies, cakes, biscuits, pastries, fried foods.
Trans Fat
Trans fats are thought to behave in a similar way to saturated fats and are therefore harmful when taken in excess quantities. Try to avoid these when possible.
Examples of foods
May be in some fried foods, takeaways, processed snacks like biscuits, cakes or pastries. Hard margarines
Ideas to help
- Use a monounsaturated spread instead of butter. Try olive oil based spreads, e.g. Utterly Butterly, St Ivel Gold, Bertolli or other olive oil type spreads
- Oven bake or grill instead of frying
- If frying then try to use olive, rapeseed or linseed oil instead
- Buy leaner cuts of meats and remove the visible fat from meat before cooking
- Skim excess fat off stews and casseroles
- Remove skin from chicken and turkey
- Choose low fat dairy products such as low fat cheese and low fat milk.
Salt
Most of us consume more salt than we need. High salt intakes can contribute to high blood pressure and fluid retention. Gradually reduce the amount of salt you add to foods – in cooking and at the table to allow you to adapt to the change in taste. Use other means of seasoning such as pepper, herbs, spices and lemon juice to flavour foods. Pre-prepared foods, sauces and soups can contain lots of salt – check the labels and try lower salt varieties, or prepare foods yourself without adding salt if possible.
Foods high in sugars
These foods should be eaten in small quantities. They provide excess calories and can contribute to weight gain. It is important to limit the amount of ‘free sugars’ in the diet. Too much free sugar can raise your triglycerides (fatty chemicals in the blood). Free sugar includes sugar added to food and drinks (either at home or during manufacturing) and sugar naturally found in foods like honey, agave syrup or fruit juice. Adults can have up to 30g of ‘free sugars’ a day. The sugar found naturally in whole fruits and vegetable is not free sugar and does not need to be included in this amount. There is advice on how to cut down on sugar on the NHS live well website. This group includes biscuits, cakes, ice cream, sweets, chocolate and fizzy or sweetened drinks.
How do I understand food labels?
Nutrition labels can help you choose between products and keep a check on the amount of foods you are eating that are high in fat, saturated fat, sugar and salt.
Packaging often shows foods in ‘traffic light’ colours, so that you can see at a glance if they are high (red), medium (amber) or low (green) in fats, sugar or salt. For a healthier choice, try to choose products that have more greens and ambers than reds.
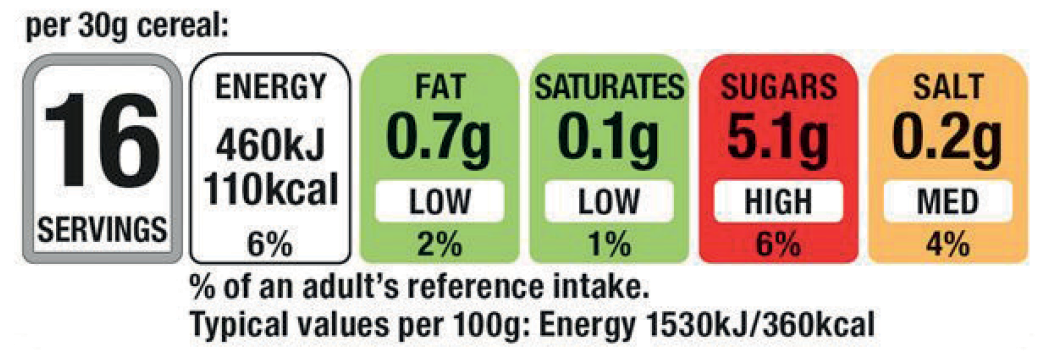
If you have a smart phone you can download the food4life food scanner App. You can scan product bar codes to check levels of sugar, saturated fat, salt and calorie content of the item. This will allow you to make an informed choice about your purchase (or product at home).
