Detailed information on all sample types and tests can be found in the test repertoire in the Microbiology User Manual and Mycology User Manual.
To prevent rejection of samples consult the Pathology labelling policy for all specimens sent.
Processing of Microbiology samples is different to other Pathology tests in that organisms may not be isolated and reported, even if present, if not incubated in specific conditions or on certain media or if specific virology assay targets not used.
For all Microbiology samples, relevant clinical details guide the laboratory to set up specimens on the most appropriate media and in the correct atmospheres to look for the target organisms, so it is very important to provide as much information as possible.
Virology testing is also based on algorithms to target the most appropriate assay for the clinical presentation so full information is essential.
Avoiding blood culture contamination when sampling reduces harm to patients from unnecessary investigations and treatment. It also reduces laboratory work and hospitalization costs. The following standard operating procedures should always be followed to minimize this risk (you must be connected to the Trust VPN to view the following information):
- Standard Operating Procedure Blood Culture Sampling in Adults
- Standard Operating Procedure Blood Culture Sampling in Paediatrics
When taking blood cultures observe universal precautions to reduce any potential infection risks through needle stick injuries. Wear gloves when obtaining blood samples to protect yourself.
For adolescents and adults 10 to 20 mL of blood is the minimum volume per set (i.e. aerobic and anaerobic bottle) and 1 to 2 mL for neonates and young children (use the Paediatric blood culture bottle please).
Blood culture samples needed for suspected diagnosis:
- Severe bacteraemia or sepsis: take before commencing empirical antibiotic therapy. Minimum one set of cultures but ideally peripheral and central paired cultures if line is present. If clinically permissible collect samples 10 to 20 mins apart
- Severe septicaemia (meningitis, osteomyelitis, arthritis, pneumonia) 2 sets of cultures before antibiotic therapy commences
- Infective endocarditis: 3 sets of cultures before therapy commences, if antibiotic therapy for infective endocarditis is delayed for 24 hrs collect another 3 sets the next day
- Low grade intravascular infection: 3 sets within 24 hrs best taken at the start of febrile episodes. Best taken before antibiotic therapy
- Febrile episodes: no more than 3 sets cultures over 24 hrs. Bacteraemia may be present 1 hr before febrile episodes
- Fever of unknown origin: 4 to 6 sets over 48 hrs
Labelling
- Follow the Pathology Sample Labelling Policy to prevent delays from rejection of samples due to insufficient details
- The request form should indicate the test requested, and clinical information
- e.g. “Enteric fever after returning from 2 weeks in Mexico”
- “To start on iv cefotaxime” or
- “Purpuric rash, shock, meningococcaemia. To start cefotaxime” or
- “Fever of unknown origin. Not on antibiotic therapy”
- It is essential to indicate if this is a high risk sample and indicate so with Danger of infection stickers
Which Container does it go in?
This sample should be sent to us in Bactec blood culture bottles.
For adult blood cultures use a set of 2 culture bottles (anaerobic and aerobic) for each collected blood sample. Red BUFALO blood culture collecting packs available.
For paediatric blood cultures please use a single paediatric blood culture bottle.
Transport
- Blood culture bottles should be transported to the laboratory with minimum delay. NICE guidelines recommends 4 hours from venipuncture to incubation within the laboratory
- Blood culture incubators are only present on LGI site so it is essential to transport cultures as soon as they are taken
- The bottles can be sent via the air tube system (bottles for mycobacteria SHOULD NOT be sent via the air tube system)
- If the Air tube system is not working porters should be contacted to transport Blood Cultures to specimen reception as soon as possible
- If insufficient Pods are available contact 22622 (LGI) or 65100 (SJH) to request additional carriers
Reporting
- Positive blood culture bottles will be reported to you electronically, followed by telephone notification when we can inform you about the presence of presence of potential organisms via a Gram stain
- During this phone call we will enquire about the clinical condition of the patient, antibiotics used and we will give advice on antibiotic therapy where appropriate.
- In most cases positive blood cultures will be followed up with susceptibility and identification results the following day
General Information
STI check for Chlamydia and Gonorrhoea, (and Trichomoniasis in symptomatic females), is done by NAAT testing. (Aptima sample).
Annual STI check is recommended for all 18-25 year olds.
