Drug allergy
The general drug allergy service offers drug skin prick testing, intradermal tests, and challenge testing where appropriate. The diagnosis of a drug allergy is largely based on history and so any details/history are valuable. Please note that an adrenaline autoinjector is not required for a suspected drug allergy.
Further information can be found on:
Drug Allergy: Diagnosis and Management (leedsth.nhs.uk)Notably, challenge tests are associated with their own inherent risks and some patients are not suitable for investigations. Commonly investigated drugs include penicillin, other anti-microbials, contrasts media and local anaesthetics.
Penicillin allergy
Due to a high volume of referrals, we only accept patients for penicillin allergy investigations if they meet NICE criteria:
- Penicillin is needed for a treatment for a disease or condition that can only be treated by a beta‑lactam antibiotic
- The patient is likely to need beta‑lactam antibiotics frequently in the future (for example, people with recurrent bacterial infections or immune deficiency) or
- The patient is allergic to penicillin, and cannot tolerate or is allergic to another antibiotic.
NSAID allergy
NSAIDs are well recognised as a cause for urticaria and angioedema, severe asthma exacerbations and occasionally anaphylactoid reactions. These reactions can occur even if the patient has tolerated NSAIDs in the past.
NSAIDs are well recognised as a cause for urticaria and angioedema, severe asthma exacerbations and occasionally anaphylactoid reactions. These reactions can occur even if the patient has tolerated NSAIDs in the past.
Patients with such reactions should avoid all NSAIDs and be vigilant to avoid over-the-counter preparations e.g. cold or flu remedies should be checked). They can have alternative analgesia such as Paracetamol or Codeine. Allergy testing is not likely to be of benefit since skin prick tests are not well validated for this class of drugs.
As per NICE guidance Recommendations for people who have had a mild allergic reaction (i.e. no features of anaphylaxis, no asthma exacerbations, but had mild angioedema and urticaria) to a non-selective NSAID but need an anti inflammatory:
• Discuss the benefits and risks of selective cyclooxygenase 2 (COX 2) inhibitors (including the low risk of drug allergy)
• Consider introducing a selective COX 2 inhibitor at the lowest starting dose with only a single dose on the first day.
Do not offer a selective COX 2 inhibitor to people in a non-specialist setting if they have had a severe reaction, such as anaphylaxis, severe angioedema or an asthmatic reaction, to a non-selective NSAID. Consider referring individuals who’ve had a severe reaction to NSAIDs and would benefit from access to a COX 2 inhibitor (e.g. has active inflammatory arthritis).
Anaesthetic drug allergy
The anaesthetic drug allergy clinic offers investigation of patients who may have had perioperative anaphylaxis.
Urgent referral criteria (consider a phone call discussion when making these referrals)
Patient needs a drug for treatment of a current infection and there are no other options e.g. Benzathine penicillin for Treponema pallidum infection.
Local anaesthetic allergy where clarity regarding allergy status is required before a procedure e.g. dental work
Suspected contrast allergy which is preventing urgent imaging
Routine Referral
Penicillin drug allergy referrals which meet NICE criteria
Multiple antibiotic allergy which is limiting treatment options
Other drug allergies where investigation would help ongoing care e.g. paracetamol
severe reaction to and would benefit from access to a COX 2 inhibitor (e.g. has active inflammatory arthritis)
Not to refer
Side effects to drugs
Patient is very clear that they would not want to be re-exposed to the drug again
Immunodeficiency
Immunodeficiencies are disorders of the immune system that manifest with unusual/severe/persistent or recurrent infection. These may be primary where this an inherent problem with the immune system, these are rare and often have a genetic basis. Alternatively, there may be secondary immunodeficiency where there is an insult to the immune system due to another disease process (e.g. thymoma or malignancy) or therapeutic agents (steroids, DMARDS, B cell depleting agents, antipsychotics).
A high degree of suspicion is required to suspect and refer an individual with an immunodeficiency. Consequently, the service is open to advice and guidance as well as referrals beyond the criteria below which serve as a guide.
Routine Referral
Documented evidence of severe/persistent/unusual/recurrent infections.
Examples of unusual infections include:
Confirmed infections with environmental (non-tuberculous) mycobacteria. E.g. ≥2 episodes of atypical mycobacterial infection with onset under the age of 30 is suggestive of Mendelian susceptibility to Mycobacterial disease.
- Laboratory investigations suggestive of immunodeficiency.
- A secondary immunodeficiency is suspected, and this is associated with significant problems with infections while the primary cause cannot be reversed.
Not to refer
IgA deficiency with no increased rate of sinopulmonary infection
Low IgM in isolation
Recurrent non-invasive Herpes Simplex infection
Recurrent urinary tract infections
Interpretation of immunoglobulin results
Immunoglobulin interpretation and myeloma screen
Immunoglobulins are increasingly requested; the following advice is tailored for adult patients. A myeloma screen (serum electrophoresis and urine electrophoresis/urine for Bence jones protein) is done to exclude a monoclonal component. In the absence of a monoclonal component there is little value of repeating immunoglobulins any more than at monthly intervals unless there is a specific indication to do so e.g. prior to giving B cell depleting agents such as Rituximab.
