Welcome
This booklet has been designed to give you information regarding the assessment process for liver transplant. Please ask any member of the team if you have any further questions.
Section 1 – General Introduction
Introduction
Liver transplant is a well recognised treatment option for chronic liver disease (cirrhosis), liver failure and other rare conditions that affect the liver. The aim of liver transplant is to enable you to live a near normal life.
Liver transplantation will not benefit everyone and it is necessary to undergo an assessment process first. This not only ensures that other treatment options have been considered and there is a good chance of increasing your life expectancy after transplant.
This booklet is designed to help you understand the various stages of the assessment process.
Explanation of terms used in this book
Transplantation: The replacement of your liver by a liver taken from another person.
Donor: The person from whom the liver is taken. The donor is usually someone who has died and who has expressed a wish to donate their liver after death.
At St James’s Hospital we also have a live donor programme which means that a family member or friend could consider donating part of their liver.
Recipient: The person who receives the new liver.
The normal role of the liver
Your liver is the largest solid organ in the body. It is found on the right hand side, just below the ribs.
It performs many essential functions to keep the rest of the body working correctly. For example:
- It produces bile and delivers this via fine tubes called bile ducts into the bowel, to help digestion and absorption of vitamins and fats.
- It controls the amount and type of food circulating in your bloodstream.
- It converts damaging substances you eat or which your body makes, into harmless products which can easily be removed from your body.
- It makes clotting factors to stop you bleeding and various other proteins, some of which help you to fight infections.
- It controls the level of several hormones in your blood.
- It metabolises (processes) many drugs.
- It makes most of the proteins that your body needs.
- It stores many important vitamins.
- It helps regulate body temperature.
- It helps provide a defence against infection.
When the liver fails to work properly
There are many different diseases that affect the working of the liver. Some of them cause gradual deterioration and take many years before they affect the liver severely enough that liver transplantation needs to be considered. These are chronic liver diseases known as cirrhosis.
Others destroy the liver in a very short period of time, often in people who have had no known liver disease beforehand. These are much less common and are called acute liver diseases.
People who suffer from any sort of liver disease can have some of the problems listed below:
- Jaundice (when the skin and eyes go yellow). This can be associated with itching, dark urine and pale stools.
- Increasing tiredness, feeling unwell, feeling cold.
- Loss of muscle strength and weight loss.
- Increasing amount of fluid in the body, causing a swollen abdomen (ascites) and swollen legs.
- Vomiting of blood from thin walled veins (varices) which develop in the gullet (oesophagus) and the stomach.
- Slowing of mental functions, confusion, excessive sleepiness or coma. This is called encephalopathy.
Reasons why a liver transplant may be considered
If you have been assessed as being suitable for liver transplantation this is usually because:
- You have liver failure and there is no alternative to increase your life expectancy and quality of life or,
- You have liver cancer and liver transplantation offers you the best chance of a cure or,
- You have some uncommon symptoms of your liver disease which affect your quality of life to such an extent that the benefits of liver transplantation outweigh the risks.
In addition, your current health is thought to be good enough to mean that you have a better than average chance of being alive five years after liver transplantation (more than 50%).
Section 2 – The Assessment
The assessment process
The assessment will usually be as an outpatient. This will have been discussed with you by a Transplant Co-ordinator before the planned dates and you will be asked to attend an out patient clinic.
It is important that you understand this is for an assessment and does not commit either you or us to a liver transplant.
The assessment team
Whilst you are undergoing your assessment you will be seen by a Consultant Hepatologist (liver specialist), Transplant Surgeon, Anaesthetist, Liver Transplant Coordinator, Social Worker, Dietitian and a Substance Misuse Nurse Specialist. A description of each role is provided below:
- Consultant Hepatologist: a liver specialist with expertise in transplant who will assess your need for liver transplant.
- Transplant Surgeon: a liver surgeon who will review the technical aspects of the operation in your case, provide a risk assessment which will include the types of liver you will be suitable to receive and the doctor who will perform the operation.
- Anaesthetist: the specialist responsible for helping to assess your fitness for general anaesthesia and liver transplant.
- Liver Transplant Coordinator: a specialist nurse with expertise in liver transplant. The coordinator organises the logistics around your assessment and the operation and will provide you with advice and support both before and after your transplant.