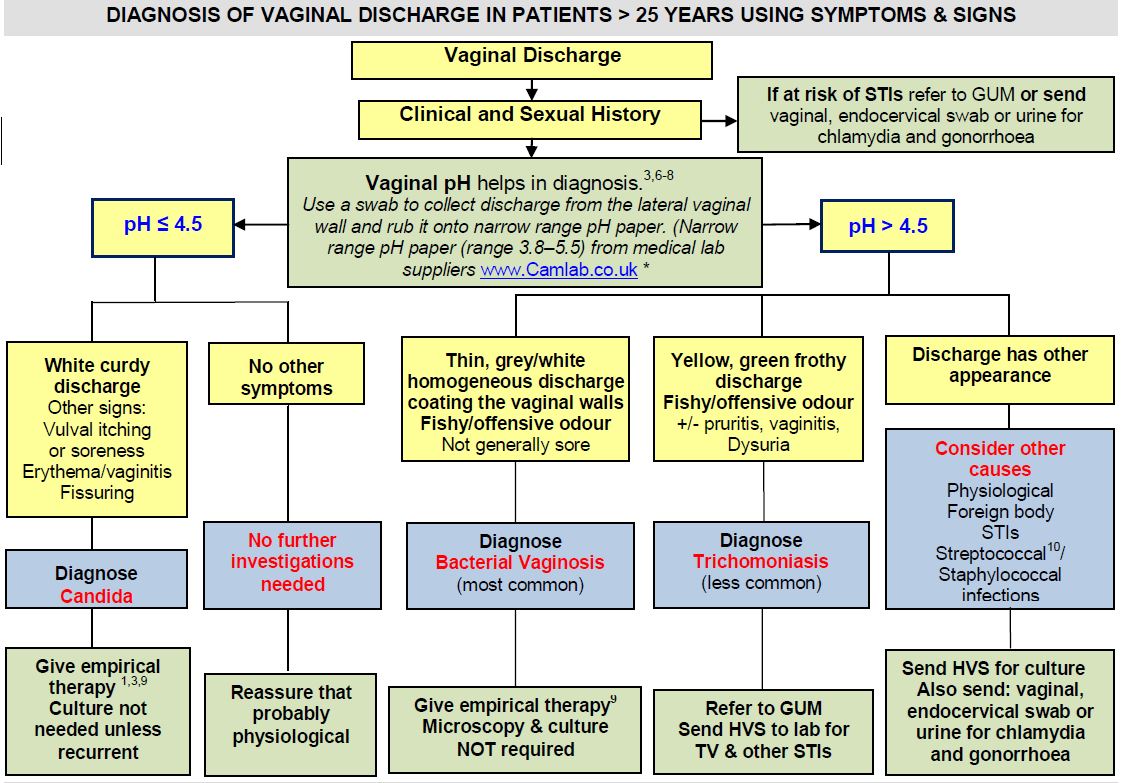
For the investigation of abnormal vaginal discharge, laboratory testing is often unnecessary. Primary investigation should include clinical observations, and testing the vaginal pH – (PHE July 2013).
Downloadable flow chart for Investigation
{kind=link}
LTHT Microbiology do NOT offer diagnostic testing for Bacterial Vaginosis (BV). This diagnosis is made on the basis of clinical observations and vaginal pH. Leeds Sexual Health offer consultancy and a referral service for patients with apparent recurrent or refractory BV.
pH is tested using narrow range pH paper. The paper should be placed directly on the lateral vaginal wall or discharge removed using a cotton bud/Q tip swab.
When requesting laboratory GUS culture tests on Order Comms, the result for vaginal pH will determine the relevant investigations to be undertaken.
Routine” culture of High Vaginal Swabs (HVS) in asymptomatic patients is of no value.
Culture for N gonorrhoeae is only available if there is strong suspicion of gonorrhoea, and treatment is planned. Swabs should be processed within 6 hours. Referral to LSH is recommended in such cases.
For detection of group B streptococci (GBS) in pregnancy, a high vaginal swab may be sent. Note that a positive MSSU with GBS during pregnancy warrants peripartum antibiotic prophylaxis irrespective of GBS status on HVS culture – therefore, sending HVS for screening for GBS is unwarranted in this case.