Serum electrophoresis
The immunology laboratory will add on serum electrophoresis where appropriate, usually in cases where there is an abnormal immunoglobulin result. This is to exclude a monoclonal component.
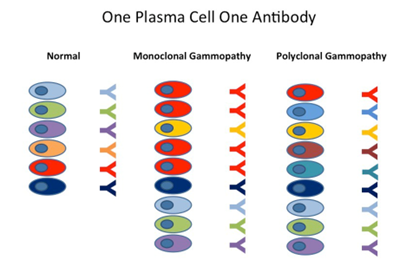
One plasma cell will only secrete one type of antibody targeted to one specific antigen (antibodies are also known as gamma globulins). In healthy individuals there should be an endless array of antibodies. However, in certain plasma cell disorders there will be expansion of one specific plasma cell, a “clone” which will produce one type of antibody known as a monoclonal gammaglobulin or a paraprotein. Serum electrophoresis can detect paraproteins and other patterns such as an acute phase response or a polyclonally raised immunoglobulin which is more likely to represent infection/inflammation.
Paraproteins
Small paraproteins can be seen in persisting severe infections transiently. They can also be seen in monoclonal gammopathy of uncertain significance (MGUS), myeloma and lymphoma. Newly identified paraproteins results are authorised by laboratory staff with comments to direct the requesting person.
Urine electrophoresis (urine for Bence Jones protein)
Antibodies are made up of heavy chains and light chains, there are two types of light chains known as kappa and lambda. In certain forms of myeloma an excess and abnormal light chains can be seen in the urine, these are detected as a ‘Bence Jones’ protein
Low IgA
A completely absent IgA level in isolation is likely to represent complete selective IgA deficiency. Depending on the population it can affect up to 1 in 600 individuals. It is associated with a slight increase in the risk of infection, atopy, and autoimmunity but not to the extent that require surveillance or intervention.
Most patients will be asymptomatic, but a minority will get recurrent bacterial sinopulmonary infections and these patients should be referred.
Patients may find the following website useful:
Selective IgA deficiency – Immunodeficiency UKAn isolated low but detectable IgA is also most likely due partial IgA deficiency. It is unlikely to be of any clinical significance. There is little value in monitoring immunoglobulin levels for IgA deficiency.
An isolated low but detectable IgA is also most likely due partial IgA deficiency. It is unlikely to be of any clinical significance. There is little value in monitoring immunoglobulin levels for IgA deficiency.
High IgA
IgA is predominantly produced and secreted in mucosal sites such as the gastrointestinal tract and the lungs. A raised IgA is a non-specific finding, and causes include mucosal and/or hepatobiliary infection and or inflammation:
Respiratory
- Bronchiectasis
- Chest infection
Gastrointestinal
- Inflammatory bowel disease
- Gastroenteritis
Hepatobiliary
- Any form of liver disease including metabolic dysfunction-associated steatotic liver disease, drug induced liver derangement
- Cholecystitis
- Excess alcohol intake
Renal
- IgA nephropathy
- IgA vasculitis (previously known as Henoch Schoenlein purpura)
Cutaneous
- Cutaneous SLE
- Blistering skin disease
The above offer guidance into the causes of a raised IgA, there should be a clinically balanced assessment into the causes. Conditions such liver disease are relatively common and if this is an established diagnosis this is the most likely cause. There is little value in offering ‘screening tests’ for SLE unless there are supportive clinical features. In the first instance of a raised IgA, a clinical assessment for infection/inflammation, an alcohol history and blood tests for a CRP, full blood count, liver function tests and renal function may be appropriate. There is usually very little value in monitoring a raised IgA, especially if a likely cause is established.
Low IgM
As with any patient with abnormal immunoglobulin results an assessment to determine if they have B type symptoms should be made. A low IgM without clinical features of lymphoproliferative disorders is unlikely to be of any clinical significance. IgM is affected by immunosuppressive agents including corticosteroids, DMARDS and B cell depleting agents such as Rituxumab. Low IgM levels in isolation are not a cause of concern, providing there is no frequency of bacterial infection. Furthermore, there is increasing evidence that IgM levels decline with age and are lower in males, consequently in older individuals a low IgM is likely to be benign.
A complete absence of IgM and recurrent unexplained bacterial infections may represent selective IgM deficiency. Whilst this is a known disorder it is incredibly rare, such patients should be referred on the basis of severe recurrent infection.
High IgM
A high IgM is a non-specific marker of infection and/or inflammation, particularly in the acute phase. This includes bacterial and viral infection as well as flares of connective tissue disease. Furthermore, Primary Biliary Cirrhosis is known to cause a raised IgM. Consequently, the following assessments and investigations should be considered in a patient with a high IgM:
- clinical features of infections e.g. fever, cough, dysuria, night sweats
- clinical features of connective tissue disease: malar rash, synovitis
- clinical features of lymphoproliferative disorders: weight loss, night sweats, lymphadenopathy
- Investigations: FBC, LFTs, U+Es, CRP, serum and urine electrophoresis, ANA (if features of connective tissue disease), viral screen including EBV, CMV, Hepatitis B, Hepatitis C, HIV dependent on risk assessments, tissue autoantibodies (if LFTs are deranged).
