Welcome to the St James’s University Hospital Renal (Kidney) Transplant Unit, Leeds. Kidney transplantation has been carried out in Leeds since 1962 and over 5000 kidney transplant operations have taken place.
The purpose of this booklet is to help you understand about kidney transplantation including why we perform kidney transplants, the assessment process and where kidneys come from. If you are accepted for a kidney transplant then we will offer you information about the operation, recovery and life after a transplant.
Why consider a transplant?
Kidney transplantation offers you the chance of regaining a much improved quality of life with many benefits:
- Freedom from dialysis.
- More energy and freedom to socialise and enjoy life with your family and friends.
- Removal of some dietary and fluid restrictions.
- Improved strength and energy.
- Improved fertility.
- On average, a longer life expectancy.
However, these benefits are not guaranteed and there are some risks associated with the operation. These include:
- Risk of a deceased donor kidney transplant failing – approximately 3 in 50 in the first year.
- Risk of a living donor kidney transplant failing – approximately 1 in 50 in the first year.
- Risk of not surviving the transplant operation – approximately 1 in 100.
Risks associated with the immunosuppressive drugs include:
- Increased risk of infections, especially in the first year.
- Small increased risk of cancer after transplantation in particular skin cancer, lymphoma (blood cancer) and cervical cancer in women.
- Small increases in the rates of diabetes, high blood pressure and high cholesterol.
- Other side effects specific to the drugs used such as headaches, vivid dreams and tremors which are usually short term.
Why do transplants make you feel better?
As long as the transplanted kidney works well then it is able to take over all the important body functions that your original kidneys did. These include:
- Continuous removal of waste products.
- Continuous removal of excess fluid.
- Production of the natural hormone erythropoietin (EPO) which reverses anaemia.
- Restores the bone turnover of calcium to normal levels.
- Excretion of drugs.
- Control of blood pressure by removal of salt.
It is important to realise that kidney transplantation is not a cure for kidney failure but it is a treatment which can offer excellent benefits to your health.
Can I have a transplant?
Each patient is assessed individually to see whether transplantation is the best option for them.
Approximately one third of patients who undergo dialysis are eligible for transplantation.
Age itself is not a reason for exclusion and a number of other factors may contribute to the decision not to proceed with registering you for a transplant.
These include:
- Being significantly overweight- this could make the operation risk unacceptably high.
- Severe heart disease.
- Severe lung disease.
- Poor circulation of the blood or a blood vessel disease.
- Severe liver disease.
- Recent or active cancer.
- Previous major surgery.
- Poor compliance with current medical treatment.
Most importantly, if you do not want to be considered for a kidney transplant then let your doctor or the renal transplant co-ordinator know and you will not be assessed.
Will my original kidney disease come back?
This will depend on the original disease.
The following diseases may occur again in your new kidney after transplantation:
- Diabetes.
- Glomerulonephritis- IgA disease, Membranous nephropathy, Focal segmental glomerulosclerosis (FSGS).
- Haemolytic uraemic syndrome (HUS).
- Lupus.
- Oxalosis.
- Vasculitis.
Even though these diseases can reoccur after transplant, it is unusual for them to cause loss of the transplant. Recurrent disease is actually an uncommon reason for kidney transplants to fail.
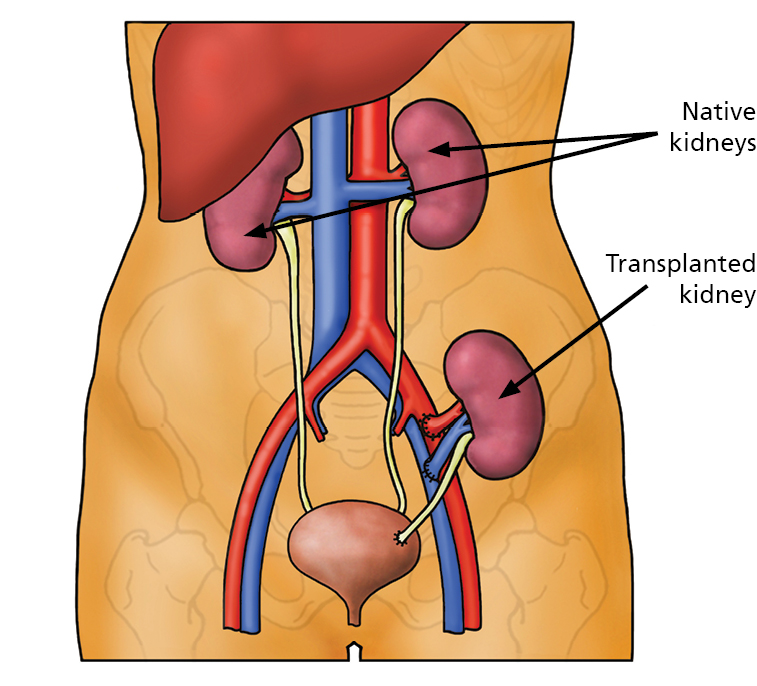
Back to topDo native (your own) kidneys need to be removed?