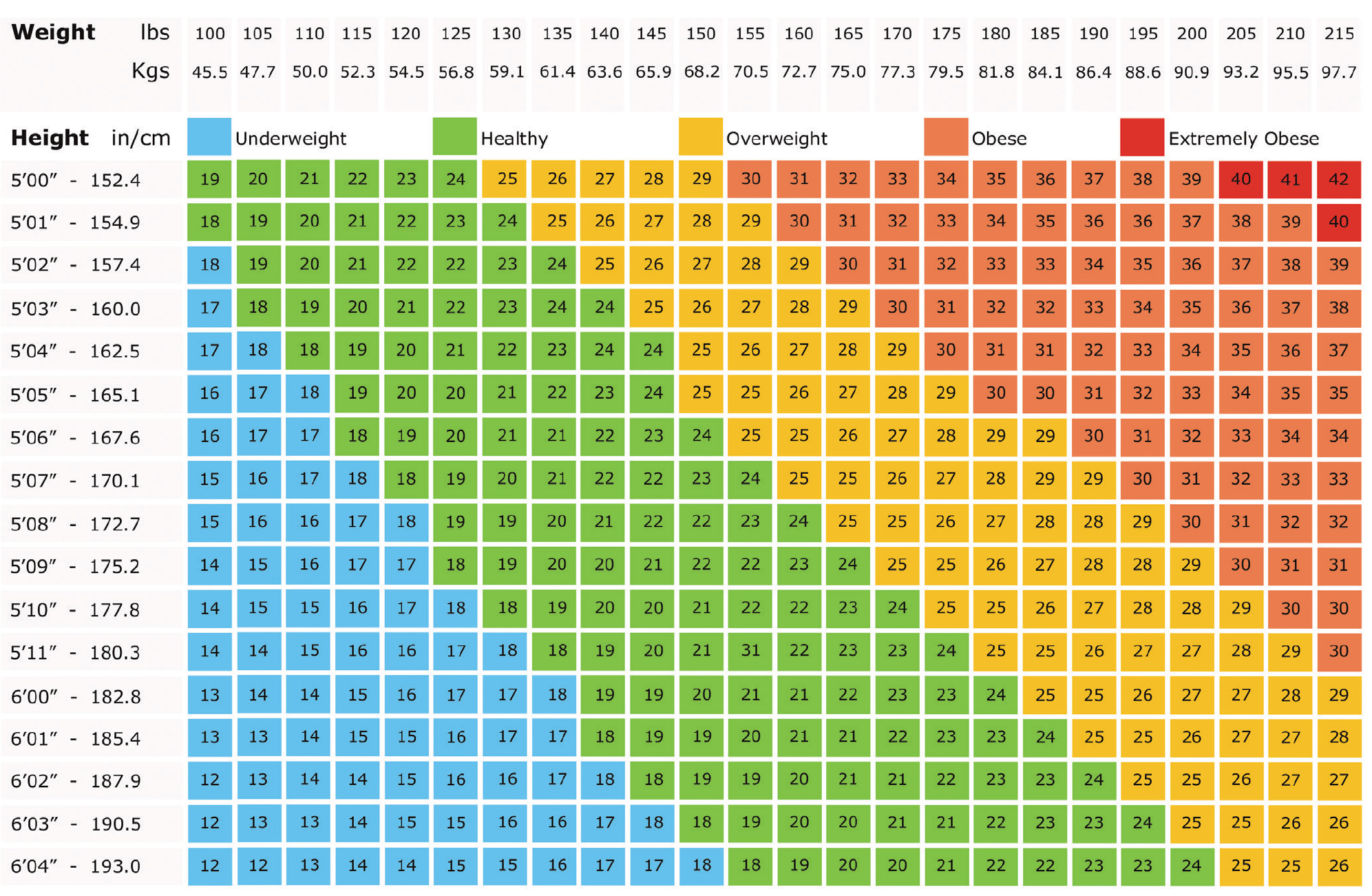
Being overweight
If you are overweight, then aiming to reduce your weight by 10% is beneficial. For example, if you are 18 stone, aim for 16 stone or if you are 14 stone aim for 13 stone. This will reduce the strain on your heart and will help lower your blood pressure. If you follow the dietary advice to reduce fat intake, your weight should come down.
Waist size is an indicator for heart disease risk. 37 inches for a man and 31.5 inches for a woman is the top end of waist measurement that is considered healthy (BNF). Look at the following chart to see where your weight falls.
You can reduce your energy intake by changing the snacks you eat (e.g. crisps, cakes, biscuits) to the fruits and vegetables suggested. Do not forget that all alcoholic drinks contain calories.
Be careful when choosing low fat foods as some can still be high in calories due to the amount of sugar in the food, e.g. fruit juices, reduced-calorie biscuits and low fat yoghurts. You may notice that you tend to eat more when you are feeling worried, low in mood or bored. If this happens to you, try and find an activity or hobby that will take your mind off food or have a glass of water or no added sugar squash instead. Keeping a diary of what you eat and drink can also help you to find ways in which you can reduce the amount of energy you eat. The support of your friends and family is also important to help you to keep motivated.