Intrauterine devices should NOT be routinely sent to the laboratory after their removal. IUCDs are only investigated if there are clinical indications of PID or other inflammatory conditions.
High Vaginal Swab for culture (NB, investigation does NOT include STI screening)
Specimen types you should send:
- High vaginal swab (HVS). Indications for HVS are: –
Symptoms consistent with recurrent thrush, vaginal pH < 4.5
Abnormal discharge NOT consistent with BV or TV, vaginal pH > 4.5
Abnormal discharge in a patient who is > 60 years old or who has dyspareunia or dysuria Group B streptococcal screening in pregnancy
How to collect the sample
- Remove all excessive amount of secretions or discharge
- Obtain samples from the mucosal membrane of the vaginal vault. Use a speculum if available
Which container does it go in?
- HVS for culture: Liquid e-Swab (NB these are not investigated for STIs)
- A guide on the use of liquid swabs
Transport
- Swabs should be transported to the laboratory as soon as possible.
- Cultures for Neisseria gonorrhea are valid up to 24 hours from collection to receipt of sample
Other GUS tests
IUCD – If Actinomyces is suspected or shown in the endocervical smear, separate prolonged culture techniques are required and the clinical information must be clearly stated on the request form
Pregnancy – Group B Strep may cause neonatal invasive disease. Send an HVS for screening. Women known to be carriers of group B strep at onset of labour are offered parenteral prophylaxis
Children- Vulval and penile swabs from children are investigated for skin/soft tissue pathogens including Staph aureus and Group A haemolytic streptococcus.
Suspected sexual abuse – refer urgently to Consultant Paediatrician. Documented procedure for clinical examination and testing, and chain of custody documentation, is mandatory
Culture for N gonorrhoeae – only when GC treatment is planned
Referral to LSH is recommended for investigation/treatment of gonorrhoea
(This will permit rapid laboratory processing and will facilitate contact tracing and expert support)
Chlamydia, Gonorrhoea and Trichomonas vaginalis NAAT testing
An annual STI check is recommended for all 18-25 year olds for infection with Chlamydia trachomatis or Neisseria gonorrhoea (GC)
Screen for Trichomonas vaginalis in patients with dysuria, strong suspicion of infection or with pH greater than 4.5 and a distinctive yellow/green frothy discharge. Vaginal swabs
Testing may also be indicated for eye swabs, use the white aptima collection device for this sample and specifically request Chlamydia/GC.
All samples must be sent in Aptima collection kits. Do not use Copan liquid swabs or UTM red capped tubes for this investigation.