In the vast majority of cases the answer is no. The transplanted kidney is usually placed in the groin and not in the place where your own kidneys are. This is due to technical considerations (ease of access, limiting trauma of surgery) and means that the original kidneys will not be removed (see illustration below).
Occasionally the native kidneys are removed for a number of possible reasons:
- Very large kidneys (e.g. large polycystic kidneys).
- Kidneys with long-standing infection.
- Appearance suspicious of cancer.
When can I be considered for a transplant?
There are no hard and fast rules for the point at which you can be considered for kidney transplantation but we attempt to assess patients before they start dialysis.
Some transplants are actually performed prior to starting dialysis (pre-emptive transplant).
In general:
- You should discuss transplantation with your doctor in the low clearance clinic even before you talk about dialysis options.
- Serious consideration should be given to any possible living donors. This is something to discuss with your family or close friends. This is generally the most likely way of receiving a pre-emptive transplant and the best option for most people as living donor kidneys generally function for longer than those from deceased donors.
It may be that you are already established on dialysis and you can discuss transplantation with a doctor in dialysis review clinic.
Being assessed for a kidney transplant
Once you have discussed transplantation with your doctor then the assessment process will begin.
This process is organised by the Renal Recipient Transplant Co-ordinators. It involves:
- Checking that you are medically fit to undergo major surgery.
- Checking that your bladder and the blood vessels in your pelvis will support a kidney transplant.
- Ensuring the necessary blood tests for tissue typing and virology screening have been performed (these can take a number of weeks to process).
- Providing you with all the appropriate information for you to make an informed decision about choosing whether to undergo a transplant.
- Recording your consent for blood to be retained in the laboratory.
- Ensuring you have discussed the risks and benefits of surgery in order to be consented for a transplant.
Once your tests are complete your case will be presented to the surgical and medical team and a decision will be made about your suitability as a potential transplant candidate.
If transplantation is considered to be in your best interests, the transplant co-ordinators will arrange an appointment with you. This is to ensure that you are fully informed about undergoing a kidney transplant.
Following this your name will be added to the National Renal Transplant Register and you will receive written confirmation of this.
What if I don’t get onto the transplant register?
It is extremely important to realise that less than half of all patients who have kidney failure will be eligible for a transplant. This is because often they will be found to be medically unfit. This information will be explained to you either by telephone or in clinic. Please inform the Transplant Co-ordinators if you have a preferred method.
In short, if you are not accepted onto the transplant register it is because going through the operation or taking the required immunosuppression medication is considered too risky for you. If you are unhappy with the decision you should raise it for discussion with your dialysis or clinic doctor.
Back to topPancreas and kidney transplant
If you have Type I diabetes you may want to consider a simultaneous pancreas and kidney (SPK) transplant. This is a slightly more complex operation that involves the transplantation of both a kidney and a pancreas from the same deceased donor. However, it offers the chance of treating the underlying diabetes so that insulin injections are no longer required.
These operations are not performed in Leeds, our nearest transplant centres are Manchester and Newcastle. You will need further assessment tests for a SPK transplant as the risks are higher than that of a kidney alone transplant however when successful it is more beneficial to you. Some people may not be deemed fit enough for a SPK transplant but may still be considered for a kidney alone transplant.
What assessment investigations are required to be considered for a kidney transplant?
