Adverse reactions to insect bites
Bee and wasp stings can cause life threatening anaphylaxis, previous stings are a risk factor and hence venom allergy is more common in beekeepers and gardeners. Referrals should be made as below. Beekeepers should be advised to give up their hives if they have had anaphylaxis to a bee sting. Select patients will be eligible for immunotherapy/desensitisation.
There are no standardised effective treatments beyond antihistamines for individuals who have a marked response to none bee/wasp stings. e.g. midge/mosquito bites leading to localised inflammation. In such cases insect repellents (e.g. Deet), high dose antihistamines e.g. Fexofenadine 360mg BD and a short supply of prednisolone 30mg OD for 3 days are suggested. There is no additional investigations or therapies that are available and hence we do not appoint these patients.
Routine referral criteria
History of anaphylaxis or systemic symptoms (urticaria, angioedema, wheeze, hypotension) within an hour of a wasp/bee sting.
History of localised reaction (erythema, angioedema at sting site) to bee and/or wasp venom in an individual at high risk of subsequent stings due to occupational exposure e.g. fruit picker, gardener.
Not to refer
Localised reaction (erythema, angioedema at sting site) to a bee and/or wasp in an individual without an occupational risk
Adverse reactions to insects which are not bee or wasps
Adverse reactions to food
IgE mediated food allergy- life threatening
IgE mediated food allergy is manifest by a small range of symptoms, nearly always including urticaria and angioedema on ingestion of the potential allergen. Common allergens include nuts, seafood, and eggs.
Where there is a suspicion of a food allergy a specific IgE to the food should be performed before referral.
IgE mediated food allergy- Oral allergy syndrome
Oral allergy syndrome is an IgE mediated food reaction. It rarely leads to life threatening reactions and an adrenaline autoinjector is rarely warranted. It is characterised by immediate onset mouth, palatal and throat itching on ingestion of raw fruits, vegetables, and nuts. While occasionally there may be mild throat and lip swelling, life threatening anaphylaxis is rare as the allergen is quickly digested to a non-allergic form by gastric secretions. Similarly, cooking the allergen will render it inactive and hence patients will tolerate roasted nuts and cooked fruit, but not the raw form.
Oral allergy syndrome is a clinical diagnosis, where the symptoms are convincing, and mild the patients do not need to be referred. The following website provides useful patient information:
Oral Allergy Syndrome (Pollen Food Syndrome) | Allergy UK | National CharityCases where the history is less clear should be referred.
Food intolerance
Symptoms of brain fog, headache, bloating, constipation, diarrhoea and abdominal discomfort related to food are symptoms of an intolerance not allergy. A referral to an allergist for further assessment is unlikely to identify any obvious triggers. We do not accept referrals for food intolerance, there are no validated blood or skin tests for food intolerance. Non-NHS tests such as hair sample testing, IgG testing (York Test) are not recommended.
IgE RAST tests are not indicated for food intolerance.
Patients should be directed to the following website:
Allergy vs Intolerance | Allergy UK | National CharityAdverse reactions to alcohol
Flushing and hives in response to alcohol are not IgE mediated There is not a significant risk of anaphylaxis. The effects are usually dose dependent. Apart from avoiding culprit drinks no further investigation or intervention ids required.
Eosinophilic Oesophagitis (EoE)
Understanding of EoE has changed over the last 5 years, the basis of the disease is not IgE mediated. As we do not add anything to the care of these patients, we no longer accept them.
Food and eczema
The role between food and eczema is complex, however there is no role for IgE testing in eczema without food allergy symptoms. Atopic individuals will often have a raised IgE and positive IgE tests which are clinically irrelevant.
IgE tests to solely investigate eczema is therefore in appropriate and may lead to undue patient anxiety and food avoidance.
Urgent referral criteria
Multiple suspected food allergy leading to significant dietary restriction
Routine referral criteria
History of suspected IgE mediated food allergy
Not to refer
Food intolerances
Adverse reactions to alcohol
Eosinophilic oesophagitis
Eczema
Allergic rhinitis/rhinoconjunctivitis and non-allergic rhinitis
Rhinitis can be due to a multitude of reasons. ANCA associated vasculitis should be excluded in cases where there is nasal crusting/bleeding by arranging an ANCA test. Cases where there is anti-MPO, and anti PR-3 positivity suggest ANCA associated vasculitis.
Rhinitis can result from both allergic and non-allergic causes. Both forms result in similar symptoms, namely, sneezing, congestion, nasal discharge, and allergic conjunctivitis. It is important to establish whether the rhinitis is allergic in nature as this affects management. The Allergy Service is particularly keen to see those patients for whom desensitisation therapy is appropriate.
Allergic rhinitis
This can be divided into:
- seasonal allergic rhinitis
- perennial rhinitis (also known as persistent rhinitis).
Seasonal allergic rhinitis
This is most commonly due to grass pollen allergy (hayfever) which occurs from June-August and tree pollen allergy which can run from the end of February to April. A smaller group has an isolated allergy to moulds which sporulate in the autumn.
In patients where there is allergic rhinitis the following can be implemented in primary care:
- High dose non-sedating antihistamines e.g. Fexofenadine 360mg BD, or Loratadine 20mg BD (these are off-licence doses which are known to be safe as per BSACI guidelines for chronic spontaneous urticaria). In pregnancy or lactating women only licenced doses should be used.