- Dietitian: the dietitian will provide a global assessment of your nutritional status and will advise you on any specialist diets that we wish you to follow both prior to, and if listed for liver transplant.
- The Health and Wellbeing Team: this team consists of a social worker, a specialist mental health worker and a substance misuse nurse. They can support you in issues related to your overall well-being and may discuss your home, family circumstances and care needs. They can also offer help in arranging support for other family members if you provide a caring role. They can also signpost you towards resources for financial support.
Blood tests
An extensive panel of blood tests are taken at the time of your assessment to review your liver function as well as your kidney function and other aspects of your health. These blood tests will also give us information on previous viruses your body has been exposed to and will check your blood group.
Scans of your liver
A decision will be made as to which scan will be performed as part of your assessment. This will either be a CT scan or an MRI scan.
The scans are performed to look at your anatomy (in particular the blood vessels supplying blood to, and taking blood away from your liver) and to exclude a liver cancer.
They will also review the other organs in your abdomen.
Tests on your heart and lungs
- Chest X ray – this is an Xray picture which looks at your lungs.
- Lung Function Tests – these measure the condition of your lungs. This helps the anaesthetist to judge whether there may be any breathing problems during or after the operation.
- Electrocardiogram (ECG) – a test of the electrical activity of the heart.
- Echocardiogram – this is a form of ultrasound of the heart to check the heart muscle pump function.
- Cardiopulmonary exercise test (CPEX) – this is an exercise test which shows your fitness level. Usually performed on a static bicycle but can be done on a treadmill.
Additional tests
Sometimes extra tests are needed, these are most often recommended to assess your heart function in more detail. Further information on the specific tests will be provided if you do need to have them done.
Other considerations
- The no alcohol agreement
For some people, alcohol is thought to have been a major contributor to their liver disease. If the team decides an alcohol agreement is necessary as a condition of being accepted for transplantation you will be asked to sign this and abide by its terms.
Some people will also be asked to see an alcohol counsellor as a condition of being accepted onto the programme.
Please note
If you sign this agreement you are making a life-long pledge to yourself, the transplant team and your donor that you will not drink alcohol again ever.
You are also showing that you understand that transplantation will not be a treatment option for you if you drink alcohol again.
Smoking
Smoking increases the risk of short term complications after surgery, such as hepatic artery thrombosis (HAT), Deep Vein Thrombosis (DVT) and wound healing problems. Smoking increases your risk of cancer in general after transplantation.
Stopping smoking may be a condition for you being listed for liver transplant. If you currently smoke you should try to stop smoking as soon as possible.
Drug use
You cannot be considered for liver transplant if you use illicit (otherwise known as illegal or recreational) drugs.
The Liver Transplant Meeting (also known as MDT)
Your case will need to be presented to the full transplant team before a decision is made. These meetings are usually held weekly and provide a wider team discussion about your care.
There may be several different outcomes of the meeting. Not all patients are suitable for transplant for many different reasons. The decision to offer you a position on the waiting list may be deferred while either you have further investigations to assess your suitability for transplant, or there may be a recommendation from the team assessing you to improve your strength and fitness prior to going on the transplant waiting list. Sometimes a recommendation will be made for you to undertake further work with the substance misuse team.
Occasionally we cannot offer you a place on the waiting list and if this is the case, you will be informed of why we have come to this decision. You will be contacted after these meetings, usually by a Transplant Coordinator.
Going on the list
You will have a pre-listing consultation with a Transplant co-ordinator and a listing discussion with a transplant Co-ordinators after watching the ‘educational film on liver transplant.
If everyone is in agreement you will be called by a transplant co-ordinator to confirm you are active on the transplant waiting list.
Types of Liver donor
When the transplant team discuss your case at the transplant MDT they will decide which types of donor liver you may be considered for. You may be considered suitable for livers from Donation after Brain Death (DBD), Donation after Circulatory Death (DCD) or Living Donors. You may also be considered suitable for a split liver transplant. The recommendations are made by reviewing several factors including: your fitness; anatomy and past surgical history and the cause of your liver disease.