Weight and height chart
Alcohol
Can I still drink alcohol?
Drinking more than the recommended amount of alcohol can have a harmful effect on your heart and general health. It can cause abnormal heart rhythms, high blood pressure, damage to your heart muscle and other diseases such as stroke, liver problems and some cancers.
Alcohol is also high in calories so it can lead to weight gain (see drinkaware.co.uk to check calorific value of alcoholic drinks). It also lowers your inhibitions which might mean you find it harder to stick to your healthy eating plans when you have been drinking. If you are trying to lose weight, cut down on alcohol.
If you drink alcohol it is important to keep within the guidelines:
- Men and women should not regularly drink more than 14 units a week
- Spread your drinking over three days or more if you drink as much as 14 units a week.
These guidelines apply whether you drink every day, once a week or only occasionally.
One unit of alcohol is equivalent to:
- One single measure of spirits
- One single measure of apertifs
- One small glass of sherry
- One small glass of wine
- Half pint of ordinary strength beer, lager or cider
Most people don’t drink alcohol every day – but if you do, try having some days off – aim for at least two alcohol free days a week. Just make sure you don’t increase the amount you drink on the other days.
Drinking large amounts of alcohol in one go, particularly on a regular basis, can cause damage to your heart muscle so avoid heavy or ‘binge’ drinking.
Your GP can help to support you in reducing your alcohol consumption if you decide you would like to do this. If you are a dependent drinker, please seek medical advice before you stop drinking suddenly. You can find more information at www.drinkaware.co.uk
Check the strength of what you are drinking, as this will affect the units, particularly if you are drinking stronger ales or lagers.
Consider the measures you pour when you are drinking at home, as these tend to be more generous than standard pub measures.
If you require further information or support with reducing your alcohol intake, please seek advice from your cardiac nurse or GP.
What to expect after your discharge from hospital
- If you are not contacted by the community cardiac rehabilitation nurses within seven working days of being discharged from hospital or if you have any concerns once home, please make contact with the numbers you have been provided with by the hospital team for your area.
- If you need help for minor accidents or unexpected health problems outside these working hours or over bank holidays, please call 111 (for urgent medical help that’s not an emergency).
- If you feel very unwell or are experiencing chest pains which are not resolving please do not hesitate to call 999 and get emergency help.
Discharge from hospital
When you are discharged home from hospital, we recommend that you have some food shopping organised and some plans in place to help you with your heavier tasks in the household and garden.
Physical activity on discharge from hospital
This section will provide advice for you and your partner or carer about the importance of physical activity. It will also give guidance about how much activity and what type is recommended during the first few weeks at home after discharge from hospital.
What are the benefits of physical activity?
Being physically active:
- Reduces the risk of stroke, coronary heart disease, diabetes, osteoporosis and some cancers
- Improves the circulation to the heart and the other major organs
- Helps keep blood pressure within normal limits (lowers raised blood pressure)
- Helps improve your blood cholesterol levels
- Tones and strengthens muscles and keeps joints flexible
- Helps to prolong independence as we get older
- Enables us to do more with less effort as fitness improves
- Helps us to maintain or to reach a healthy weight
- Helps in the prevention and management of depression and anxiety
- Improves psychological well-being (increases self-esteem)
- Helps to prevent blood clotting
- Helps us to sleep better and gives us more energy
- Helps us to relax.
What sort of physical activity can I do?
Walking will have formed an important part of your hospital recovery and needs to continue as part of your rehabilitation when you return home. Your first walk at home should be a similar distance to that walked in hospital. It is important to gradually increase the time spent walking and then the speed.
How much should I do?
In the first six weeks of your recovery, you should be aiming to increase your walking to 30 minutes continuously. We recommend you use the ‘Walk-Talk Test’ to ensure that you do not over do it. This simply means that you should be able to talk and be active at the same time. Everyone has a different level of fitness and it is important that you exercise at your own pace.
You could try making a list of all the physical activity you do in your day, gradually working your way up to 30 minutes and increasing it by a little more each day.
Everyday activity
This section is designed to help you return to everyday life after you come home from hospital. It is a guide only and you must remember that everybody recovers at different rates and has different levels of fitness. As with everything, you should start gently and build up gradually.