Do not send multiple genital swab requests for MMCS and NAAT testing in the same sample bag as this leads to delays in testing.
Male or Female Urine Specimen Collection Guidance
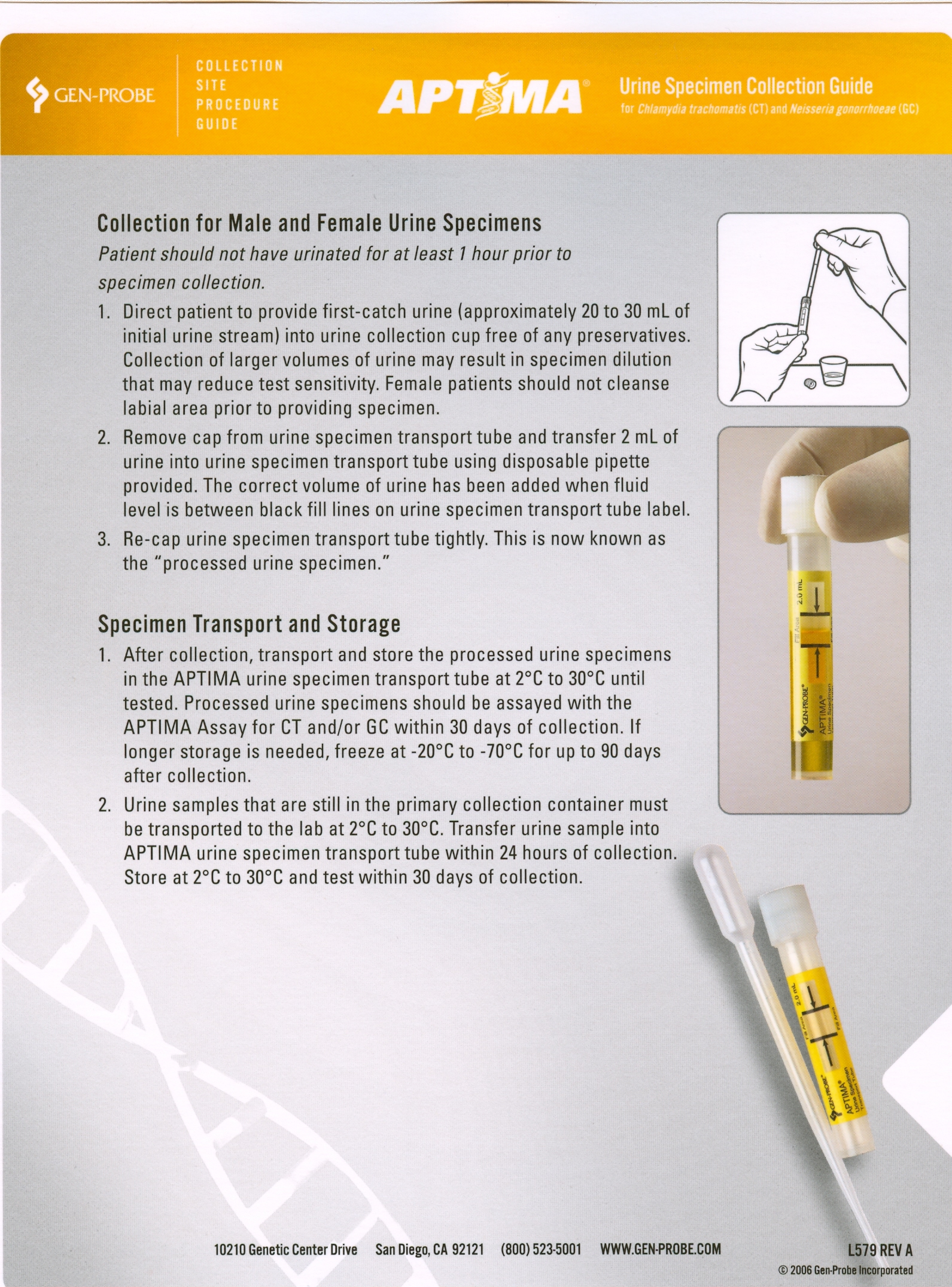{kind=link}
{kind=link}
An annual STI check is recommended for all 18 to 25 year olds for infection with Chlamydia trachomatis or Neisseria gonorrhoea (GC)
Screen for Trichomonas vaginalis in patients with dysuria, strong suspicion of infection or with pH greater than 4.5 and a distinctive yellow/green frothy discharge.
Testing may also be indicated for eye swabs, use the white aptima collection device for this sample and specifically request Chlamydia/GC.
All samples must be sent in Aptima collection kits. Do not use Copan liquid swabs or UTM red capped tubes for this investigation.
Do not send multiple genital swab requests for MMCS and NAAT testing in the same sample bag as this leads to delays in testing.
Microbiology are required to handle a number of potentially high risk organisms which may be a risk to staff. To help the laboratory minimise the risk from these samples, users should include all relevant clinical detail along with Danger of Infection stickers on request forms. This enables the laboratory to recognise samples that potentially may grow Hazard Group 3 Pathogens and therefore should be handled using category 3 precautions.
This below shows clinical details that may suggest potential infection by Hazard Group 3 Pathogens.
| Clinical detail | High risk occupations | High risk sports/pastimes |
|---|---|---|
| IV drug abuser | Hospital or Laboratory staff (exposure incident) | Outdoor Water Sports |
| Return travel/visitor from abroad where HG3 pathogens are endemic | Veterinary / Animal worker | Caving / pot-holing |
| Consumption of unpasteurised products (milk/diary) | Farming, visit to farm | Camping & Hunting in endemic areas |
| Psoas abscess / cold abscess | Slaughter house/abbatoir worker | Animal Hide Drum playing/making |
| Enteric fever | Horse caretakers | |
| HUS – (haemolytic uremic syndrome) | Equine Butchers | |
| Consumption of raw or undercooked meat products | Industrial processing of wool, hide or hair | |
| Meat Packing Plant Employees |
It is the responsibility of the requesting clinician to indicate or highlight that a specimen may contain a HG3 pathogen(s). As per Trust policy this should be clearly stated on the request form and a yellow high risk specimen label attached to the form and specimen. They MUST supply all relevant clinical details as is reasonable and practical at the time of initial clinical assessment.