Donation after brain death (DBD)
This is a donor who has been declared dead by brain stem death testing. This type of donor has a continuous blood supply to the liver during the retrieval surgery.
Donation after circulatory death (DCD)
For these livers, a decision will have been made that the donor will not survive their illness. Any supportive treatment will be withdrawn and the donors heart has to stop. This process has to occur within a set time frame for the organ to be suitable to be considered for donation. After withdrawal of supportive treatment, the blood supply to the liver will be decreased.
This means that in DCD organs, we can see a delay in liver function after transplant and occasionally biliary problems in the recipient. This type of transplant can often be cancelled due to the donation not proceeding in the strict timings required.
Split livers
Surgeons have looked at how to maximise the number of transplants we can perform. Some livers can be split meaning that either two small adults or an adult and a child can receive a part of the same liver.
In these cases the liver grows to fit the recipient. There are certain complications associated to split livers but these can be managed.
Living donation
From April 2007 liver transplant units in England have been able to offer transplantation involving living donation. The Leeds Liver Unit is one of the biggest centres for live donation. Advantages of LDLT include being able to plan your transplant surgery. For anyone who would like to consider being a donor, there is a contact number for the team below who will be able to provide more information and talk through the steps that are involved.
If you are considering a social media campaign for live donation, please discuss this with us. We can carefully guide you regarding the correct processes around this.
Live Donor Co-ordinator
For more information about this program please contact the Live Donor
Co-ordinator.
Section 3 – Liver Transplant Surgery & Complications
When you are called in
You will be asked to make your way to St. James’s Hospital, Leeds. We will inform you which ward to go to. As storage is minimal please bring only essential items and your medications, leave any valuables at home.
The transplant coordinator will inform you when you need to fast from. On arrival you will be examined to assess the current state of your health. You will have baseline tests carried out.
A close relative or friend may come with you, they may also accompany you to the waiting area in the Operating Theatre.
Accommodation for relatives
When you are called in for the operation your relatives might want to stay nearby for a day or two. There is a hotel in Bexley Wing which the ward staff can help you to book. Alternatively (or if the hotel is fully booked) there are local hotels nearby.
The operation
The length of time for liver transplant surgery is unpredictable and once completed, a member of the team will your contact your relatives.
You will have a large wound across the upper half of your abdomen. This wound will be closed with metal staples which will be removed around 14 days after your operation. During the operation drainage tubes will be inserted in your abdomen. These will usually be removed during your
in-patient stay.
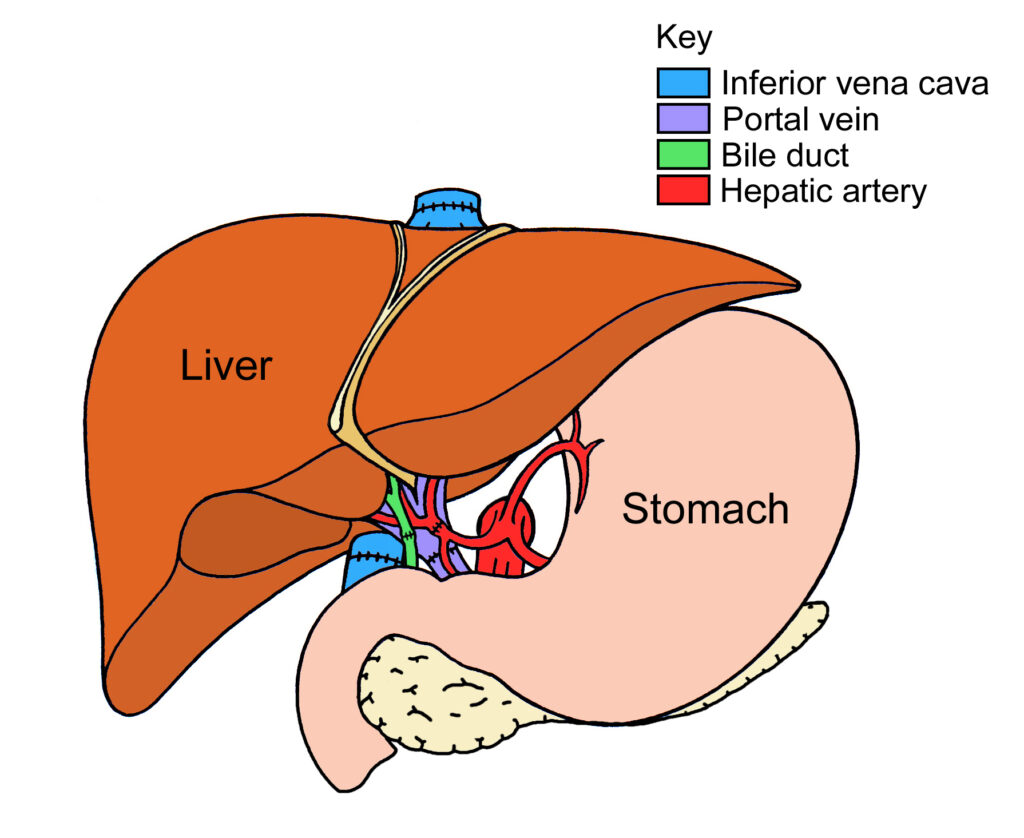
During the surgery multiple joins (anastomoses) are made between the donor blood vessels and your blood vessels. The surgeon will also connect the drainage channels in the donor liver (bile ducts) either to your bile ducts, or in certain cases, a Roux loop will be formed.