How much you feel able to, or want to do will depend on your usual daily routine. You may find it useful to break down a task into more manageable chunks – giving yourself more time to rest. If you experience pain or discomfort, stop doing the task.
Individual advice and guidance on work and leisure activities can be sought from the cardiac rehabilitation team. If you have been seen by the physiotherapist whilst in hospital you should have been shown the following exercises. These are examples that you could try at home instead of going for a walk. Remember to start off slowly, gradually increasing your pace.
Aim to begin with 30 seconds for exercises 1 to 4, and five ‘sit to stands’ (exercise 5). If you feel able, aim to do these twice a day.
When you can manage the exercises comfortably, gradually increase the time, e.g. from 30 to 40 seconds and five to seven sits to stands.
1. Walk on the spot
Swing your arms, step your feet.

2. Toe Taps
Alternate stepping forwards, tapping your left and right toes.

3. Step ups
Hold onto a rail for support. Step up onto the step. Step back down. Repeat. Try holding on to the back of the chair or to the wall if you need a little more support with exercises 1-3.

4. Shoulder circling
Put your hands on your shoulders. Circle both arms forwards and then backwards.

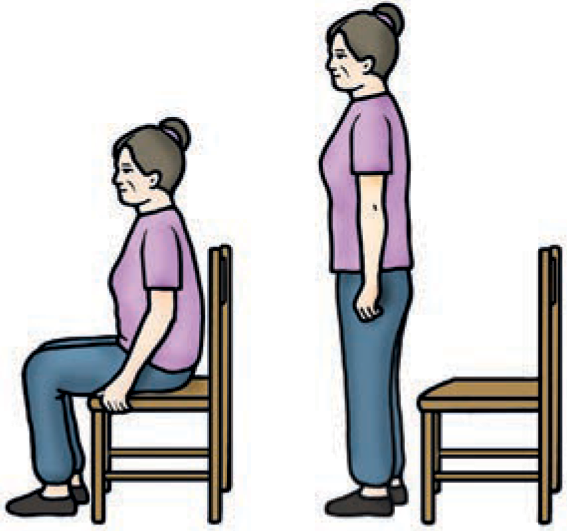
5. Sit to stand
Sitting on a dining/kitchen chair. Feet on the floor, shoulder width apart. Stand up then sit down slowly. Repeat.
Exercises too boring?
- Try walking on the spot whilst watching TV or making a phone call
- Put some of your favourite music on, or listen to the radio whilst carrying them out
- Try a step counter so you can see how much you are doing
- If the weather’s bad, could you take a trip to an indoor shopping centre to do some walking?
The following provides some general guidelines for you
For the first few days at home, keep to the same routine as in hospital. Get dressed, potter around the house, climb stairs slowly and rest when you need to. For the first six weeks do not lift anything heavier than a half full kettle (with approximately half a litre of water in).
Avoid
- Carrying shopping, lifting, pushing, pulling heavier objects, heavier housework, cleaning and gardening for the first twelve weeks
- Walking the dog on a lead for the first twelve weeks
- This is to allow time for the wound and sternum to heal.
Friends and relatives may wish to visit at this time, which may be enjoyable but also very tiring. Ask them to stay for short periods and limit the number of visitors.
Follow these stages, starting at stage one and when you feel ready move onto the next stage.
At around six weeks after discharge you will have a starting date for a cardiac rehabilitation exercise and health education programme. Your community cardiac rehabilitation nurse will discuss this with you.
Physical activity diary
You may find it useful to record your activities on a diary sheet. This will also be useful for the cardiac rehabilitation staff when you attend the exercise and education programme. An example of a physical activity diary is available in the PDF version of this information, or in the printed copy that your healthcare team should have given you.
For your safety please avoid the following:
- Exercising during periods of illness, if you feel unwell, or have a temperature
- Drinking alcohol and being physically active
- Engaging in physical activities for at least an hour after eating
- Having a very hot or a very cold bath or shower after activities
- Being active in extremes of temperature, (e.g. in very cold weather, wrap up warmly and walk at a slower pace. This is because the heart has to work harder in these conditions)
- Sudden excessive physical activity.