You will be asked questions about your medical history as well as your general fitness in order for us to make sure that we arrange the appropriate investigations for you.
Heart and Lungs Assessment
It is important to know the condition of your heart and lungs to ensure you are fit to undergo major surgery.
Potential investigations include:
- ECG (Electrocardiogram).
- Some patients may require a chest X-ray particularly if they have ever smoked or have breathing problems.
- Some patients may require a more detailed heart scan (Myoview or stress echo) performed in the Nuclear Cardiology department. The test involves an injection of a small amount of radioactive material which is taken up by the heart and shows if the heart is receiving an adequate blood supply.
- Some patients may require a CPEX (Cardiopulmonary exercise test). This is a non-invasive exercise test to assess the health of the heart and lungs.
- Some patients may require an echo (echocardiogram). This is a heart scan which includes an assessment of the valves in the heart.
The renal team may ask a cardiologist, chest physician or anaesthetist to review your results, the outcome of which may be that you need to be assessed in person.
Blood vessel and Surgical Assessment:
- One of the doctors may assess the pulses in your groin and legs to evaluate your blood flow. It is important to ensure your blood vessels are able to support a kidney transplant and provide an adequate blood supply.
- Some patients require a MRI or CT scan of the blood vessels in their pelvic area. This often involves a dye being injected into your blood in order for the surgeons to have a map of your blood vessels to ensure there is somewhere for a transplant kidney to be placed.
- Some patients need to see the transplant surgeons before the operation to discuss technical issues. Some common causes for this include:
- You may have large kidneys (e.g. polycystic kidneys) that need to be assessed before transplantation to ensure there is enough space for the transplant kidney.
- You have bladder or kidney drainage problems which need assessment.
- You are significantly overweight and need to discuss the extra risk in such circumstances.
- You have had one or more previous kidney transplants – to ensure it is technically possible to carry out another transplant.
- You have a reduced exercise tolerance (can not walk very far) or have an increased frailty score.
You may also be referred to the urology team if it is felt that your bladder requires further assessment.
Screening for TB:
This is a blood test called Quantiferon to ensure that people who require TB preventative medication after a transplant receive it.
We carry this blood test out once, unless you travel to a high risk area for TB whilst you are waiting for a transplant, in which case it needs to be repeated.
We will not perform this blood test if you have previously had TB and successfully completed treatment, as it will not provide us with any additional information. After a transplant we will assess whether or not it is in your best interests to take some TB preventative medication for a period.
You will be contacted if the is positive result. The TB specialists would then aim to review you in clinic and assess whether you have an active or inactive form of TB infection. If it is inactive then you would be prescribed preventative TB medication to take for a time period. Once you are established on this medication it would not delay you being activated on the transplant register providing everything else was in place.
If you are found to have an active TB infection then you will need to be investigated and fully treated for this before we can place your name on the transplant register.
Body mass index (BMI) Assessment
Your BMI is calculated from your height and weight as part of your assessment process. If you wish to know your current BMI the dialysis staff, outpatient department or transplant co-ordinator can tell you this.
It is unlikely that you will be accepted for a transplant if your BMI is above 35. Ideally, in order to reduce your risks during and recovering from the operation your BMI will be below 30.
If you wish to seek assistance as to how you can reduce your BMI please ask to speak to one of our dieticians or the transplant team.
Dental Assessment
The mouth and teeth are often a source of infection. We strongly advise that you complete a dental check-up prior to being registered for a kidney transplant.
If your dentist recommends any dental work to be done it should be completed before you are registered as active on the transplant register. If you have difficulty registering with a dentist please contact the transplant co-ordinators who may be able to refer you to the local dental hospital.
Cancer Screening
Before your name is placed on the renal transplant register you must be up to date with any routine cancer screening.
This is because the immunosuppression medication will increase the spread of any pre-existing cancer.
Back to topYou should have received a leaflet ‘Spotting cancer early’, please take some time to read this and ensure your screening is up to date, such as cervical smear tests, bowel screening and mammograms. We will also write to your GP to request their assistance with this.
What if I have had cancer?
Previous cancer is not necessarily a problem that will stop you from being assessed for a transplant.
In general, the previous cancer will need to be under complete control (in remission) with no further cancerous cells present.