Your gallbladder will be removed with your old liver and this is unlikely to cause you any problems in the future.


Section 4 – General Anaesthesia Intensive Care
& Complications
About the anaesthetic
Transplants are carried out under General Anaesthetic.
The anaesthetist you see during your assessment will not necessarily be the same one who puts you to sleep for your operation.
When you are brought to the operating theatre, you will still be awake and aware of your surroundings.
You will be brought into the main operating theatre and transferred on to the operating table. At this stage, you will be connected to a number of monitors, so that we can observe your heart rate, oxygen levels and blood pressure, while you are asleep.
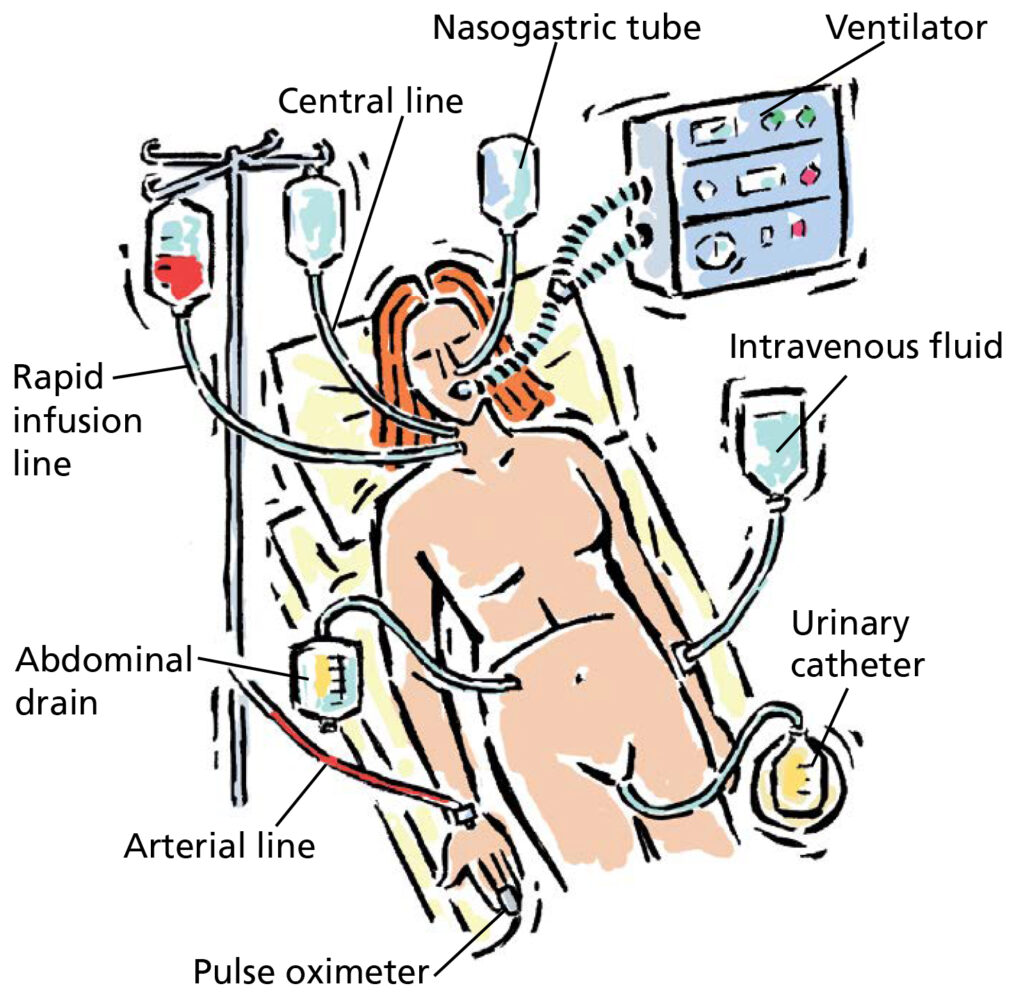
A cannula will be placed and an anaesthetic drug injected through it, which will send you off to sleep. Once you are asleep, various lines will be inserted for monitoring.