Remember it is important to:
- Always warm up and cool down
- Wear comfortable clothing and footwear with low heels
- Reduce intensity of any physical activity following illness or a break
- Gradually build up your activity levels
- Increase your fluid intake on hot days
- Make physical activity part of your daily routine
- Find a long term physical activity you enjoy
- Mention any concerns you have about sexual activities to your cardiac nurse or doctor.
During physical activity it is normal to:
- Feel yourself breathing harder than normal
- Feel warmer during and after the exercise
- Feel your heart beating slightly faster.
You should still be able to talk whilst exercising and feel that you could keep going at this level for some time. The key is to exercise without over exertion.
- If you feel well and pain-free following your exercises, do not be tempted to continue as prolonged exercising will not speed up your recovery
- Do not exercise (or continue to exercise) if you are experiencing any of the following: chest, arm or jaw pain, nausea, excessive breathlessness, palpitations, excessive sweating, muscle cramps, feeling faint or dizzy
- Should you experience difficulties with any aspects of the home exercise programme do not hesitate to contact your cardiac rehabilitation team as alternative exercise programmes and physical activities can be discussed.
If you were not very active before your hospital stay or you suffer from a condition which restricts your level of activity, e.g. arthritis, you may need to progress at a slower pace.
What is the cardiac rehabilitation exercise and health education programme?
Programmes are run in community leisure centres with your cardiac rehabilitation nurse. You can attend from about six weeks onwards after discharge from hospital. You will usually have an outpatient appointment with your Consultant prior to starting the programme.
The programme involves a supervised exercise session twice a week for six weeks depending on the programme. The exercise sessions take about an hour, followed by a talk and a chance to ask any questions. You will spend approximately two and a half hours at the programme each time.
The talks may include
- How the heart works
- Healthy eating
- Physical activity
- Managing stress
- Medication
You will be invited for an introductory visit to meet the cardiac rehabilitation staff and for the Physiotherapist/exercise professional to design an individual exercise programme for you.
When can I return to my sports and hobbies?
Everyone is different and therefore has different recovery rates, so please ask your doctor or a member of the cardiac rehabilitation team. Participating in the exercise and health education programmes will also give you the opportunity to seek advice from the team about this issue.
Hobbies
Remember as with any activity, start gently and build up gradually. If you experience any pain or discomfort whilst exercising or have any questions, consult your cardiac rehabilitation nurse.
Walking
You may start walking as soon as you get home from hospital. Start by walking indoors and distances that you could manage in hospital. Gradually increase the distance and progress to outdoors, as you feel comfortable.
Gardening
After a month you can start light gardening, such as weeding, but avoid prolonged bending. No digging or heavy work until you have full wound and sternum healing at about 12 weeks.
Swimming
You may return to swimming after 12 weeks providing there are no wound and/or sternum healing problems. Swimming is a good all round exercise, especially for those who are overweight or have joint problems.
Cycling
This is a good exercise for increasing leg strength and overall stamina. After 12 weeks you may start cycling on paths and quiet roads, progressing as you feel confident. If you have an exercise bike you may start this after eight weeks.
Fishing
Use shorter, lighter rods if possible to begin with. If you intend to row a boat then you must wait at least 12 weeks.
Golf
Start with putting and progress to pitching, no driving until 12 weeks – to allow for full bone healing. Begin with 9 holes and progress to 18, as you feel comfortable.
Do not attempt rugby or any contact sports without discussing this with your Consultant or seeking advice from your Cardiac Rehabilitation Nurse.
Exercise is for life!
Any extra physical activity you can add into your life above 30 minutes a day can significantly benefit your health.
Why not try..?
- Walking to work
- Parking your car further away from the shops
- Getting off the bus one or two stops earlier
- Using the stairs instead of the lift or escalators
- Using the television remote control less
If you alter your lifestyle in this way and then exercise regularly, you will notice how much more you can do with less effort. You will enjoy all the benefits of exercise and may meet new people.
It is very important whilst choosing an exercise to find one you enjoy, so you are more likely to continue with it.
The exercise and health education programme will be able to encourage and help you with your future exercise levels, so until then try including more activity into your daily routine.
Breathlessness
Is it common to become breathless when walking or doing tasks?
It is quite normal to breathe a bit harder than normal when you are physically active. If you get breathless when physically active, pacing your activities or resting usually helps. Sometimes people find they get very worried about breathing a bit harder than usual. This worry can lead to the body becoming tenser which may make relaxed breathing more difficult. Recognising when breathing harder is normal and learning how to relax can both be of help if you think this applies to you.