Where there is a failure to follow this procedure a Datix incident report will be raised for investigation by the requestors CSU.
Guidance on organisms that should be notified can be found on Leeds Health Pathways website (you must be connected to the Trust VPN to view the following information).
Specimen types you should send:
Throat Swabs for bacterial culture: (COPAN e-Swab)
- For throat swabs samples taken from the inflamed areas of the pharynx are most likely to grow the causative organism of acute tonsillopharyngitis
General swabs (i.e. surface wound swabs, skin swabs, ulcer swabs) for bacterial culture: (COPAN e-Swab)
- For a representative sample of a wound it is important that not only pus is sent but more importantly material from the advancing margin of the lesion. For abscesses the walls of the abscess should be firmly sampled
- Open lesions and open abscess (including burns wounds). Decontaminate the skin, sample the exudate from the base or margin of the lesion by firmly applying the swab to it
- Pustules and Vesicles Friction blisters of severe cellulitis are not appropriate for culture
- Vesicular lesions of suspected Chickenpox or Zoster should be sent for virological examination
- Transport the sample to the laboratory as quickly as possible, refrigerate if not being sent immediately i.e within 1hr
- Samples requiring culture for Neisseria gonorrhoeae must be received by the laboratory within 24 hours or the result may not be valid
Sterile Samples (e.g. CSF, abscess pus, synovial fluid, tissue biopsies)
Specimen types you should send:
- Sterile body fluid samples (see list below) obtained for microbiological culture
- Samples should be collected from sterile sites using aseptic techniques
- Please indicate if tuberculosis is a possible diagnosis when collecting samples from sterile sites. Samples and request forms should be labeled with Danger of Infection stickers
- White cell counts other than on CSF samples should be sent on a separate request to Haematology department
- If samples require urgent processing please contact the Microbiology Department
How to Collect the Sample
- For taking lumbar puncture samples please refer to lumber puncture standard operating procedure (you must be connected to the Trust VPN to view the following information)
- Disinfect the skin site thoroughly prior to puncture or incision
- If necessary use sterile gloves and sterile drapes around the incision or puncture site
- Aspirate the body fluid into a syringe and decant the fluid into the sterile container
- Screw the lid back on the container and make sure that it does not leak
List of samples that fall under above sampling recommendations
- Cerebrospinal fluid (CSF)
- Abscess aspirates (from various anatomical locations)
- Pleural fluid
- Ascites
- Bone biopsy
- Tissue biopsy (from sterile anatomical sites e.g. brain, liver, spleen, lymph nodes)
- Bone marrow aspirate
- Synovial biopsy
- Synovial fluid samples – joint fluid aspirates (use same containers for synovial fluid crystal detection – please note that samples for crystal detection should reach the lab as soon as possible)
Transport
- Transport the sample to the laboratory as quickly as possible
- Note: The recovery of anaerobes is compromised if transport time exceeds 3 hours
- Do not refrigerate the sample
When sending stool samples a full travel history and clinical details must be included on request or some pathogens may be missed. If suspected E coli 0157, Shigella dysenteriae or typhoid or details of HUS, PUO or fever following foreign travel mark clearly as Danger of Infection.
For ova, cyst and parasite (OCP) testing please note that administration of barium, oil, magnesium or crystalline compounds can lead to unsatisfactory results. Please delay specimen collection for at least 5 days after administration of such agents.
Rotavirus testing by enzyme immunoassay (EIA) will automatically be carried out on all samples submitted on patient’s under 5 years of age.
Cryptosporidium and Giardia testing by EIA will automatically be carried out on patients with a travel history, appropriate clinical details and liquid stool samples.
Specimen types you should send:
The specimen of choice is diarrheal stool. (Please note that some patients may have taken anti-diarrheal treatments).
A rectal swab is only recommended and permissible for infants.
A single specimen of diarrheal stool should suffice to find any routinely screened for bacterial pathogen, including Salmonella, Shigella, Campylobacter and E.coli species.