The immunosuppressant drugs that are used after transplantation will reduce the body’s own defence against cancer. This means that a previous tumour may be more likely to come back.
It is therefore sensible to wait a certain amount of time after successful treatment before deciding to consider transplantation. The amount of time usually varies and can be over five years but depends on the type of cancer you had previously and how invasive it was.
Psychologist or Social Worker Assessment
You may be asked to meet with a Psychologist or Social Worker before your transplant to determine if you have any emotional concerns or life situations – such as housing, family or financial difficulties – that could stand in the way of caring for yourself or others after your transplant.
If there are problems, the Psychologist or Social Worker can work with you to help find solutions.
The importance of compliance
A kidney transplant is a very precious resource for which demand far outweighs supply. We like to think of it as a precious gift either from the living donor or the family of a deceased donor. For this reason we are obliged to make sure it goes to someone who will look after it.
Your transplant registration may be delayed if we have concerns regarding your:
- Compliance with dietary restriction (consistently high phosphate and potassium levels).
- Fluid gain between dialysis sessions.
- Compliance with taking medications.
- Previously failed transplant due to not taking medication.
- Dialysis or outpatient attendance.
Vaccinations
After a kidney transplant, due to the anti-rejection medication you are more at risk from infections. We therefore recommend that you are up to date with all vaccinations offered to you before you join the transplant register. This includes Flu, COVID and Shingles.
Where will your new kidney come from?
There are three sources of donor kidneys:
- Living Donors.
- Deceased donors following brain stem death (DBD).
- Deceased donors following circulatory death (DCD).
Are all donor kidneys similar in quality?
The donor kidneys are of variable quality. Ideally, all donor kidneys would be from young, living donors without any other disease.
However, this is simply not possible. Generally speaking, the following factors make donor kidneys better quality:
- Living donor.
- Younger donor.
- Donor without high blood pressure or diabetes.
- Short transfer time between donor and recipient.
- Good tissue match.
Despite these factors, any kidney is likely to provide a significant benefit from dialysis but on average, kidneys from living donors are more likely to work straight away and work for a longer period of time. Deceased donors who have a history of diabetes, high blood pressure and smoke are not excluded as kidney donors based on these grounds.
These aspects of the donor’s history would not necessarily be discussed with you at the time of transplant.
Types of transplant
Living donors
Nationally, each year there are increasing numbers of patients undergoing a living kidney transplant.
Transplantation from a living donor is not a new idea. The very first live donor transplant was performed between identical twins in 1954 in Boston, USA. Here in Leeds, living donation has increased steadily from 17 transplants in 2000 to currently approximately 50 a year. Nationally, there has been a steady increase in live donation from 101 in 1990 to over a thousand a year.
Live donor transplantation is a unique procedure where a healthy individual undergoes surgery for no clinical benefit to themselves.
All parties involved must consider all the positives and negatives involved. Each case must be carefully assessed to ensure a low level of risk to the donor and a high benefit to the recipient.
Advantages of living donation
For the recipient the benefits of a live donor transplant may include:
- Reduced waiting time on the transplant database than for a deceased donor transplant as the live donor assessment normally takes up to 6 months.
- The procedure can be planned on a set date (electively) and therefore you can make arrangements beforehand.
- Improved quality of the donated kidney as it spends less time outside of the body.
- Receiving a transplant before your health deteriorates.
There are often considerable benefits to everyone in the family if one member receives a transplant from another.
This is due to a marked improvement in the recipient’s energy and activity levels as well as possibly returning to work and normal leisure activities.
Disadvantages of living kidney donation
As with deceased donation, there is is no guarantee that the transplant will work for a particular length of time or indeed, at all. It is important that the donor understands the following risks:
- Risk of death associated with the operation is very small, approximately 1 in 3500.
- Risk of moderate to severe complications, e.g. a deep vein thrombosis, collapsed lung or injury to the bowel, less than 1 in 50.
- Risk of minor complications, such as chest infection, urine infection or wound infection.
- Small risk of bleeding after the operation, with the potential for needing further surgery.
- In the long term, most live donors will develop protein in the urine, although this has no detrimental effect on general health.