An arterial line
This is a small tube placed into the artery in your wrist. This enables monitoring of your blood pressure and heart rate.
A central line
This is a tube placed into one of the large veins in the neck. This enables us to give you concentrated drugs which could not be safely given into a small vein in your hand.
Tracheal tube
This is a tube into the trachea or windpipe, which is used to provide oxygen and to assist you with your breathing during the operation (it is connected to a life support machine).
Nasogastric tube
This is a small soft plastic tube, which passes through the nose and down the throat into the stomach.
Blood products
You may be given blood transfusions or transfusions of plasma to help blood clotting and to compensate for any blood loss during the surgery.
At the end of the operation, you will be transferred to the intensive care unit. Some patients are woken up before being moved to the ICU and others are kept asleep. The majority of patients stay in the ICU for up to 48 hours before being transferred back to the ward.
Is the anaesthetic dangerous?
Anaesthetics have very minor side-effects which though normally well tolerated, but may be a problem for those who are extremely sick or who are having complex surgery.
It is common to feel a bit drowsy or nauseated after a general anaesthetic. It is also common to have a sore throat.
There is a small risk, 1 to 2 in every 100 patients, from the various tubes which you will need. They include bruising, damage to blood vessels, or a punctured lung. These side-effects may require additional treatment during surgery.
Because the body is put under a lot of stress during major surgery and transplantation the heart can sometimes develop irregular rhythms called arrhythmias.
Very rarely people develop unexpected allergic reactions to the drugs used for the anaesthetic. However when this does occur it can be serious and sometimes fatal.
Intensive care
Transplant surgery
Complications that may arise
The terminology we have used is explained below:
- Uncommon: (<10%): less than one person in every hundred undergoing liver transplantation.
- Common: (10% or higher): approximately 10 in every 100 people undergoing liver transplantation.
Overall risk with liver transplantation
Nationally the survival rate one year after a liver transplant is greater than 90%. This means that the average patient has a 9 out of 10 chance of being alive and well 12 months after the transplant.
Common complications after surgery
Pain and discomfort after surgery is to be expected. You will first have a hand held pump containing morphine to help control pain. Later this will change to tablets.
Feeling confused after the operation is common in the first 48 hours. It is partly due to the effect of the general anaesthetic wearing off and can also be due to either the pain or the medications we are giving you.
If patients have encephalopathy (a form of confusion) due to their liver disease before the transplant, this can take several days to improve.
The bowel can sometimes be slow to work and constipation is common. If the bowel becomes temporarily lazy it can cause abdominal swelling (distension) and nausea or vomiting. This is called an ileus.
There is a risk of chest infection, urine infection and wound infection.
Uncommon complications after surgery
The donated liver, sometimes doesn’t work. This is called primary non-function (PNF), the chances of this happening is around 2 in every 100 transplants performed. If possible you will be considered for a second emergency transplant. Sometimes people are too unwell for another operation or do not survive to receive a second liver.