How to Collect the Sample
Faecal material is placed into the depicted container with the aid of the plastic spoon. Enough sample to fill one third of the pot should be provided. Ensure lid is secure.
Transport
If the specimen is not transported immediately for bacterial culture refrigerate. Shigella species may not survive pH changes that occur in stool samples if not sent without delay.
Please note that stool samples taken to demonstrate trophozoites of Entamoeba histolytica – for diagnosis of amoebic dysentery – must reach the laboratory within 30mins. No time limit for ova, cysts and non-trophozoite forms of parasites.
TB Quantiferon can be used to diagnose active tuberculosis and latent tuberculosis infection (LTBI)
This test is only available on Medical Microbiology Request
For enquires within hours contact Deborah Gascoyne-Binzi on 0113 3923929
Specimen types you should send:
QuantiFERON TB Gold Plus tubes must be used for this investigation. The four tube system consists of the Nil antigen (grey cap), TB1 (green cap), TB2 (yellow cap) and Mitogen (purple cap)
How to Collect the Sample
For each patient collect 1 ml of blood by venepuncture directly into each QuantiFERON – TB Gold Plus tube.
As 1 ml tubes draw blood slowly, keep the tube on the needle for 2-3 seconds, until the tube appears to have completed filling: ensure that the correct volume is drawn.
The black mark on the side of the tube indicates the 1 ml fill volume. If the level of blood is not close to the indicator line, it is recommended to obtain another blood sample. NB Tubes should not be overfilled.
If a “butterfly needle” is used, a “purge” tube should be used to ensure the tubing is filled with blood prior to filling QuantiFERON TB Gold Plus tubes.
Once the blood sample has been taken mix the tubes by shaking vigorously for 5 seconds to ensure the entire surface of the tube has been coated with blood.
Transport of Samples
Samples must not be refrigerated or they will not be valid for testing. Samples must arrive within 16 hours of collection. Samples should be received in Microbiology at LGI by 16:00 Monday to Friday.
On receipt of samples shake each tube vigorously for 5 seconds. Incubate at 37°C for 16 hours as soon as possible in an upright position, and within 16 hours of collection.
Record on the request card that samples have been incubated and transport to Leeds as soon as possible after this time.
External Referring Laboratories
On receipt of samples shake each tube vigorously for 5 seconds. Incubate at 37°C for 16 hours as soon as possible in an upright position, and within 16 hours of collection.
Record on the request card that samples have been incubated and transport to Leeds as soon as possible after this time.
- Samples must be obtained under sterile conditions. If small sample add sterile saline to prevent desiccation
- Do not send whole amputated tissue. Suspected infected portion should be sent
- Specimen should be transported to the laboratory as soon as possible. Larger pieces of tissue may maintain viability of organisms longer. If delayed transport refrigerate sample. Delays over 48 hours are undesirable
- If Acid and Alcohol fast bacilli (AAFB) are suspected ensure sample is labelled as high risk and that this request is explicit on the form
- If an urgent gram stain is required please contact the laboratory. Gram stain is not routinely performed on non-sterile tissue, diabetic feet or prosthetic joint samples. Gram stain will be available within 24 hours or sooner if requested as urgent
How to Collect the Sample
- Disinfect the skin site thoroughly prior to puncture or incision. If necessary use sterile gloves and sterile drapes around the incision or puncture site
- Guidance on taking wound swabs
- A guide on the use of liquid swabs
To help the Laboratory tremendously A good history on the request would be of great benefit (e.g. “not on antibiotics….urinalysis positive” or “on 3 days of trimethoprim still urinary symptoms”) Simply recording dipstick results without other clinical information is NOT acceptable.
Microscopy and Culture
Urine should be sent in boric acid preservative, filled to the line marked on the container.
Suitable samples for test are: Mid-stream urine, urine collected from urinary catheter port (not bag bladder washout samples), cystoscopy urine, nephrostomy tube urines, bag urine from infants, supra-pubic aspirate.
Test is indicated for investigation of urinary tract infection
Instructions for New Collection Cups and Tubes (541kB pdf)
Small Samples
e.g. in paediatric patients, 5ml bottles should be used. This prevents the concentration of the preservative affecting the result.
Sterile Universal Containers should be sent for:
Early morning urine, samples required from 3 consecutive days for mycobacterial culture.