- Live donors are at a slightly increased risk of developing high blood pressure in the future (1 in 4 people) which is an increase from 1 in 5 people in the general population.
However, it is important to state that there is good scientific evidence that:
- Individuals who lose a kidney for other reasons (not living transplant donors) generally enjoy a normal lifespan without later kidney problems.
- Long term follow up of living kidney donors reveals a normal lifespan.
Who can donate?
Anyone can come forward as a potential living donor for you. Possible donors can include:
- Brothers and sisters.
- Mothers and fathers.
- Grandparents, uncles and aunts.
- Cousins.
- Husbands, wives and partners (unrelated).
- Friends (unrelated).
It is important that any donor is in good general health, with a healthy weight and have a BMI below 30 and is aged over 18 years.
It is becoming increasingly common for people to use social media to appeal for potential living donors. If this is something that you are considering please speak to the living donor team beforehand as they will be able to support you to do this in a constructive way.
Kidney Sharing Scheme
If you have a potential live donor who is not a blood group or tissue match to you then they can still complete the assessment tests. If they are accepted as a living donor then you can be placed in the National Kidney Sharing Scheme. Every 3 months NHS Blood & Transplant service (NHSBT) would then identify whether there is a pair in the same situation in the country who you could exchange kidneys with. This means that your living donor donates a kidney and you receive a living donor transplant later that day but it is not your donor’s kidney.
This scheme has generated a significant number of living donor transplants that would not otherwise be able to take place.
You can discuss this option with your doctor or ask any potential living donors to contact the live donor co-ordinators on: 0113 206 6601 for more information.
Receiving a live donor transplant
Once all the necessary assessment tests are completed for both the donor and recipient, we will aim to schedule surgery for a time that is convenient to you, your donor and the transplant team.
Altruistic Donors
This is where a living person volunteers to donate a kidney to an unknown recipient, that is, someone they have never met before and is unknown to them. These kidneys are allocated nationally in a similar way to the deceased donor kidneys, but the transplant is carried out on a known date.
You will receive a telephone call explaining the situation if an altruistic kidney is found to be compatible for you.
Deceased Donors
Transplant patients who do not have a suitable living donor will receive their kidney from a deceased donor – someone who has died. The donor or their families have consented to donate their kidneys and perhaps other organs and tissues for transplantation. There are two types of deceased donors:
- Donation after brain stem death (DBD) – donors who have suffered fatal brain injury and have been certified as brain stem dead. The heart and blood circulation continue to work right up until the kidneys are retrieved.
- Donation after circulatory death (DCD) – donors who have suffered severe injury or illness but are not certified as brain stem dead. Treatment is withdrawn and the patient dies (heart and breathing stop) before the organ retrieval. The surgery is therefore carried out in the absence of a beating heart.
If you are offered a deceased donor transplant the donor could be either a DCD or DBD donor. That is because you will be contacted for whichever transplant is available first for you. If you receive a kidney from a DBD donor the chance of delayed graft function (sleeping kidney) is 1 in 4 compared to 1 in 2 from a DCD donor.
This means you may need dialysis in this period of time but reassuringly the kidney success rate whether it is from a DBD or a DCD, is that 94 out of every 100 transplants performed are working after 1 year.
Waiting for a deceased donor transplant
All patients waiting for a deceased donor kidney transplant are placed on the national transplant database which is co-ordinated from the headquarters of NHSBT in Bristol.
Kidneys are allocated through a computer system that ensures each organ goes to the best possible recipient.
Factors in selecting a recipient include:
- Tissue matching- blood type, tissue type, antibodies.
- How long the patient has been waiting or has been on dialysis.
- The age difference between the donor and potential recipient.
The number of people waiting for a donor organ is far greater than the number of organs that become available.
You could be called in for a transplant at any time following your activation on the register but the average wait time in the UK is currently about 2 to 3 years.
Finding the right kidney for you, whether it comes from a living donor or a deceased donor, requires matching.
There are important levels of matching:
- Blood group.
- Tissue typing (HLA testing).
- HLA antibodies.
How are the kidneys allocated?
Clearly the distribution of precious kidneys is a highly emotive issue and for this reason it is essential to ensure a transparent and fair system. The organ allocation system in the UK is run by NHSBT. This is an independent but government funded organisation charged with the job of ensuring fair distribution of all transplant organs. They also try to increase organ donation rates.