Occasionally a blood clot develops in the blood vessel supplying the liver, the hepatic artery. This happens in between 2 and 5 in every 100 transplants. This is called hepatic artery thrombosis (HAT) and if it occurs very quickly after the transplant and you are well enough, you will be considered for a second emergency transplant.
Sometimes the donated liver may take a bit longer than expected to work. This is called delayed function which will increase the overall length of stay in hospital and increases your risk of infection.
You may develop complications with your bile duct, occurring in around 10 out of 100 transplants. Early complications include leaking or breakdown of the join of your bile ducts (anastomosis). Later complications include narrowing at the site of the join.
There are different ways of managing these complications.
We will send the fluid that surrounds the donor liver for analysis, occasionally bugs are found that may require treatment.
Blood clots to the leg (deep vein thrombosis or DVT) and lung (pulmonary embolus) are uncommon after liver transplantation. You will be on blood thinning injections during your hospital stay to reduce the risk.
Some patients may require a period of support for their kidneys with a dialysis machine. This may increase your length of stay in hospital but won’t be needed after discharge.
Major cardiovascular events during surgery e.g heart attacks are uncommon.
Donor transmitted disease
Livers are screened but there is still a risk of donor transmitted disease. Any information regarding the donor we feel needs to be shared will be passed on to you, prior to surgery when/if available.
All donors are screened for Hepatitis B, C infection and for HIV infection.
Transmission of cancer from donor to recipient
Rarely we find out that the donor had a cancer at the time of their death. The risk of transmission depends on the position, size, and type of the original cancer. Any necessary change to your follow up will be discussed with you.
The recovery period
After the surgery you will return to the Intensive Care Unit and when clinically stable, moved to Ward 83.
- You will be reviewed daily by the transplant team, bloods taken regularly and have at least one scan of your new liver.
- You will be encouraged to mobilise early to reduce complications and enhance your recovery after liver transplant.
- You will receive education from the liver transplant
- co-ordinators, dieticians and pharmacist about life after transplant. You will receive reading material to support this.
- The length of stay in hospital varies from patient to patient but is usually around 1-2 weeks, depending on your recovery.
Section 5 – Complications of Transplantation in General
Infections
General
The drugs needed after liver transplantation dampen down or suppress the immune system and can make you more prone to infection.
Cytomegalovirus (CMV)
Cytomegalovirus infection is a virus most adults have been exposed to whilst growing up. If you have never had this before and you receive a liver from someone who has, then you are at risk of developing CMV infection and will be prescribed anti-CMV medication for the first few weeks after transplant.
In the context of immunosuppression, CMV can also be reactivated and you may require treatment for this. Symptoms associated with CMV include fever, diarrhoea, lethargy, difficulty swallowing and shortness of breath.
Seek medical attention if you develop any of these symptoms.
The number of superbugs in the UK is increasing. The hospital has strict source isolation policies for patients at risk. These include MRSA and CPE. It is essential that anyone entering the ward should wash their hands at the sinks provided. There are hand gel dispensers throughout the ward and at the end of each bed.

Other general complications
Rejection
Your immune system will recognise the donated liver as being “foreign” ie – not a normal part of you and will try and fight it. This is why you need to take regular medications.
However, rejection is quite common in the first few weeks after transplant – up to a quarter of patients may have at least one episode. A liver biopsy may be required for diagnosis of, and to give us an indication of the severity of the rejection. Rejection can be treated, usually this is with an increase in the doses of your anti-rejection medications, and this sometimes will need to be in hospital. Very occasionally rejection can progress and become chronic which will impact on the long-term health of your liver transplant.
Longer-term medical problems
Certain medical conditions become more common after transplantation. This is partly due to the immunosuppressant drugs. Common ones include: diabetes (either new, or more difficult to control), high blood pressure, high cholesterol, kidney impairment (but true kidney failure needing dialysis is rare).
Weight gain
This commonly can occurs after transplantation and increases your risk of other medical problems, including the development of fat in your new liver. Your weight will be monitored in the post transplant clinic and a referral to a dietician made if we have concerns about weight gain.
Cancer
Following liver transplant there is a small increased risk of all types of cancer. Smoking greatly increases the risk of cancer developing after a transplant and this is why we advise you to stop smoking.
Specifically related to liver transplant are skin cancers and blood cancers (lymphoma).