If the CRP is raised it is more pragmatic to monitor the CRP than a raised IgM.
Low IgG
The causes of a low IgG are similar to a low IgM. However, protein loss and/or catabolism as seen in nephrotic syndrome, inflammatory bowel disease, protein losing enteropathy and sepsis are more common causes of a low IgG. IgG levels will mirror serum albumin levels, hence repeating Immunoglobulins when the albumin normalises in a hypolbuminaemic patient is usually the first recommended step. Other secondary causes include immunosuppressive agents including recurrent courses of corticosteroids. Patients with a marginally low IgG (>5g/l) and an attributable cause such as recurrent courses of corticosteroids in COPD do not need to be referred unless the frequency of infection is disproportionately high. A discussion with the on-call immunologist or advice and guidance may be appropriate in the first instance.
A low IgG is more concerning than a low IgA or IgM and there should be a lower tolerance of referring patients especially if there is an increased frequency of infection.
High IgG
A high IgG reflects an ongoing inflammatory response. A myeloma screen should be completed in the first instance. Causes of a high IgG include:
- Any infection including HIV
- Connective tissue disease, especially Sjogrens disease and SLE
- Other autoimmune disorders e.g. Autoimmune hepatitis
- Any form of severe liver disease can cause a raised IgG including alcoholic liver cirrhosis.
- Clonal B cell and plasma cell disorders e.g. myeloma, lymphoma- these diagnoses only need to be considered if there’s suggestive clinical features such as unexplained weight loss, drenching night sweats and lymphadenopathy.
- Sarcoidosis (rare)
- IgG4 related disease (rare)- this only needs to be considered in specific clinical situations such as retroperitoneal fibrosis and autoimmune pancreatitis.
In light of the above the investigative process is similar to that of a raised IgM. Once a likely cause of a raised IgG there is little value in monitoring the levels unless for a specific indication. e.g. in autoimmune hepatobiliary disease where immunoglobulins are a prognostic factor.
Low IgE
A low or absent IgE is not a cause of concern.
High IgE
A total IgE should only be requested alongside specific IgE testing for allergy. A high IgE is rarely a cause of concern and usually reflects a predisposition to atopy. It can be >5000 in atopic disease. The immunodeficiency hyper IgE syndrome is an incredibly rare cause of a raised IgE and is associated with recurrent infections and lung infections. A patient suspected of having hyper IgE syndrome should be referred.
Autoinflammatory service referrals
The autoinflammatory service is one of a small handful in the UK. It manages patients with periodic fever syndromes as well as acquired autoinflammatory syndromes including VEXAS. These disorders present with episodes of sterile pyrexia, neutrophilic dermatoses, unexplained raised inflammatory markers and sepsis like episodes.
The conditions that are managed include, but are not limited to:
- Familial Mediterranean fever (FMF)
- Tumour necrosis factor receptor-associated periodic fever (TRAPS)
- Cryopyrin-associated periodic syndromes (CAPS)
- Familial cold autoinflammatory syndrome (FCAS)
- Muckle-Wells syndrome (MWS)
- NOMID/CINCAE
- Schnitzler’s syndrome
- PFAPA syndrome
- Paraneoplastic Autoinflammation
- VEXAS
- Undifferentiated autoinflammatory syndromes- this makes up a significant proportion of patients seen.
The cardinal feature of autoinflammatory disorders is unexplained fever. Other features include:
- Rigours
- Myalgia
- Synovitis
- Serositis: peritonitis, pleuritis
- Neutrophilic dermatoses
- Lymphadenopathy
- Oral and/or genital ulcer
- Unexplained and severe recurrent pharyngitis
These disorders require a high degree of suspicion and hence the service is open to offer advice and guidance when appropriate. In VEXAS cases there is a national VEXAS MDT which may be an appropriate platform to discuss patients who may not be able to travel to our department for an initial appointment.
We will only accept referrals from secondary care after they have had thorough workup to exclude connective tissue disease, occult infection, and malignancy.
As the service is national and patients are required to attend a face-to-face appointment when first attending a thorough local work up is mandated before referral. This should include:
- Investigations to exclude malignancy especially haematological e.g. CT scan, PET CT where appropriate, bone marrow biopsy if indicated.
- Infection screen with a focus on excluding TB which may mimic autoinflammatory disorders.
- Investigations and assessment to exclude connective tissue disease.
- Serial CRPs
- Baseline investigations that are required before starting Anakinra or Tocilizumab including a TB QuantiFERON, Hepatitis B and C screen, HIV screen and a chest X ray.
Routine Referral
Suspicion of a periodic fever syndrome/autoinflammatory disorder as described above.
Not to refer
Connective tissue disease- these should be referred to local rheumatology services.
Oral ulcers in isolation- such cases need to be referred to oral health.
Non-specific symptoms in the absence of recurrent fever and raised inflammatory markers.