Pregnancy testing; early morning sample recommended
Antigen detection tests e.g. legionella Virology testing e.g. BK virus, CMV
Urine for Schistosomiasis must be collected between 10am and 2pm after a period of activity. Minimum 10mls Alternatively a 24h collection of terminal samples of urine may be obtained.
How to collect a sample
Collect 20ml of urine if using a red topped universal container, this should fill up to the fill line. If less than 20ml is collected the boric acid in the container may inhibit the growth of some bacteria. Urine can be collected from a variety of sites (Mid-stream specimen of urine – MSSU – , catheter urine, bag urine from young children, nephrostomy tube urine, suprapubic aspirates of urines etc).
MSSU samples are prone to contamination and the patient has to be instructed to cleanse the area of the urethra thoroughly with soap and water before collecting after voiding the initial portion of urine. This reduces the contamination rate greatly.
Indicators of contamination are presence of epithelial cells or absence of white cells or pyuria. The cell count is found on the final report.
Transport
If the specimen is not transported immediately for bacterial culture, refrigerate.
Delay in transit can lead to a false positive result.
Types of Specimens
Serum Samples
Serum Samples are required for antibody detection tests IgG/IgM
Take sample in serum gel tube or serum separator – min 5 mls
Adult: Red top, yellow ring – ensure tube is filled to line. Separate samples should be sent for blood sciences requests.
Paediatrics: Red top, white ring. Multiple tests may require multiple bottles.
Do not use tubes with additives
Plasma Samples
Plasma Samples are required for molecular PCR tests
Adults: Lavender top, black ring, ensure tube is filled to line. Multiple tests require additional tubes.
Paediatrics: Lavender top, white ring
Samples for CMV, EBV, Adenovirus PCR tests need to be in the lab by 9:30am (Mon to Sat) for same day testing.
Viral swab sample – Copan flocked swabs
Pink top Copan Swabs. Suitable for Skin swabs, eye swabs, throat swabs, nose swabs, vesicle fluid swabs for PCR.
Respiratory Sample
Nasopharyngeal aspirate BAL or Tracheal Aspirate in Sterile Universal. Samples should reach the laboratory by 9:30am for same day testing (NB: Respiratory testing at weekends is normally only on Sundays except during peak influenza season).
CSF Sample
Send separate sample and request from other investigations in a sterile Universal. Suitable for PCR testing.
Faeces sample
Samples for faecal virology will not be routinely tested in all patients. Indicated for immunocompromised patients and suspected community acquired outbreaks. Suitable for PCR testing.
Tissue Sample
If small biopsy or aspirate sample, moisten with sterile saline. Send in sterile universal. Suitable for PCR testing.
Urine Sample
Urine samples for virology should be sent in sterile containers,do not use containers with boric acid preservative.
Transport
Samples should reach the laboratory within 24 hrs. If this is not possible refrigerate.
HIV and Hepatitis Viral Load samples must be centrifuged within 24 hours of the sample been taken so should be sent without delay. External users of this service can send serum samples instead of whole blood if transport is likely to be delayed.
TB QuantiFERON tests and T spot should not be refrigerated and must be received within 16 hours of collection. See sampling for TB QuantiFERON tests and T spot on our tests and tubes site.