How do I know when I should ask for help?
Everyone gets a bit breathless at times if they have to do something they’re not used to and find it a bit of a challenge. However, if you find that you are experiencing any of the following, please seek help:
- The breathlessness comes on suddenly
- Is different from normal
- Does not go with rest
- Comes on when you are not active
- Or, if you find that you are gradually getting more breathless over a few days.
Questions about sex
Following discharge from hospital you are advised to gradually increase your daily exercise as you gain strength and confidence, pacing yourself as you feel most comfortable. This applies to all your daily activities including sexual intercourse. You can have sex as soon as you feel ready.
Many people have concerns about having sex after heart surgery. Some commonly asked questions are:
Your emotional recovery
Many people find waiting to come into hospital for heart surgery stressful. You might feel relieved that the operation is over. Or, you may be reading this having come into hospital suddenly because you became unwell and needed the surgery quickly. Not having much time to prepare yourself can be a challenge as you start to recover.
People sometimes think that stress and worries can lead to a person having heart problems. However, there is little scientific evidence to support this. It is true that people who are under high levels of stress are likely to smoke or drink more, both of which add to risk. The stress itself is not thought to be problematic.
The following are a few questions that other people who have had heart surgery have asked and which you might find helpful as you recover.
Pacing yourself
As part of your recovery it is important to get back to doing things that you enjoyed before. The rate at which different people are able to do this will vary, and you should follow the advice of your cardiac rehabilitation nurse, doctor, physiotherapist or fitness instructor, as to how much you should be doing and how soon you should be doing it.
For some people, the worry caused by having heart problems stops them from activities they previously enjoyed, even after they have been told that they can do them. If you find yourself doing this, here is some advice you might find useful.
- Set yourself a target. For example, some people want to get back to doing the gardening or jobs around the house. Break the target down into smaller chunks. For example, you may decide that weeding a whole flowerbed would be too much. Think about how much you might be able to do without becoming tired. If this is five minutes of dead- heading flowers, have a go. Be prepared to stop if it gets too much. Set yourself a target and increase as able, and breaking down into smaller tasks. If you found it easy, think about doing a bit more next time, e.g. 10 minutes. However, make sure you do not do more that you had planned to do one day as rushing into things can make you feel more tired.
- Do activities with other people, you may be worried about going out alone straight away. Try going somewhere nearby with someone else the first time. When you feel okay about doing this, go some of the way on your own and then gradually do more to build up your confidence.
How about the future?
For some people, recovering from a heart operation can be the start of some positive changes. Many people become a lot fitter and may decide to take up new activities such as swimming or walking, which they had not thought of before. Others realise the importance that some things – and some people – have to them and are determined to make time for themselves to do things they enjoy. Worrying will not bring on heart problems, but people often realise that they would like to be less stressed and do something about it. Many people get a real sense of achievement from doing something positive to feel healthier.
How can the cardiac rehabilitation team help me?
After your surgery, it is important that you feel supported in getting back your confidence. There may be a lot of information to remember when you first come out of hospital. Your Cardiac Rehabilitation Nurse can help you with any questions you may have about your recovery.If you have been invited to attend an exercise and health education programme, you will receive further suppport and advice from the members of the team as well as meeting other people who are also recovering and making positive changes to their lifestyles.
Driving, holidays and work
When can I drive again?
There are regulations about driving which are issued by the driving vehicle licence authority (DVLA). They generally depend on what type of operation you have had, so if you are not sure, find out and write the name of the operation. These regulations are:
Coronary artery bypass grafting and valve repair or replacement.
- You do not need to tell the DVLA about your operation, but you do need to let your insurance company know.
- The DVLA advise that you do not drive for four weeks following your surgery. However, the surgeons here at the Leeds General Infirmary strongly advise that you wait for at least six weeks. This is to ensure that the breast bone can take all the tugging from the steering wheel etc. without worsening any chest discomfort. You may also experience a lack of concentration for some time after your surgery, which could be dangerous when driving.
Remember these are only guidelines – some people feel that they are not up to the stresses and concentration necessary for driving in today’s traffic until much later than this six week period, whilst other people do not have any problems. It is up to you to make sure that you are safe to drive again, in whatever conditions you might meet.
N.B. You are still required to wear a seat belt.