- Nasal spray
- Steroid nasal spray such as Fluticasone or Beclomethasone. Correct administration technique is important, please advise the patient, an information leaflet can be found here (second page) https://www.bsaci.org/wp-content/uploads/2019/12/Howtouseanasalspray.pdf
- Where steroid nasal spray fail, Azelastine/Fluticasone preparation (Dymista) may be considered
- Eye drops- either Sodium cromoglycate or Olopatadine.
- If there is concomitant asthma, control should be optimised as immunotherapy/desensitisation is contraindicated in cases where the patient has poorly controlled asthma.
- In individuals who have asthma like symptoms during the pollen season a steroid inhaler may be considered.
Perennial rhinitis
Allergic rhinitis which is persistent is nearly always in the United Kingdom secondary to house dust mite allergy. Management strategies for persistent rhinitis are similar to those outlined for seasonal rhinitis.
A subgroup of patients may have perennial rhinitis due to animal dander (cat, dog) sensitisation and a pet at home. Such patients will often experience relief when away from the animal. Individuals who are allergic to their pets should be encouraged to rehome them in addition to the measures above. Immunotherapy/desensitisation to animal dander is often poorly tolerated and reserved for individuals who have occupational risks e.g. Veterinary surgeons and nurses, animal handlers, farmers.
Non-allergic rhinitis
Non- allergic rhinitis presents in a similar nature to perennial rhinitis; however, the symptoms do not co-exist with allergy conjunctivitis type symptoms. It typically presents later in life and is less responsive to antihistamines and tends to be watery in nature.
It may be made worse by temperature changes, sulphite rich foods and often co-exists with Aspirin Exacerbated respiratory disease.
A negative specific IgE RAST to an aeroallergen mix in the context of a normal or high IgE and supportive clinical features are enough to make a diagnosis of non-allergic rhinitis. Patients who have been seen by community ENT and have negative skin prick tests are likely to have non allergic rhinitis.
The following should be implemented where there is a suspicion of allergic rhinitis:
- Up to four times the licenced dose of a non-sedating antihistamine e.g. Fexofenadine 360mg BD.
- Ipratropium Bromide nasal spray, 2 sprays each nostril 2-3 times a day
- A trial of Montelukast 10mg once at night
Routine referral criteria
There is severe disease (poor quality of life, decreased function) AND an inhaled
allergen mix specific IgE (available for testing in the laboratory) has been undertaken AND the advice above has been trialled
Not to refer
Patients who have been assessed by the ENT team and have negative skin tests and blood tests. These patients are likely to have non-allergic rhinitis.
We do not offer an aspirin provocation or desensitisation service for Aspirin Exacerbated Respiratory Disease
Mast cell activation syndrome
As outlined in the existing consensus criteria (J Allergy Clin Immunol Pract. 2019 Apr;7(4):1125-1133.e1.), the diagnosis of MCAS requires the simultaneous presence of three key criteria:
- Typical Clinical Signs: The patient should exhibit severe recurrent acute systemic mast cell activation features, meeting the criteria for ‘idiopathic anaphylaxis’ with involvement of at least two organ systems.
- Biochemical Analyses: Mast cell involvement must be demonstrated through biochemical analyses. An increase in tryptase to >20% of baseline plus 2 ng/ml is indicative of mast cell activation.
- Response to Treatment: Symptoms should respond to treatment with mast cell stabilizing agents or drugs targeting mast cell mediator production, secretion, or receptor binding (e.g., antihistamines, dodium cromoglycate).
We accept referrals for patients who have the typical clinical features which are synonymous with idiopathic anaphylaxis. We will also see patients who have acute episodes of profuse urticaria/angioedema with simultaneous acute episodes of gastrointestinal symptoms (typically diarrhoea and abdominal cramps) as this would constitute 2 organ systems.
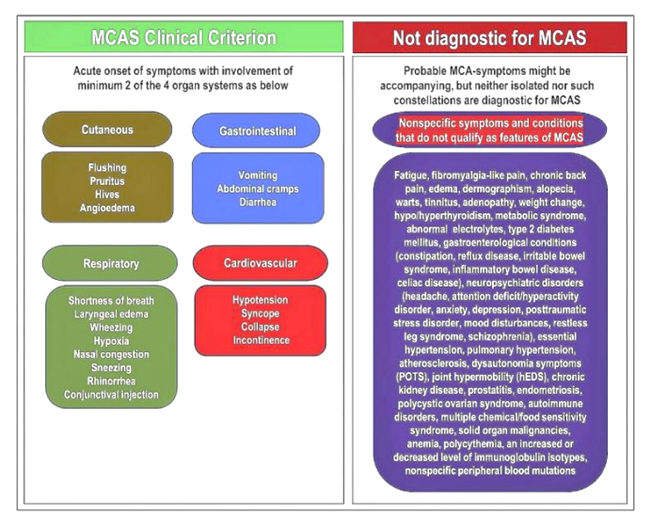
We do not accept referrals regarding patients with unsubstantiated MCAS, as well as those presenting with complaints historically associated with MCAS but later found to be independent of mast cell activation, such as:
- Postural orthostatic tachycardia syndrome or hypotension
- Hypermobility-type Ehlers-Danlos syndrome
- Chronic fatigue
- Fibromyalgia
- Brain fog
We will not see patients who have non-specific symptoms attributed to MCAS as highlighted in figure 1 on the next page.