Clinical staff from all around the country (as well as patient groups) contribute to the running of the organisation.
When a family gives consent for the donation of organs from a relative who will be a deceased donor, the intensive care unit contact NHSBT to register the organs to be potentially donated. The donor is then tissue typed (HLA) and these details are analysed.
The better matched the kidney is to you then the less likely that rejection will occur. Additionally, the better matched the kidney the lower the chance of antibodies being formed, which may affect your waiting time should you require another transplant in the future.
The principle of having a national matching system is to ensure that the majority of kidneys go to the best matched person. Once the HLA type has been received by NHSBT the process of matching can begin.
As well as the HLA type being matched, the blood group also has to be compatible.
The process of matching also considers the following:
- The patients age.
- Time spent on the waiting list. Priority is given to those patients who have either been on dialysis or on the transplant database for longer, particularly if it has been over 7 years.
- “Sensitised” patients (priority is given to patients who have multiple antibodies and therefore are very limited in which kidneys they can receive).
The matching system is constantly monitored to ensure fairness. The longer that you are on the list the more chance you have of receiving a kidney.
Blood group
For all transplants, the first critical factor is matching blood groups. If the blood groups are not compatible, the organ will certainly be rejected immediately, apart from in the live donor setting where a successful treatment may be planned prior to transplant.
The permitted combination are:
| Recipient’s blood type | Required blood type of potential donor |
| O (48% of the population) | O |
| A (38% of the population) | O or A |
| B (10% of the population) | O or B |
| AB (4% of the population) | O or A or B or AB |
It is worth noting that blood group B is much more common in the Asian community. The relative lack of blood group B donors is one of the reasons that on average, Asian recipients wait longer for a deceased donor transplant.
Back to topTissue typing (HLA Typing)
You inherit your HLA (Human Leucocyte Antigen) type from your parents. HLAs are found on the surface of most cells in the body. If your HLA is different to the donor’s, your body’s immune system may recognise the difference and attack the kidney, causing it damage.
The better the HLA match between you and the donor, the better the chances of the transplant being successful in the long term.
However, while a perfect match is best, it is not always essential and many transplants work well despite some differences in the HLA types.
There are many different tissue types and so most people are different from each other. The best chances of finding a good match are among your close family members, especially brothers and sisters. However, it is also possible to find a good match with donors who are not related to you. We must find your HLA type to help choose a suitable donor for your transplant. We will do this by testing a sample of your DNA, which we get from your blood cells. The laboratory will store a sample of your DNA in case we need to carry out more tests in the future.
We will give the results of your HLA typing to the team that will perform your transplant. We will also send this information to NHS Blood and Transplant Organ Donation and Transplantation (NHSBT ODT) as part of the information they need to help find a suitable donor for you. We may send copies to the other healthcare staff who are treating you (for example, your dialysis unit), so they have your results in their files. We can also send these results to any other hospitals you may transfer to in the future.
HLA antibodies
HLA antibodies also known as cytotoxic antibodies, can be made by your immune system. These antibodies may attack the donor HLAs and cause damage to the kidney. You may have HLA antibodies if you have:
- Previously had a transplant that failed.
- Had blood transfusions.
- Been pregnant.
HLA antibodies can appear, disappear and reappear over time and so it is important to test for these regularly. If you are waiting for a transplant, you must be tested for HLA antibodies at least once every three months.
Your blood will be sent to the H&I laboratory to carry out these tests at the relevant times normally by your dialysis unit or low clearance clinic.
The laboratory will use the results to help decide which differences in you and your donor’s HLA types can be allowed and which cannot.
The laboratory will then send the results to NHSBT ODT to help make sure you are only offered a kidney from a suitable donor.
The laboratory will keep all these samples to carry out crossmatch tests in the future.
Crossmatching
The crossmatch test is a direct test between the antibodies in your blood and the white blood cells from a potential donor. This is the ultimate test of whether you have any antibodies that could cause a transplant to fail.
If you have been offered an organ from a deceased donor (a donor who has died), we may need to carry out this test immediately before the transplant is expected to take place, to decide whether you match the donor.