Recurrence of disease
This is well recognised for many sorts of liver disease. If your original disease comes back into the new liver it may not progress in the same way as previously.
Here are some examples:
If you were transplanted for liver cancer (hepatocellular carcinoma), there is a 10% overall risk of recurrence.
Liver diseases that can recur after transplant include Primary Sclerosing Cholangitis, Primary Biliary Cirrhosis and Auto- Immune Hepatitis.
If you are transplanted for alcohol related liver disease, this should not recur if you continue with life-long abstinence.
If you are transplanted for Metabolic dysfunction Associated Steatotic Liver Disease (MASLD) you will be encouraged to maintain a healthy weight to prevent this being a recurring problem in the transplanted liver.
New liver disease
In addition, new liver diseases can occur just as in anyone else. If your liver tests become abnormal after the liver transplant, investigations for new diseases may be performed.
How the waiting list works
Donor after brainstem death livers
DBD livers are matched to people using a set of criteria called the Transplant Benefit Score (TBS). This scoring system is designed to try and ensure the greatest number of patients get access to an organ at the right time.
This scoring system takes into account a number of variables including patient age, cause of liver disease, bloods and symptoms of liver disease. We can explain this in more detail if required. The TBS score determines your place on the national liver transplant waiting list. Your position may change depending on your clinical condition.
Donor after circulatory death
This is a second type of waiting list managed by the Leeds Liver Unit, utilising organs that originate from a specific geographical locations.
Much like the DBD list, the aim of this list is to transplant those with the greatest need first. Machine perfusion can be used in this type of donor liver.
Increasing access to liver transplantation
There are several ways that we can increase the number of donor livers that we can use for transplantation. This includes use of livers from donors who have previously had hepatitis B or C, and from those who currently have these infections.
The use of machine perfusion has also increased the number of liver offers in the UK.
Machine perfusion
We now use machines to assess the function of the donor liver before it is implanted. This may reduce the number of biliary complications associated with DCD liver transplants. Machine perfusion has a role in increasing the number of liver offers as previously we may have not accepted a liver for transplant based on the information available, however we can now look at the liver and its function in more detail before making a final decision about transplantation.
There is more information on machine perfusion in a separate leaflet that will have been provided to you.
Hepatitis C donors
Due to breakthroughs in Hepatitis C virus treatment it is now possible to consider using organs from donors infected with Hepatitis C virus for transplantation. Please see leaflet LN004721 – Use of Hepatitis C Infected Organs in Hepatitis C Negative Recipients. Link below:
Hepatitis B donors
Livers previously exposed to hepatitis B have been used for many years and an additional daily medication to prevent this causing a problem for you is needed. If we feel you might need to consider accepting a liver from a donor who still has active hepatitis B, what this means for you will be discussed in detail.
Waiting list review
Once a month, the transplant team meets to discuss all patients active on the liver transplant waiting list at Leeds.
During these meetings clinicians have the opportunity to highlight patients who they are particularly concerned about to ensure that all opportunities for transplant have been explored. Sometimes in these meetings the types of donor liver you are suitable for may change – taking into account your health as well as your need for transplant.
Any changes to your transplant plan will always be discussed with you by a member of the team.
Section 6 – Waiting on the Transplant List
Waiting for a liver
This can be a very difficult time for both patients and their friends and relatives. We do not know how long you will have to wait and it is likely that it will be several months to years. We advise that you try and carry on life as normally as possible, following your usual routine and continuing your work if possible.
You can continue to see family and friends and could consider taking short holidays within the UK.
If you want to go away for a few days ring the co-ordinators and discuss where you plan to go and how you can be contacted or if you wish to be suspended.
You also need to let us know if any of your contact details change or if you are admitted to your local hospital.
Outpatient visits
You will need to be seen regularly in the transplant waiting list clinic. We aim to share your care with your local hospital. If you need transport for these visits, you need to book this via your GP.
During the appointment you may be seen by multiple members of the team and it may not always be a Doctor performing your consultation.
Please bring a list of your medications, exercise journal and any questions you have.
At your appointment your pulse, blood pressure weight and an assessment of your frailty will be routinely monitored. You will need to have blood tests after seeing the team.