Pacemaker operation
You must inform the DVLA of your operation. They will want to make enquiries about your health with your G.P. This is to ensure that regular checks can be made to ensure that your health does not affect your ability to drive.
These regulations apply to ordinary drivers licences only. If you hold a HGV or PSV licence, you must inform the DVLA immediately and your licence will be temporarily withdrawn. You will be able to re-apply for your licence, so please ask your doctor or cardiac rehabilitation nurse for further advice.
Car insurance
As mentioned before, it is very important that you let your insurance company know about your operation or you may find that your policy is not valid. In most cases you should state that you have had a ‘corrective procedure’. This means that the operation has “corrected” your condition.
Some people find that their insurance companies accept this, whilst other companies ask for a medical certificate before they will agree to give you insurance cover and other companies will load your policy by up to 20%.
The attitude of motor insurance companies really does vary so if you have problems ask your cardiac rehabilitation nurse, who may be able to offer some advice. If in doubt, shop around for your car insurance.
Can I go on holiday on a plane?
You should not travel abroad until after you have attended your six week outpatient appointment. We recommend that before you make plans to travel abroad, you discuss it with your cardiac rehabilitation nurse.
Remember the flight on the aeroplane is often the least physical part of your journey. The hassle of finding a parking place, queuing at the check-in desk and waiting around can be very tiring, so it’s worth bearing these things in mind before you book your holiday.
Holiday insurance can sometimes be a problem and some airline companies may ask for a medical certificate to say that you are medically fit to fly.
N.B. most travel insurance policies ask you to declare any medical condition that you have been treated for in the past 12 months, so if in doubt ask before you travel.
When can I go back to work?
This very much depends on the job that you do. The best plan would be to discuss this with the surgeon either before you are discharged or at your outpatient appointment. Your cardiac rehabilitation nurse may also be able to advise you. If your job is a desk job you may feel able to return to work after 8-12 weeks. However, if you have a more physical job you may have to wait longer. The ward team can provide you with a sick note.
Cardiac rehabilitation nurses
You should have been given the contact number of your Community Cardiac Rehabilitation Team either before your surgery or prior to your discharge home.
The community cardiac rehabilitation nurses are a team of specialist nurses with broad nursing experience and specialist skills. They will contact you by telephone within a week of discharge from hospital. During this phone call they will arrange an appointment for you within the next few weeks. If you have not heard from them after a week, please contact them – see next page for contact numbers. They will follow-up with you with visits in clinic and over the telephone.
The community cardiac specialist team work closely with the cardiac rehabilitation team at the Leeds General Infirmary, your GP and other services, as well as your family, carers and friends to maintain and improve your quality of life. The team can advise on:
- medication issues
- the safest way to resume physical activity, offer reassurance, advice and support to help you make positive lifestyle changes
- the exercise and education programme and on-going support.
Community cardiac rehabilitation teams contact numbers
Airedale Cardiac Rehabilitation Team
Bradford Cardiac Rehabilitation Team
Bradford Hospital Trust
Bradford community based Cardiac Rehabilitation Nurse
Bradford city
Bradford community based Cardiac Rehabilitation Nurse
Bradford south and west
Calderdale Cardiac Rehabilitation Team
Harrogate Cardiac Rehabilitation Team
Huddersfield Cardiac Rehabilitation Team
Areas included: Cleckheaton, Batley, Liversidge, Mirfield, Heckmondwike, Huddersfield
Leeds Community Cardiac Team
Mid Yorks Cardiac Rehabilitation Service
Normanton office
Mid Yorks Cardiac Rehabilitation Service
Dewsbury office
Pontefract/Wakefield Cardiac Rehabilitation Team
York Cardiac Rehabilitation Team
Glossary of terms
Further contacts
Health advice
Other Advice
Alcohol/drug misuse
Anxiety & Depression
Bereavement
Carers
Disability
Driving
General Health Information
Exercise
Older People
PALS
Voluntary services/networks in Leeds
If you’re looking for support/assistance on discharge there is a vast amount available. You can get assistance with practical tasks such as shopping and gardening, assistance with checking benefits and completing the forms, social groups and drop-in centres to name a few.
These services are available through three main networks that can be accessed by telephone or on-line. They are:-

Registered Charity No. 1002063
Raising funds exclusively for the Yorkshire Heart Centre at Leeds General Infirmary, St James’s Hospital and its units within the Leeds Teaching Hospitals NHS Trust.