Viruses Associated by Clinical Syndrome
| Clinical syndrome/details | Viruses associated | Specimen and comments | Test method |
|---|---|---|---|
| Conjunctivitis/Keratitis/ Retinitis | Herpes Simplex Virus (HSV) Adenovirus Varicella-zoster virus (VZV) Enterovirus Cytomegalovirus (CMV) | Viral Eye Swab | PCR |
| Mucous or cutaneous membranes – vesicular or ulcerative lesions | Herpes Simplex Virus (HSV)AdenovirusVaricella-zoster virus (VZV)Enterovirus | Viral Swab sample, skin lesions, mouth, lip samples | PCR |
| Maculopapular rash | Measles Parvovirus B19 Enterovirus Rubella Syphilis | Various samples see test repertoire | PCR and serology |
| Respiratory Infection | Adenovirus Influenza viruses A and B Respiratory Syncytial Virus (RSV) Parainfluenza viruses 1-4 Metapneumovirus Rhinovirus | NPA BAL Tracheal Aspirate Nose and Throat swabs in VTM. | PCR |
| Exposure to Blood Borne Virus | Hepatitis B surface antigen Hepatitis C antibody HIV | Serum sample Acute recipient samples will be stored only. If recipient post 3 month please include hepatitis B vaccination history in clinical details. Donor samples should indicate known infection if applicable. | Serology |
| Meningitis and Encephalitis | HSV VZV Adenovirus Enterovirus. In addition for immunocompromised patients: CMV EBV JC. | CSF sample Faeces samples for enterovirus only | PCR |
| Myocarditis and Pericarditis | Enterovirus Parvovirus Influenza A&B (seasonal) | EDTA sample Faeces sample for enterovirus only Respiratory samples | PCR |
| Haemorrhagic cystitis | AdenovirusCMVBK virus | Urine Sample | PCR |
| Gastroenteritis | Norovirus Rotavirus` Adenovirus* Sapovirus* Astrovirus* | Faeces Sample* Tested on patients <5 years, all immunocompromised and immunosuppressed. External users should specifically request extended testing if required | PCR |
| Acute Hepatitis Jaundice Abnormal LFTs Hepatomegaly Dark urine/pale stools | Hepatitis A, B, C, E | Serum sample | Serology |
| Viral Neonatal Fever | HSVAdenovirusEnterovirusCMVEBVVZV | EDTA sampleFaeces sample for enterovirus only | PCR |
| Viral Fever > 3 months | AdenovirusEpstein Barr VirusCMV | EDTA sample | PCR |
| Viral Rash | Herpes SimplexVaricella ZosterAdenoEnterovirus. | UTM sample of affected siteFaeces sample for enterovirus only | PCR |
Uncertainty in Microbiology Tests
In laboratory testing there are potential “uncertainties” that may affect test results (for example, specimen not collected correctly, presence of antimicrobials, biological variation)
Additionally factors within the laboratory may lead to variation (for example, incubation times, time to processing). The Microbiology laboratory has measures in place to minimize the level of uncertainty and this is reflected by the Quality Assurance processes in place.
Results provided by the laboratory are representative of the sample tested and must be considered against clinical presentation. There are a number of factors that may affect the quality and validity of a result that are outside of the laboratories control:
| Factors that may affect results | Mitigating actions |
|---|---|
| Delays in transportation of samples. Isolation or quantification of some microorganisms may be affected by prolonged storage of a sample. | Ensure samples are sent as soon as possible via transport (external) or airtube (internal). If problems with transport occur contact the laboratory. Notify the laboratory of any urgent samples. Ensure the date of collection is clearly marked so any possible decrease in quality can be noted on the report. |
| Incorrect storage conditions for sample type e.g. TB QuantiFERON and T spot tests must not be refrigerated and samples must be received within 16 hours | User manual provides full information on sample collection and transport information. Special blue bags are provided to allow laboratory staff to easily identify these samples. See website: How to sample TB QuantiFERON |
| Inappropriate sample type sent for investigationsExamples:Copan liquid swabs used for Chlamydia or Viral PCRPlain universals used for urine cultureFormalin pots used for tissue samples for microbiological cultureBlood tubes with preservatives sent for serology tests | Refer to user guide and tests and tubes website. Contact laboratory if unsure of requirements. Print specimen user guides. |
| Insufficient volume of sample sent | Refer to user guide and tests and tubes website. Contact laboratory if unsure of requirements. |
| Out of Date specimen container used | Do not overstock areas. Practice stock rotation. Check expiry dates before use. |
| Contamination of samples | Always use sterile containers. Maintain aseptic technique. Where appropriate refer to sampling guidance on Leeds Healthcare Pathways. |
| Sample Quality | Maintain aseptic technique. Where appropriate refer to sampling guidance on Leeds Healthcare Pathways. Refer to user guide and tests and tubes website. |
| Insufficient Clinical Details – tests may often be designated within the laboratory based on the clinical details provided. Tests may be missed if there is not enough information | Complete requests as fully as possible. |
| Presence of antimicrobials | Where possible take samples before therapy is started. State any antimicrobials in use on the request form. |
| Inherent Factors e.g. Age, gender, congenital immunosuppression | Advice on the need to always provide full clinical details. Medical authorisation of results. |
Bacterial PCR Request Form
Download the Bacterial PCR Request Form