The crossmatch test will use some of your stored blood samples, but the transplant team may also call you in to provide a fresh sample. This is a test of whether you have any antibodies in your blood that could attack the transplanted organ and cause it to fail. We often call it “doing a transplant in a test tube”. A transplant cannot usually take place unless the result of this test shows that none of these antibodies are in the patient’s blood at the time of transplant.
If a living donor is being considered, you will probably have more than one crossmatch test to make sure the donor is suitable. These tests will usually take place over a number of months, as it can be a long time between the first test and the transplant. The final crossmatch test will be shortly before the transplant is due to take place. Until the transplant team know the results of the final crossmatch test, they cannot make a decision about whether or not the donor is suitable, and whether the transplant can go ahead.
A compatible match means there is no reaction and it is safe to proceed with the transplant. If there is a reaction, the test is called an incompatible match and the transplant cannot proceed. We will give the crossmatch results to a member of the transplant team as soon as we have them.
Once you have had your transplant, the laboratory will store all your samples, and the donor’s samples, in case they need them for tests to help with your treatment in the future.
What happens to my sample?
When we no longer need your samples for testing, or we have more samples then we need, the law allows us to use these anonymously for quality control (making sure our tests are working correctly), research (depending on whether this is approved by ethics committee) or introducing new procedures, or for educating and training doctors, nurses, scientists and other professionals working in healthcare.
This helps us maintain accurate testing procedures and improve our knowledge, and so provide the best possible care for all patients.
However, if you do not want us to use your samples for any of the purposes above, please tell a Transplant Co-ordinator. We will respect your wishes and dispose of any samples we no longer need.
Data Storage
All data obtained by the laboratory is held and used in compliance with the Data Protection Act 2018.
Why do you need my permission?
We need permission for scientists to test, and store, your blood sample.
If you do not give your permission, we cannot carry out tests or keep your sample.
Locally allocated kidneys
Most kidneys are allocated nationally. However sometimes kidneys are allocated in Leeds. In this situation we take into account the:
- Blood group compatibility.
- HLA match.
- Age difference between donor and recipient.
- Length of time each recipient has waited for a transplant.
Fast-track kidneys
To ensure as many kidneys as possible are transplanted nationally, there is an offering sequence known as the ‘fast track’ system. This is when kidneys are offered simultaneously to all transplant centres in the UK if the originally allocated or local centres are unable to transplant the kidney.
You are entitled to ask if you are receiving a ‘fast track’ kidney, and if so, why other centres have declined to use the kidney for transplantation.
Receiving a deceased donor transplant
Once you are placed on the renal transplant database, you must be contactable at all times as you will be required to attend St James’s University Hospital at short notice in the event of a potential transplant offer.
Only in extremely rare circumstances are two people called into hospital for the same kidney transplant, therefore, if you are called into hospital for a transplant we highly anticipate that this will go ahead.
Should you have any further questions please contact the transplant co-ordinators, otherwise we will be in contact with you following completion of your assessment.
Back to topUseful websites
NHSBTThe Blood and Transplant section of the NHS. NHSBT staff promote and facilitate deceased and living organ donation and organise the offering of kidneys to transplant. The annual data from all transplant centres in the UK is published on their website.
www.organdonation.nhs.uk British Kidney Patient AssociationThe KPA is run by people living with kidney disease for people living with kidney disease to offer informal peer support.
Kidney BeamThis is a free to access online programme for people living with kidney disease containing exercise sessions, education and wellbeing support.
Kidney Care UKA charity to support people living with kidney disease. Resources include information resources, financial grants, counselling, dietary advice and an online community.
National Kidney FederationA charity run by kidney patients, for kidney patients. Resources include information resources, a helpline, peer support service and financial advice.
Contact us
By post
Renal Transplant Co-ordinators, Level 2, Lincoln Wing,
St. James’s University Hospital, Leeds, LS9 7TF
Online
Renal Transplant Co-ordinators Living Donor Transplant Co-ordinatorsBy telephone
Renal Recipient Transplant Co-ordinators
Mon – Fri, 08:00 – 17:00
Living Donor Transplant Co-ordinators
Mon – Fri, 08:00 – 17:00