Liver scans whilst waiting
Most patients will require a scan whilst waiting. For patients with cirrhosis the minimum will be an ultrasound scan every six months to look for the development of new nodules in the liver.
- Patients with liver cancer will require an MRI scan every three months and a CT scan every six months to ensure that their cancer has not grown outside the limits for transplantation.
- If you are on the transplant waiting list for longer than one year we will repeat your echocardiogram to ensure that you remain well enough for a transplant.
Clinical deterioration whilst waiting for your transplant
It is important that you are aware that being listed for a transplant does not guarantee that you will receive a transplant. Between 10-15% of patients will unfortunately become too unwell or die whilst waiting.
If you feel your condition is deteriorating, please let us know as it may be necessary to bring your appointment forward or advise you to attend your local hospital. If admitted to hospital please let us know and ask the medical team looking after you to contact us.
Sometimes we need to suspended patients on the waiting list, either pending further investigations or to allow improvement in fitness or to recover from recent illness.
If you reach a point where you are likely to be better off without a transplant we will remove you from the waiting list. This does not prevent you from being reassessed again in the future if things change.
Carers
It is very useful for someone else to attend appointments with you. They can provide useful up to date information if you become unwell.
A guide to looking after yourself before your transplant
Your aim should be to keep yourself as fit, healthy and as active as possible whilst you wait for a liver transplant. You may have been given the “Keeping active on the waiting list“ leaflet, please complete this and bring to clinic with you each time.
Dental care
Visits to the dentist are It is important to continue with regular dental checks. Poor oral hygiene may lead to infection.
If you require dental work, your dentist may recommend referral to a dental hospital rather than in the local practice. This is because you are at greater risk of bleeding.
Driving
If you have ever experienced confusion due to your liver disease (encephalopathy) and been told not to drive please DO NOT drive. If you continue to drive against medical advice then we will inform the DVLA as you are a risk to yourself and other road users.
Infection
If you experience a fever or feel you have a temperature, please seek medical advice. It may help to have a digital thermometer at home.
Variceal bleeding
If you cough or vomit blood or pass blood from your back passage (this may be dark red or black in appearance), please phone 999 and travel by ambulance to your local Accident and Emergency Department. You may require immediate medical attention.
Flu/Pneumonia/COVID vaccines
Please arrange to have these at your local surgery. The flu vaccine is to be given every year and the Pneumonia vaccine is given every five years. Please take up the offer of any COVID vaccines that you are offered and confirm with your GP that you have been highlighted as an ‘at risk patient’. If you are offered the shingles vaccine then we would recommend that you have this.
Medications
IMPORTANT
Please do not take any anti-inflammatory drugs as this may damage the kidneys and have other side effects in patients with liver disease e.g. Ibuprofen, Neurofen, Naproxen and Diclofenec etc.
Please do not take sleeping tablets sedatives or strong pain killers without discussing with your doctors, as you are already at risk of drowsiness and confusion due to your liver disease.
Pregnancy
You cannot be pregnant whilst waiting for a transplant. We can provide advice on contraception if required.
Patients support group
Please ask the coordinators for more information.
Section 7 – After Discharge & General information
Going home
When the team are happy with your progress, blood results and you understand your medication you can be discharged home. Occasionally it may be necessary to transfer you to your local hospital before going home.
Transplant clinic
This is held every Tuesday morning. At first you will need to come every week but the frequency of visits will gradually be reduced. In the longer term we endeavour to share your post transplant care with your local team.
Readmission
Readmission is very common after transplant – do not be disappointed.
Just like whilst waiting for transplant, if you are admitted to your local hospital after transplant please let the coordinators know.
Research
The Leeds Liver Unit actively participates in research programmes. If there are projects or trials which are relevant to you and your condition we will approach you to discuss these and provide information. Participation is your choice and will not affect your place on the transplant waiting list or the care you receive.
Section 8 – Contacts
Contacts numbers
Ward J83
Intensive Care Unit (Ward J54)
Liver Recipient Co-ordinators
An answerphone service is available. Please speak clearly and leave your name and contact telephone number and we will return your call, although this may not be the same day.
If your call is urgent please contact: Ward J83 – 0113 20 69183